Vacuum aspiration
| Background | |
| Abortion type | Surgical |
| First use | China 1958 and UK 1967[1] |
| Gestation | 3-12 weeks |
| Usage | |
| Figures are combined usage of MVA and EVA. | |
| Sweden | 42.7% (2005) |
| UK: Eng. & Wales | 64% (2006) |
| United States | 88.3% (2003) |
| Infobox references | |
Vacuum or suction aspiration uses aspiration to remove uterine contents through the cervix. It may be used as a method of induced abortion, a therapeutic procedure used after miscarriage, or a procedure to obtain a sample for endometrial biopsy. The rate of infection is lower than any other surgical abortion procedure at 0.5%.[2]
Some sources may use the terms dilation and evacuation[3] or "suction" dilation and curettage[4] to refer to vacuum aspiration, although those terms are normally used to refer to distinct procedures.
History
Vacuuming as a means of removing the uterine contents, rather than the previous use of a hard metal curette, was pioneered in 1958 by Drs Wu Yuantai and Wu Xianzhen in China,[5] but their paper was only translated into English on the fiftieth anniversary of the study that "ultimately led to the technique becoming the world’s most common and safest obstetric procedure".[1]
In Canada, the method was pioneered and improved on by Henry Morgentaler, achieving a complication rate of 0.48% and no deaths in over 5,000 cases.[6] He was the first doctor in North America to use the technique, which he trained other doctors to use.[7]
Dorothea Kerslake introduced the method into the United Kingdom in 1967 and published a study in the United States that further spread the technique.[1][8]
Harvey Karman in the United States refined the technique in the early 1970s with the development of the Karman cannula, a soft, flexible cannula that avoided the need for initial cervical dilatation and so reduced the risks of puncturing the uterus.[1]
Clinical uses
Vacuum aspiration may be used as a method of induced abortion, as a therapeutic procedure after miscarriage, to aid in menstrual regulation, and to obtain a sample for endometrial biopsy.[9] It is also used to terminate molar pregnancy.[10]
When used as a miscarriage treatment or an abortion method, vacuum aspiration may be used alone or with cervical dilation anytime in the first trimester (up to 12 weeks gestational age). For more advanced pregnancies, vacuum aspiration may be used as one step in a dilation and evacuation procedure.[11] Vacuum aspiration is the procedure used for almost all first-trimester abortions in many countries.[9]
Procedure
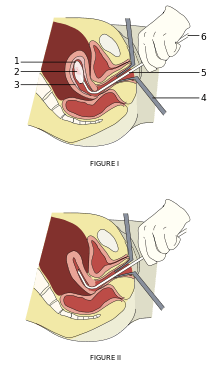
1: Amniotic sac
2: Embryo
3: Uterine lining
4: Speculum
5: Vacurette
6: Attached to a suction pump
Figure I is before aspiration of amniotic sac and embryo, and Figure II is after aspiration with the instrument still inside the uterus.
Vacuum aspiration is an outpatient procedure that generally involves a clinic visit of several hours.[12] The procedure itself typically takes less than 15 minutes.[2] Suction is created with either an electric pump (electric vacuum aspiration or EVA) or a manual pump (manual vacuum aspiration or MVA). A hand-held 25cc or 50cc syringe can function as a manual pump.[13] Both methods use the same level of suction, and so can be considered equivalent in terms of effectiveness and safety.[14]
The clinician may first use a local anesthetic to numb the cervix. Then, the clinician may use instruments called "dilators" to open the cervix, or sometimes medically induce dilation with drugs. Finally, a sterile cannula is inserted into the uterus and attached via tubing to the pump. The pump creates a vacuum which empties uterine contents.[2]
After a procedure for abortion or miscarriage treatment, the tissue removed from the uterus is examined for completeness.[2] Expected contents include the embryo or fetus, as well as the decidua, chorionic villi, amniotic fluid, amniotic membrane and other tissue.
Post-treatment care includes brief observation in a recovery area and a follow-up appointment approximately two weeks later. These would tend to include tests for infection in case any biological material was not properly removed.
