Sleep deprivation
| Sleep deprivation | |
|---|---|
.png) | |
| Minor dark circles, in addition to a hint of eye bags - a combination suggestive of minor sleep deprivation. | |
| Specialty | Sleep medicine |
Sleep deprivation is the condition of not having enough sleep; it can be either chronic or acute. A chronic sleep-restricted state can cause fatigue, daytime sleepiness, clumsiness and weight loss or weight gain.[1] It adversely affects the brain and cognitive function.[2] However, in a subset of cases sleep deprivation can, paradoxically, lead to increased energy and alertness and enhanced mood; it has even been used as a treatment for depression (see below).[3][4]
Few studies have compared the effects of acute total sleep deprivation and chronic partial sleep restriction.[2] Complete absence of sleep over long periods has not been seen in humans (unless they suffer from fatal familial insomnia); it appears that brief microsleeps cannot be avoided.[5] Long-term total sleep deprivation has caused death in lab animals.[6]
Physiological effects
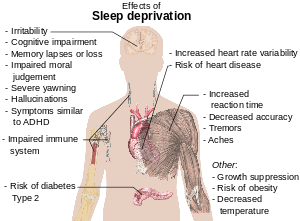
Generally, sleep deprivation may result in:[7][8]
- aching muscles[9]
- confusion, memory lapses or loss[8][10]
- depression[10]
- development of false memory
- hand tremor[11]
- headaches
- malaise
- stye
- periorbital puffiness, commonly known as "bags under eyes" or eye bags
- increased blood pressure[12][13]
- increased stress hormone levels[13]
- increased risk of diabetes[13]
- increased risk of fibromyalgia[14]
- irritability[7]
- nystagmus (rapid involuntary rhythmic eye movement)[15]
- obesity[13]
- seizures[16]
- temper tantrums in children[7]
- yawning[7]
- mania[17]
- symptoms similar to:
Diabetes
It has been suggested that people experiencing short-term sleep restrictions, process glucose more slowly than individuals receiving a full 8 hours of sleep, increasing the likelihood of developing type 2 diabetes.[19] In 2005, a study of over 1400 participants showed that participants who habitually slept few hours were more likely to have associations with type 2 diabetes.[20] However, because this study was merely correlational, the direction of cause and effect between little sleep and diabetes is uncertain. The authors point to an earlier study which showed that experimental rather than habitual restriction of sleep resulted in impaired glucose tolerance (IGT).[21] Sleep deprivation can cause insulin resistance in the body, triggering the onset of early diabetes.[22]
On the brain
Sleep deprivation can adversely affect the brain and cognitive function.[23] A 2000 study, by the UCSD School of Medicine and the Veterans Affairs Healthcare System in San Diego, used functional magnetic resonance imaging (fMRI) technology to monitor activity in the brains of sleep-deprived subjects performing simple verbal learning tasks.[24] The study showed that regions of the brain's prefrontal cortex, an area that supports mental faculties such as working memory and logical and practical ("means-ends") reasoning, displayed more activity in sleepier subjects. Researchers interpreted this result as indicating that the brain of the average sleep-deprived subject had to work harder than that of the average non-sleep-deprived subject to accomplish a given task, and from this indication they inferred the conclusion the brains of sleep-deprived subjects were attempting to compensate for adverse effects caused by sleep deprivation.
