Suxamethonium chloride
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | /ˌsʌksɪnɪlˈkoʊlin/ |
| Trade names | Quelicin, Anectine |
| AHFS/Drugs.com | Monograph |
| Pregnancy category | |
| Routes of administration | intravenous, intramuscular |
| ATC code | |
| Legal status | |
| Legal status | |
| Pharmacokinetic data | |
| Bioavailability | NA |
| Metabolism | By pseudocholinesterase, to succinylmonocholine and choline |
| Onset of action | 30-60 sec (IV), 2-3 min (IM) |
| Duration of action | < 10 min (IV), 10-30 min (IM) |
| Excretion | Kidney (10%) |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| Chemical and physical data | |
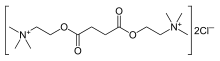
| Formula | C14H30N2O4 |
| Molar mass | 290.399 g/mol |
| 3D model (JSmol) | |
| |
| |
| | |
Suxamethonium chloride, also known as suxamethonium or succinylcholine, is a medication used to cause short-term paralysis as part of general anesthesia.[1] This is done to help with tracheal intubation or electroconvulsive therapy.[1] It is given either by injection into a vein or muscle. When used in a vein onset of action is generally within one minute and effects last for up to 10 minutes.[2]
Common side effects include low blood pressure, increased saliva production, muscle pain, and rash.[2] Serious side effects include malignant hyperthermia and allergic reactions.[3] It is not recommended in people who are at risk of high blood potassium or a history of myopathy.[1] Use during pregnancy appears to be safe for the baby.[4] Suxamethonium is in the neuromuscular blocker family of medications and is of the depolarizing type. It works by blocking the action of acetylcholine on skeletal muscles.[2]
Suxamethonium was described as early as 1906 and came into medical use in 1951.[5] It is on the World Health Organization's List of Essential Medicines, the most effective and safe medicines needed in a health system.[6] Suxamethonium is available as a generic medication.[2] The wholesale cost in the developing world is about 0.45 to 1.31 USD a dose.[7] It may colloquially be referred to as "sux".[5]
Medical uses

Its medical uses are limited to short-term muscle relaxation in anesthesia and intensive care, usually for facilitation of endotracheal intubation. It is perennially popular in emergency medicine because it has the fastest onset and shortest duration of action of all muscle relaxants. The former is a major point of consideration in the context of trauma care, where endotracheal intubation may need to be completed very quickly. The latter means that, should attempts at endotracheal intubation fail and the person cannot be ventilated, there is a prospect for neuromuscular recovery and the onset of spontaneous breathing before low blood oxygen levels occurs. It is better than rocuronium in making it easy to intubate.[8]
Suxamethonium is also commonly used as the sole muscle relaxant during electroconvulsive therapy, favoured for its short duration of action.
Suxamethonium is quickly degraded by plasma butyrylcholinesterase and the duration of effect is usually in the range of a few minutes. When plasma levels of butyrylcholinesterase are greatly diminished or an atypical form is present (an otherwise harmless inherited disorder), paralysis may last much longer, as is this the case in liver failure or in neonates.[9]
It is recommended that the vials be stored at a temperature between 2°-8°C, for optimum action. This is all the more important in temperate and tropical countries where room temperatures can go as high as 30°C.
Side effects
Side effects include malignant hyperthermia, muscle pains, acute rhabdomyolysis with high blood levels of potassium,[9] transient ocular hypertension, constipation[10] and changes in cardiac rhythm, including slow heart rate, and cardiac arrest. In people with neuromuscular disease or burns, an injection of suxamethonium can lead to a large release of potassium from skeletal muscles, potentially resulting in cardiac arrest. Conditions having susceptibility to suxamethonium-induced high blood potassium are burns, closed head injury, acidosis, Guillain–Barré syndrome, cerebral stroke, drowning, severe intra-abdominal sepsis, massive trauma, myopathy, and tetanus.
Suxamethonium does not produce unconsciousness or anesthesia, and its effects may cause considerable psychological distress while simultaneously making it impossible for a patient to communicate. Therefore, administration of the drug to a conscious patient is contraindicated.
Hyperkalemia
The side effect of high blood potassium may occur because the acetylcholine receptor is propped open, allowing continued flow of potassium ions into the extracellular fluid. A typical increase of potassium ion serum concentration on administration of suxamethonium is 0.5 mmol per liter. The increase is transient in otherwise healthy patients. The normal range of potassium is 3.5 to 5 mEq per liter. High blood potassium does not generally result in adverse effects below a concentration of 6.5 to 7 mEq per liter. Therefore, the increase in serum potassium level is usually not catastrophic in otherwise healthy patients.