Additional medications used in vacuum aspiration include NSAID analgesics that may be started already the day before the procedure, as well as misoprostol the day before for cervical ripening.[15]
Advantages over dilation and curettage
Dilation and curettage (D&C), also known as sharp curettage, was once the standard of care in situations requiring uterine evacuation. However, vacuum aspiration has a number of advantages over D&C and has largely replaced D&C in many settings.[16][17]
Vacuum aspiration may be used earlier in pregnancy than dilation and curettage (D&C). Manual vacuum aspiration is the only surgical abortion procedure available earlier than the 6th week of pregnancy.[2] Vacuum aspiration has lower rates of complications when compared to D&C.[14]
Vacuum aspiration - especially manual vacuum aspiration - is significantly cheaper than D&C. The equipment needed for vacuum aspiration costs less than a curette set. While D&C is generally provided only by physicians, vacuum aspiration may be performed by advanced practice clinicians such as physician assistants and midwives.[18]
Manual vacuum aspiration does not require electricity and so can be provided in locations that have unreliable electrical service or none at all. Manual vacuum aspiration also has the advantage of being quiet, without the noise of an electric vacuum pump.[18]
Complications
When used for uterine evacuation, vacuum aspiration is 98% effective in removing all uterine contents.[14] Retained products of conception require a second aspiration procedure. This is more common when the procedure is performed very early in pregnancy, before 6 weeks gestational age.[2]
Other complications occur at a rate of less than 1 per 100 procedures and include excessive blood loss, infection, injury to the cervix or uterus,[14] including perforation, and uterine adhesions.[19]
References
- 1 2 3 4 Coombes R (14 June 2008). "Obstetricians seek recognition for Chinese pioneers of safe abortion". BMJ. BMJ. 336 (7657): 1332–3. PMC 2427078
 . PMID 18556303. doi:10.1136/bmj.39608.391030.DB.
. PMID 18556303. doi:10.1136/bmj.39608.391030.DB. - 1 2 3 4 5 6 "Manual and vacuum aspiration for abortion". A-Z Health Guide from WebMD. October 2006. Retrieved February 18, 2006.
- ↑ "Miscarriage". EBSCO Publishing Health Library. Brigham and Women's Hospital. January 2007. Retrieved 2007-04-07.
- ↑ "What Every Pregnant Woman Needs to Know About Pregnancy Loss and Neonatal Death". The Unofficial Guide to Having a Baby. WebMD. 2004-10-07. Retrieved 2007-04-29.
- ↑ Wu Y, Wu X (1958). "A report of 300 cases using vacuum aspiration for the termination of pregnancy" (PDF). Chinese Journal of Obstetrics and Gynaecology. 336: 447–9. PMC 2427078 . PMID 18556303. doi:10.1136/bmj.39608.391030.DB.
- ↑ Morgentaler H H (1973). "Report on 5641 outpatient abortions by vacuum suction curettage". CMAJ. 109 (12): 1202–5. PMC 1947080 . PMID 4758593.
- ↑ Morgentaler H (May–Jun 1989). "Alan F. Guttmacher lecture". Am J Gynecol Health. 3 (3-S): 38–45. PMID 12284999.
- ↑ Kerslake D, Casey D (July 1967). "Abortion induced by means of the uterine aspirator". Obstet Gynecol. 30 (1): 35–45. PMID 5338708.
- 1 2 Baird, Traci L.; Susan K. Flinn (2001). "Manual Vacuum Aspiration: Expanding women's access to safe abortions services" (PDF). Ipas: 3. Retrieved 2008-01-28., which cites:
- Greenslade, Forrest; Janie Benson; Judith Winkler; Victoria Henderson; Ann Leonard (1993). "Summary of clinical and programmatic experience with manual vacuum aspiration". Advances in Abortion Care. 3 (2).
- ↑ "Managing complications in pregnancy and childbirth: A guide for doctors and midwives". World Health Organization. 2003. Retrieved 2006-09-14.
- ↑ Baird (2001), pp. 4-5,14 (sidebars and information box).
- ↑ Baird (2001), p. 10 (table).
- ↑ http://contraception.about.com/od/unplannedpregnancy/p/AspirationProcedure.htm
- 1 2 3 4 Baird (2001), pp. 4-6.
- ↑ Table 2 in: Allison JL, Sherwood RS, Schust DJ (2011). "Management of first trimester pregnancy loss can be safely moved into the office". Rev Obstet Gynecol. 4 (1): 5–14. PMC 3100102 . PMID 21629493.
- ↑ Baird (2001), p. 2.
- ↑ https://www.sharecare.com/health/abortion/what-is-vacuum-aspiration
- 1 2 Baird (2001), pp. 5,8-13.
- ↑ Dalton, VK; Saunders NA; Harris LH; Williams JA; Lebovic DI (June 2006). "Intrauterine adhesions after manual vacuum aspiration for early pregnancy failure". Fertility and Sterility. 85 (6): 1823.e1–3. PMID 16674955. doi:10.1016/j.fertnstert.2005.11.065.