The temporal lobe, a brain region involved in language processing, was activated during verbal learning in rested subjects but not in sleep-deprived subjects. The parietal lobe, not activated in rested subjects during the verbal exercise, was more active when the subjects were deprived of sleep. Although memory performance was less efficient with sleep deprivation, greater activity in the parietal region was associated with better short term memory.[25]
A 2001 study at the Chicago Medical Institute suggested that sleep deprivation may be linked to serious diseases, such as heart disease and mental illness including psychosis and bipolar disorder.[26] The link between sleep deprivation and psychosis was further documented in 2007 through a study at Harvard Medical School and the University of California at Berkeley. The study revealed, using MRI scans, that sleep deprivation causes the brain to become incapable of putting an emotional event into the proper perspective and incapable of making a controlled, suitable response to the event.[27]
The negative effects of sleep deprivation on alertness and cognitive performance suggest decreases in brain activity and function, primarily in the thalamus, a structure involved in alertness and attention, and in the prefrontal cortex, a region sub-serving alertness, attention, and higher-order cognitive processes.[28] This was the finding of an American study in 2000. Seventeen men in their 20s were tested. Sleep deprivation was progressive with measurements of glucose (absolute regional CMRglu), cognitive performance, alertness, mood, and subjective experiences collected after 0, 24, 48, and 72 h of sleep deprivation. Additional measures of alertness, cognitive performance, and mood were collected at fixed intervals. PET scans were used and attention was paid to the circadian rhythm of cognitive performance.[28]
A noted 2002 University of California animal study indicated that non-rapid eye movement sleep (NREM) is necessary for turning off neurotransmitters and allowing their receptors to "rest" and regain sensitivity which allows monoamines (norepinephrine, serotonin and histamine) to be effective at naturally produced levels. This leads to improved regulation of mood and increased learning ability. The study also found that rapid eye movement sleep (REM) deprivation may alleviate clinical depression because it mimics selective serotonin reuptake inhibitors (SSRIs). This is because the natural decrease in monoamines during REM is not allowed to occur, which causes the concentration of neurotransmitters in the brain, that are depleted in clinically depressed persons, to increase. Sleep outside of the REM phase may allow enzymes to repair brain cell damage caused by free radicals. High metabolic activity while awake damages the enzymes themselves preventing efficient repair. This study observed the first evidence of brain damage in rats as a direct result of sleep deprivation.[29]
Animal studies suggest that sleep deprivation increases stress hormones, which may reduce new cell production in adult brains.[30]
On growth
A 1999 study[31] found that sleep deprivation resulted in reduced cortisol secretion the next day, driven by increased subsequent slow-wave sleep. Sleep deprivation was found to enhance activity on the hypothalamic-pituitary-adrenal axis (which controls reactions to stress and regulates body functions such as digestion, the immune system, mood, sex, or energy usage) while suppressing growth hormones. The results supported previous studies, which observed adrenal insufficiency in idiopathic hypersomnia.
On the healing process
A study conducted in 2005 showed that a group of rats, which were deprived of REM sleep for five days, experienced no significant changes in their ability to heal wounds, compared to a group of rats not deprived of "dream" sleep.[32] The rats were allowed deep (NREM) sleep. However, another study conducted by Gumustekin et al.[33] in 2004 showed sleep deprivation hindering the healing of burns on rats.
On attention and working memory
Among the possible physical consequences of sleep deprivation, deficits in attention and working memory are perhaps the most important;[2] such lapses in mundane routines can lead to unfortunate results, from forgetting ingredients while cooking to missing a sentence while taking notes. Performing tasks that require attention appears to be correlated with number of hours of sleep received each night, declining as function of hours of sleep deprivation.[34] Working memory is tested by such methods as choice-reaction time tasks.[2]
The attentional lapses also extend into more critical domains in which the consequences can be life-or-death; car crashes and industrial disasters can result from inattentiveness attributable to sleep deprivation. To empirically measure the magnitude of attention deficits, researchers typically employ the psychomotor vigilance task (PVT) which requires the subject to press a button in response to a light at random intervals. Failure to press the button in response to the stimulus (light) is recorded as an error, attributable to the microsleeps that occur as a product of sleep deprivation.
Crucially, individuals' subjective evaluations of their fatigue often do not predict actual performance on the PVT. While totally sleep-deprived individuals are usually aware of the degree of their impairment, lapses from chronic (lesser) sleep deprivation can build up over time so that they are equal in number and severity to the lapses occurring from total (acute) sleep deprivation. Chronically sleep-deprived people, however, continue to rate themselves considerably less impaired than totally sleep-deprived participants.[35] Since people usually evaluate their capability on tasks like driving subjectively, their evaluations may lead them to the false conclusion that they can perform tasks that require constant attention when their abilities are in fact impaired.