Severely high blood levels of potassium will cause changes in cardiac electrophysiology, which, if severe, can result in asystole.
Malignant hyperthermia
Malignant hyperthermia (MH) from suxamethonium administration can result in a drastic and uncontrolled increase in skeletal muscle oxidative metabolism. This overwhelms the body's capacity to supply oxygen, remove carbon dioxide, and regulate body temperature, eventually leading to circulatory collapse and death if not treated quickly.
Susceptibility to malignant hyperthermia is often inherited as an autosomal dominant disorder, for which there are at least six genetic loci of interest, the most prominent being the ryanodine receptor gene (RYR1). MH susceptibility is phenotype and genetically related to central core disease (CCD), an autosomal dominant disorder characterized both by MH symptoms and by myopathy. MH is usually unmasked by anesthesia, or when a family member develops the symptoms. There is no simple, straightforward test to diagnose the condition. When MH develops during a procedure, treatment with dantrolene sodium is usually initiated; dantrolene and the avoidance of suxamethonium administration in susceptible people have markedly reduced the mortality from this condition.
Apnea
The normal short duration of action of suxamethonium is due to the rapid metabolism of the drug by non-specific plasma cholinesterases. However plasma cholinesterase activity is reduced in some people due to either genetic variation or acquired conditions, this results in a prolonged duration of neuromuscular block. Genetically ninety six percent of the population have a normal (Eu:Eu) genotype and block duration, however some people have abnormal genes (Ea, Es, Ef) which can be found in varying combinations with the Eu gene or other abnormal genes (see Pseudocholinesterase deficiency). All will result in a longer duration of block from 20 minutes up to several hours. Acquired factors that affect plasma cholinesterase activity include pregnancy, liver disease, kidney failure, heart failure, thyrotoxicosis, cancer and a number of other drugs.[11]
If unrecognized by a clinician it could lead to awareness if anesthesia is discontinued whilst still paralyzed or hypoxemia (and potentially fatal consequences) if artificial ventilation is not maintained. Normal treatment is to maintain sedation and ventilate the patient on an intensive care unit until muscle function has returned. Blood testing for cholinesterase function can be performed.
Mivacurium, a non-depolarizing neuromuscular blocking drug, is also metabolized via the same route with a similar clinical effect in patients deficient in plasma cholinesterase activity.
Deliberate induction of conscious apnea using this drug led to its use as a form of aversion therapy in the 1960s and 1970s in some prison and institutional settings.[12][13][14] This use was discontinued after negative publicity concerning the terrifying effects on subjects of this treatment and ethical questions about the punitive use of painful aversion.
Mechanism of action
There are two phases to the blocking effect of suxamethonium.
Phase 1 block
Phase 1 blocking has the principal paralytic effect. Binding of suxamethonium to the nicotinic acetylcholine receptor results in opening of the receptor's monovalent cation channel; a disorganized depolarization of the motor end-plate occurs and calcium is released from the sarcoplasmic reticulum.
In normal skeletal muscle, acetylcholine dissociates from the receptor following depolarization and is rapidly hydrolyzed by the enzyme acetylcholinesterase. The muscle cell is then ready for the next signal.
Suxamethonium has a longer duration of effect than acetylcholine, and is not hydrolyzed by acetylcholinesterase. By maintaining the membrane potential above threshold, it does not allow the muscle cell to repolarize. When acetylcholine binds to an already depolarized receptor, it cannot cause further depolarization.
Calcium is removed from the muscle cell cytoplasm independent of repolarization (depolarization signaling and muscle contraction are independent processes). As the calcium is taken up by the sarcoplasmic reticulum, the muscle relaxes. This explains muscle flaccidity rather than tetany following fasciculations.
The results are membrane depolarization and transient fasciculations, followed by paralysis.
Phase 2 block
This phase is not abnormal and is a part of its mechanism of action. It is caused by the blood concentration of suxamethonium exceeding the therapeutic window. Desensitization occurs at the nerve terminal, and the myocyte becomes less sensitive to acetylcholine; the membrane repolarizes and cannot be depolarized again.