On driving ability
The dangers of sleep deprivation are apparent on the road; the American Academy of Sleep Medicine (AASM) reports that one in every five serious motor vehicle injuries is related to driver fatigue, with 80,000 drivers falling asleep behind the wheel every day and 250,000 accidents every year related to sleep,[36] though the National Highway Traffic Safety Administration suggests the figure for traffic accidents may be closer to 100,000.[37] The AASM recommends pulling off the road and taking a 15- or 20-minute nap to alleviate drowsiness.[36]
According to a 2000 study published in the British Medical Journal, researchers in Australia and New Zealand reported that sleep deprivation can have some of the same hazardous effects as being drunk.[38] People who drove after being awake for 17–19 hours performed worse than those with a blood alcohol level of 0.05 percent, which is the legal limit for drunk driving in most western European countries and Australia. Another study suggested that performance begins to degrade after 16 hours awake, and 21 hours awake was equivalent to a blood alcohol content of 0.08 percent, which is the blood alcohol limit for drunk driving in Canada, the U.S., and the U.K.[39]
Fatigue of drivers of goods trucks and passenger vehicles have come to the attention of authorities in many countries, where specific laws have been introduced with the aim of reducing the risk of traffic accidents due to driver fatigue. Rules concerning minimum break lengths, maximum shift lengths and minimum time between shifts are common in the driving regulations used in different countries and regions, such as the drivers' working hours regulations in the European Union and hours of service regulations in the United States.
Other effects
In addition, as a result of continuous muscular activity without proper rest time, effects such as cramping are much more frequent in sleep-deprived individuals. Extreme cases of sleep deprivation have been reported to be associated with hernias, muscle fascia tears, and other such problems commonly associated with physical overexertion.
A 2006 study has shown that while total sleep deprivation for one night caused many errors, the errors were not significant until after the second night of total sleep deprivation.[40] However, combining alcohol with acute sleep deprivation results in a trebled rate of driving off the road when using a simulator.[41]
The National Sleep Foundation identifies several warning signs that a driver is dangerously fatigued, including rolling down the window, turning up the radio, trouble keeping eyes open, head-nodding, drifting out of their lane, and daydreaming. At particular risk are lone drivers between midnight and 6:00am.[42]
Sleep deprivation can negatively impact performance in professional fields as well, potentially jeopardizing lives. Due largely to the February 2009 crash of Colgan Air Flight 3407, which killed 50 people and was partially attributed to pilot fatigue, the FAA reviewed its procedures to ensure that pilots are sufficiently rested. Air traffic controllers were under scrutiny when in 2010 there were 10 incidents of controllers falling asleep while on shift. The common practice of turn-around shifts caused sleep deprivation and was a contributing factor to all air traffic control incidents. The FAA reviewed its practices of shift changes and the findings saw that controllers were not well rested.[43] A 2004 study also found medical residents with less than four hours of sleep a night made more than twice as many errors as the 11% of surveyed residents who slept for more than seven hours a night.[44]
Twenty-four hours of continuous sleep deprivation results in the choice of less difficult math tasks without decreases in subjective reports of effort applied to the task. Naturally caused sleep loss affects the choice of everyday tasks such that low effort tasks are mostly commonly selected. Adolescents who experience less sleep show a decreased willingness to engage in sports activities that require effort through fine motor coordination and attention to detail.[45][46]
Great sleep deprivation mimics psychosis: distorted perceptions can lead to inappropriate emotional and behavioral responses.[47]
Astronauts have reported performance errors and decreased cognitive ability during periods of extended working hours and wakefulness as well as due to sleep loss caused by circadian rhythm disruption and environmental factors.[48]
Microsleeps
Microsleeps occur when a person has a significant sleep deprivation. Microsleeps usually last for a few seconds and happen most frequently when a person is trying to stay awake when they are feeling sleepy.[49] The person usually falls into microsleep while doing a monotonous task like driving, reading a book, or staring at a computer.[50] Microsleeps are similar to blackouts and a person experiencing them is not consciously aware that they are occurring.
An even lighter type of sleep has been seen in rats that have been kept awake for long periods of time. In a process known as local sleep, specific localized brain regions went into periods of short (~80 ms) but frequent (~40/min) NREM-like states. Despite the on and off periods where neurons shut off, the rats appeared to be awake, although they performed poorly at tests.[51]
Weight gain and loss
In rats, prolonged, complete sleep deprivation increased both food intake and energy expenditure with a net effect of weight loss and ultimately death.[52] This study hypothesizes that the moderate chronic sleep debt associated with habitual short sleep is associated with increased appetite and energy expenditure with the equation tipped towards food intake rather than expenditure in societies where high-calorie food is freely available.[1]
Several large studies using nationally representative samples suggest that one of the causes of high obesity rates in the United States might be a corresponding decrease in the average number of hours that people are sleeping.[53][54][55] The findings suggest that this might be happening because sleep deprivation could be disrupting hormones that regulate glucose metabolism and appetite.[56]
The association between sleep deprivation and obesity appears to be strongest in young and middle-age adults. Other scientists hold that the physical discomfort of obesity and related problems, such as sleep apnea, reduce an individual's chances of getting a good night's sleep.
Sleep loss is currently proposed to disturb endocrine regulation of energy homeostasis leading to weight gain and obesity. For instance, laboratory sleep deprivation studies in young men have demonstrated that one night of wakefulness (typically found in shift workers) exerts significant effects on the energy balance the next morning, including reduced energy expenditure,[57] enhanced hedonic stimulus processing in the brain underlying the drive to consume food,[58] and overeating that goes beyond satiety.[59] Further recent studies have shown that a reduction of sleep duration to four hours for two consecutive nights has been shown to decrease circulating leptin levels and to increase ghrelin levels, as well as self-reported hunger. Similar endocrine alterations have been shown to occur even after a single night of sleep restriction.
In a balanced order, nine healthy normal-weight men spent three nights in a sleep laboratory separated by at least two weeks: one night with a total sleep time of seven hours, one night with a total sleep time of 4.5 hours, and one night with total sleep deprivation (SD). On a standard symptom-rating scale, subjects rated markedly stronger feelings of hunger after total SD than after seven hours of sleep (3.9 ± 0.7 versus 1.7 ± 0.3; P = 0.020) or 4.5 hours sleep (2.2 ± 0.5; P = 0.041). Plasma ghrelin levels were 22 ± 10% higher after total SD than after seven hours of sleep (0.85 ± 0.06 versus 0.72 ± 0.04 ng mL(−1); P = 0.048) with intermediate levels of the hormone after 4.5 hours sleep (0.77 ± 0.04 ng mL(−1)). Feelings of hunger as well as plasma ghrelin levels are already elevated after one night of SD, whereas morning serum leptin concentrations remain unaffected. Thus, the results provide further evidence for a disturbing influence of sleep loss on endocrine regulation of energy homeostasis, which in the long run may result in weight gain and obesity.[60]
Uses
Scientific study of laboratory animals

In science, sleep deprivation (of rodents, e.g.) is used in order to study the function(s) of sleep and the biological mechanisms underlying the effects of sleep deprivation.
Some sleep deprivation techniques are:
- Gentle handling: during the sleep deprivation period, the animal and its polysomnograph record are continuously observed; when the animal displays sleep electrophysiological signals or assumes a sleep posture, it is given objects to play with and activated by acoustic and, if necessary, tactile stimuli.[61] Although subjective,[62] this technique is used for total sleep deprivation as well as REM or NREM sleep deprivation. This technique often requires polysomnography.
- Single platform: during the sleep deprivation period, the animal is placed on an inverted flower pot, the bottom diameter of which is small relative to the animal's size (usually 7 cm for adult rats). The pot is placed in a large tub filled with water to within 1 cm of the flower pot bottom. The animal is able to rest on the pot and is even able to get NREM sleep, but at the onset of REM sleep, with its ensuing muscular relaxation, it will either fall into the water and clamber back to its pot or will get its nose wet enough to awaken it. Thus, this technique is only useful for studying REM sleep deprivation. This was one of the first scientific methods developed (see Jouvet, 1964[63] for cats[64] and for rodents).
- Multiple platform: in an effort to reduce the elevated stress response induced by the single platform method,[65] researchers developed the "multiple platform" technique of REM sleep deprivation. In this configuration, the animal is placed within a large tank containing multiple platforms, thereby eliminating the movement restriction in the earlier setup.
- Modified multiple platform: modification of the multiple platform method where several animals together experience sleep deprivation (Nunes and Tufik, 1994).