Chemistry
Suxamethonium is an odorless, white crystalline substance. Aqueous solutions have a pH of about 4. The dihydrate melts at 160 °C, whereas the anhydrous melts at 190 °C. It is highly soluble in water (1 gram in about 1 mL), soluble in ethyl alcohol (1 gram in about 350 mL), slightly soluble in chloroform, and practically insoluble in ether. Suxamethonium is a hygroscopic compound.[15] The compound consists of two acetylcholine molecules that are linked by their acetyl groups. It can also be viewed as a central moiety of succinic acid with two choline moieties, one on each end.
History
Suxamethonium was first discovered in 1906 by Reid Hunt and René de M. Taveau. When studying the drug, animals were given curare and thus they missed the neuromuscular blocking properties of suxamethonium. Instead in 1949 an Italian group led by Daniel Bovet was first to describe succinylcholine induced paralysis. The clinical introduction of suxamethonium was described in 1951 by several groups. Papers published by Stephen Thesleff and Otto von Dardel in Sweden are important but also to be mentioned is work by Bruck, Mayrhofer and Hassfurther in Austria, Scurr and Bourne in UK, and Foldes in America.[16]
Society and culture
Suxamethonium has been described as a "perfect poison" for murder, and has been used by criminals in murders.[17] Suxamethonium chloride is the INN.
Other animals
It is sometimes used in combination with pain medications and sedatives for euthanasia and immobilization of horses.
References
- 1 2 3 WHO Model Formulary 2008 (PDF). World Health Organization. 2009. pp. 426–428. ISBN 9789241547659. Retrieved 8 December 2016.
- 1 2 3 4 "Succinylcholine Chloride". The American Society of Health-System Pharmacists. Retrieved 8 December 2016.
- ↑ "Anectine Injection - Summary of Product Characteristics (SPC) - (eMC)". www.medicines.org.uk. 12 January 2016. Retrieved 16 December 2016.
- ↑ "Prescribing medicines in pregnancy database". Therapeutic Goods Administration (TGA). 16 December 2016. Retrieved 16 December 2016.
- 1 2 Lee, C; Katz R. (2009). "Clinical implications of new neuromuscular concepts and agents: So long, neostigmine! So long, sux!". J Crit Care. 24 (1): 43–9. PMID 19272538. doi:10.1016/j.jcrc.2008.08.009.
- ↑ "WHO Model List of Essential Medicines (19th List)" (PDF). World Health Organization. April 2015. Retrieved 8 December 2016.
- ↑ "Suxamethonium Cl". International Drug Price Indicator Guide. Retrieved 8 December 2016.
- ↑ Tran, DT; Newton, EK; Mount, VA; Lee, JS; Wells, GA; Perry, JJ (29 October 2015). "Rocuronium versus succinylcholine for rapid sequence induction intubation.". The Cochrane database of systematic reviews. 10: CD002788. PMID 26512948. doi:10.1002/14651858.CD002788.pub3.
- 1 2 Rod J. Flower (25 March 2011). Rang and Dale's Pharmacology. Elsevier Science Health Science Division. ISBN 978-0-7020-3471-8.
- ↑ DiPiro, Joseph, et al. Pharmacotherapy: A Pathophysiologic Approach. 6th ed. McGraw-Hill, 2005:685.
- ↑ Pharmacology for Anaesthesia and Intensive Care. 2nd Edition. Peck, Hill & Williams
- ↑ Reimring, MJ; Morgan, SW; Bramwell, PF (1970). "Succinylcholine as a modifier of acting-out behavior". Clinical Medicine. 77 (7): 28.
- ↑ von Hoffman, Nicholas (1972) "A Bit of 'Clockwork Orange,' California-Style." Washington Post April 5, 1972. mirror
- ↑ Sansweet RJ. (1975) The Punishment Cure. New York: Mason/Charter. ISBN 0-88405-118-8.
- ↑ Gennaro, Alfonso. Remington: The Science and Practice of Pharmacy, 20th ed. Lippincott Williams & Wilkins, 2000:1336.
- ↑ Dorkins, HR (Apr 1982). "Suxamethonium-the development of a modern drug from 1906 to the present day.". Medical History. 26 (2): 145–68. PMC 1139149
 . PMID 7047939. doi:10.1017/S0025727300041132.
. PMID 7047939. doi:10.1017/S0025727300041132. - ↑ Jayfk, Rubidium (29 May 2012). "The History Of Sux, The World's Most Discrete Murder Weapon". gizmodo.com.au. Retrieved 17 December 2015.