- Pendulum: animals are prevented from entering into REM sleep by allowing them to sleep for only brief periods of time. This is accomplished by an apparatus that moves the animals' cages backwards and forwards in a pendular motion. At the extremes of the motion, the animals experience postural imbalance, forcing them to walk back and forth to retain their balance.[66]
Interrogation
Sleep deprivation can be used as a means of interrogation, which has resulted in court trials over whether or not the technique is a form of torture.[67]
Under one interrogation technique, a subject might be kept awake for several days and when finally allowed to fall asleep, suddenly awakened and questioned. Menachem Begin, the Prime Minister of Israel from 1977 to 1983, described his experience of sleep deprivation as a prisoner of the NKVD in Russia as follows:
In the head of the interrogated prisoner, a haze begins to form. His spirit is wearied to death, his legs are unsteady, and he has one sole desire: to sleep... Anyone who has experienced this desire knows that not even hunger and thirst are comparable with it.[68]
Sleep deprivation was one of the five techniques used by the British government in the 1970s. The European Court of Human Rights ruled that the five techniques "did not occasion suffering of the particular intensity and cruelty implied by the word torture ... [but] amounted to a practice of inhuman and degrading treatment", in breach of the European Convention on Human Rights.[69]
The United States Justice Department released four memos in August 2002 describing interrogation techniques used by the Central Intelligence Agency. They first described 10 techniques used in the interrogations of Abu Zubaydah, described as a terrorist logistics specialist, including sleep deprivation. Memos from May 2005 introduced four more techniques and claimed that the combination of interrogation methods did not constitute torture under United States law.[70]
The question of extreme use of sleep deprivation as torture has advocates on both sides of the issue. In 2006, Australian Federal Attorney-General Philip Ruddock argued that sleep deprivation does not constitute torture.[71] Nicole Bieske, a spokeswoman for Amnesty International Australia, has stated the opinion of her organization thus: "At the very least, sleep deprivation is cruel, inhumane and degrading. If used for prolonged periods of time it is torture."[72]
Depression
Studies show that sleep restriction has some potential in the treatment of depression.[4] Those who suffer from depression tend to have earlier occurrences of REM sleep with an increased number of rapid eye movements; therefore, monitoring patients' EEG and awakening them during occurrences of REM sleep appears to have a therapeutic effect, alleviating depressive symptoms.[73] As many as 60% of patients, when sleep-deprived, show immediate recovery, although most relapse the following night. The effect has been shown to be linked to increases in the brain-derived neurotrophic factor (BDNF).[74] It has been shown that chronotype is related to the effect of sleep deprivation on mood in normal people: those with morningness preference become more depressed following sleep deprivation while those with eveningness preference show an improvement in mood.[75] A comprehensive evaluation of the human metabolome in sleep deprivation in 2014 found that 27 metabolites are increased after 24 waking hours and suggested serotonin, tryptophan, and taurine may contribute to the antidepressive effect.[76]
The incidence of relapse can be decreased by combining sleep deprivation with medication.[77] Many tricyclic antidepressants suppress REM sleep, providing additional evidence for a link between mood and sleep.[78] Similarly, tranylcypromine has been shown to completely suppress REM sleep at adequate doses.
Insomnia
Some common sleep disorders have been shown to respond to cognitive behavioural therapy for insomnia. This involves a controlled regime of "sleep restriction" in order to restore the homeostatic drive to sleep and encourage normal "sleep efficiency".[79]
Causes
Insomnia
Insomnia, one of the six types of dyssomnia, affects 21%-37% of the adult population.[80][81] Many of its symptoms are easily recognizable, including excessive daytime sleepiness; frustration or worry about sleep; problems with attention, concentration, or memory; extreme mood changes or irritability; lack of energy or motivation; poor performance at school or work; and tension headaches or stomach aches.
Insomnia can be grouped into primary and secondary, or comorbid, insomnia.[82][83][84]
Primary insomnia is a sleep disorder not attributable to a medical, psychiatric, or environmental cause.[85] There are three main types of primary insomnia. These include: psychophysiological, idiopathic insomnia, and sleep state misperception (paradoxical insomnia).[82] Psychophysiological insomnia is anxiety-induced. Idiopathic insomnia generally begins in childhood and lasts the rest of a person’s life. It’s suggested that idiopathic insomnia is a neurochemical problem in a part of the brain that controls the sleep-wake cycle, resulting in either under-active sleep signals or over-active wake signals.[86] Sleep state misperception is diagnosed when people get enough sleep but inaccurately perceive that their sleep is insufficient.
Secondary insomnia, or comorbid insomnia, occurs concurrently with other medical, neurological, psychological and psychiatric conditions. Causation is not necessarily implied.[87]
Voluntary
Sleep deprivation can sometimes be self-imposed due to a lack of desire to sleep or the habitual use of stimulant drugs. Sleep deprivation is also self-imposed to achieve personal fame in the context of record-breaking stunts.
Sleep apnea
Sleep apnea (obstructive sleep apnea, OSA) is a collapse of the upper airway during sleep, which reduces airflow to the lungs. It has many serious health outcomes if untreated, but can very often be effectively treated with positive air pressure therapy. Nasal problems such as a deviated septum will shut down the airway and increase swelling in the mucus lining and nasal turbinates. Corrective surgery (septoplasty) will maximise the airflow and correct the feedback loop to the brain which keeps awakening the sufferer so as not to asphyxiate.
Central sleep apnea is repeated stops in breathing during sleep when the brain temporarily stops sending signals to the muscles that control breathing.
Mental illness
The specific causal relationships between sleep loss and effects on psychiatric disorders have been most extensively studied in patients with mood disorders. Shifts into mania in bipolar patients are often preceded by periods of insomnia, and sleep deprivation has been shown to induce a manic state in susceptible individuals. Sleep deprivation may represent a final common pathway in the genesis of mania,[88] and sleep loss is both a precipitating and reinforcing factor for the manic state.
School
The National Sleep Foundation cites a 1996 paper showing that college/university-aged students got an average of less than 6 hours of sleep each night.[89]
In the study, 70.6% of students reported obtaining less than 8 hours of sleep, and up to 27% of students may be at risk for at least one sleep disorder.[90] Sleep deprivation is common in first year college students as they adjust to the stress and social activities of college life.
A study performed by the Department of Psychology at the National Chung Cheng University in Taiwan concluded that freshmen received the least amount of sleep during the week.[91]
In 1997, University of Minnesota research compared students who started school at 7:15 am with those who started at 8:40 am. They found that students who started at 8:40 got higher grades and more sleep on weekday nights than those who started earlier.[37] One in four U.S. high school students admits to falling asleep in class at least once a week.[92]
It is known that during human adolescence, circadian rhythms and therefore sleep patterns typically undergo marked changes. Electroencephalogram (EEG) studies indicate a 50% reduction of deep (stage 4) sleep and a 75% reduction in the peak amplitude of delta waves during NREM sleep in adolescence. School schedules are often incompatible with a corresponding delay in sleep offset, leading to a less than optimal amount of sleep for the majority of adolescents.[93]
Treatment
Several strategies are common in attempting to increase alertness and counteract the effects of sleep deprivation. Caffeine is often used over short periods to boost wakefulness when acute sleep deprivation is experienced; however, caffeine is less effective if taken routinely.[94] Other strategies recommended by the American Academy of Sleep Medicine include prophylactic sleep before deprivation, naps, other stimulants, and combinations thereof. However, the only sure and safe way to combat sleep deprivation is to increase nightly sleep time.[95]
Recovery of cognitive function is accomplished more rapidly after acute total sleep deprivation than after chronic partial sleep restriction.[2] Chronic deprivation is the more common in everyday life. Just one night of recovery sleep can reverse adverse effects of total sleep deprivation. Recovery sleep is more efficient than normal sleep with shorter sleep latency and increased amounts of deep and REM sleep.
Longest periods without sleep
Randy Gardner holds the scientifically documented record for the longest period of time a human being has intentionally gone without sleep not using stimulants of any kind. Gardner stayed awake for 264 hours (11 days), breaking the previous record of 260 hours held by Tom Rounds of Honolulu.[47] LCDR John J. Ross of the U.S. Navy Medical Neuropsychiatric Research Unit later published an account of this event, which became well-known among sleep-deprivation researchers.[47][96][97]
The Guinness World Record stands at 449 hours (18 days, 17 hours), held by Maureen Weston, of Peterborough, Cambridgeshire in April 1977, in a rocking-chair marathon.[96]
Claims of total sleep deprivation lasting years have been made several times,[98][99][100] but none are scientifically verified.[101] Claims of partial sleep deprivation are better documented. For example, Rhett Lamb of St. Petersburg, Florida, was initially reported to not sleep at all, but actually had a rare condition permitting him to sleep only one to two hours per day in the first three years of his life. He had a rare abnormality called an Arnold-Chiari malformation where brain tissue protrudes into the spinal canal and the skull puts pressure on the protruding part of the brain. The boy was operated on at All Children's Hospital in St. Petersburg in May 2008. Two days after surgery he slept through the night.[102][103]
French sleep expert Michel Jouvet and his team reported the case of a patient who was quasi-sleep-deprived for four months, as confirmed by repeated polygraphic recordings showing less than 30 minutes (of stage-1 sleep) per night, a condition they named "agrypnia". The 27-year-old man was suffering from Morvan's fibrillary chorea, a rare disease that leads to involuntary movements, and in this particular case, extreme insomnia. The researchers found that treatment with 5-HTP restored almost normal sleep stages, however some months after this recovery the patient died during a relapse which was unresponsive to 5-HTP. Despite the extreme insomnia, psychological investigation showed no sign of cognitive deficits, except for some hallucinations.[104]
Fatal familial insomnia is a neurodegenerative disease eventually resulting in a complete inability to go past stage 1 of NREM sleep. In addition to insomnia, patients may experience panic attacks, paranoia, phobias, hallucinations, rapid weight loss, and dementia. Death usually occurs between 7 and 36 months from onset.
See also
- Effects of sleep deprivation on cognitive performance
- Narcolepsy
- Polyphasic sleep
- Sleep medicine
- Sleep onset latency
- Wake therapy
- Tony Wright, who claims to hold the world record for sleep deprivation.
- Foreign Correspondent a 1940 film depicting interrogation by sleep deprivation.
References
- 1 2 Taheri S, Lin L, Austin D, Young T, Mignot E; Lin; Austin; Young; Mignot (December 2004). "Short Sleep Duration Is Associated with Reduced Leptin, Elevated Ghrelin, and Increased Body Mass Index". PLoS Med. 1 (3): e62. PMC 535701
 . PMID 15602591. doi:10.1371/journal.pmed.0010062.
. PMID 15602591. doi:10.1371/journal.pmed.0010062. - 1 2 3 4 5 Alhola, Paula; Päivi Polo-Kantola (October 2007). "Sleep deprivation: Impact on cognitive performance". Neuropsychiatr. Dis. Treat. 3 (5): 553–567. PMC 2656292 . PMID 19300585.
Although both conditions [total and partial SD] induce several negative effects including impairments in cognitive performance, the underlying mechanisms seem to be somewhat different.
- ↑ Nykamp K, Rosenthal L, Folkerts M, Roehrs T, Guido P, Roth, T; Rosenthal; Folkerts; Roehrs; Guido; Roth (September 1998). "The effects of REM sleep deprivation on the level of sleepiness/alertness". Sleep. 21 (6): 609–614. PMID 9779520.
- 1 2 Riemann D, Berger M, Voderholzer U; Berger; Voderholzer (July–August 2001). "Sleep and depression - results from psychobiological studies: an overview". Biological Psychology. 57 (1–3): 67–103. PMID 11454435. doi:10.1016/s0301-0511(01)00090-4.
- ↑ Kushida, Clete Anthony (2005). Sleep deprivation. Informa Health Care. pp. 1–2. ISBN 0-8247-5949-4.
- ↑ Rechtschaffen A, Bergmann B; Bergmann (1995). "Sleep deprivation in the rat by the disk-over-water method". Behavioural Brain Research. 69 (1–2): 55–63. PMID 7546318. doi:10.1016/0166-4328(95)00020-T.
- 1 2 3 4 5 "Sleep deprivation". betterhealth.vic.gov.au.
- 1 2 Read, Bryan F. "Sleep Deprivation". St. Paul's School for Girls, Brooklandville, Maryland. Archived from the original on 2008-02-09.
- ↑ Morin, Charles M. (2003). Insomnia. New York: Kluwer Academic/Plenum Publ. p. 28 death. ISBN 0-306-47750-5.
- 1 2 National Institute of Neurological Disorders and Stroke – Brain Basics: Understanding Sleep. ninds.nih.gov
- ↑ Smith, Andrew P. (1992). Handbook of Human Performance. London: Acad. Press. p. 240. ISBN 0-12-650352-4.
- ↑ "The Human Brain – Sleep and Stress". Fi.edu. 27 September 2007. Retrieved 2012-08-13.
- 1 2 3 4 "Harvard Heart Letter examines the costs of not getting enough sleep – Harvard Health Publications". Health.harvard.edu. 31 May 2012. Retrieved 2012-08-13.
- ↑ "The Role of Magnesium in Fibromyalgia". Web.mit.edu. Retrieved 2012-08-13.
- ↑ Citek, K; Ball, B; Rutledge, DA (2003). "Nystagmus testing in intoxicated individuals" (PDF). Optometry. 74 (11): 695–710. PMID 14653658.
- ↑ Epilepsy: A Comprehensive Textbook - Google Books. Books.google.com. Retrieved 2015-01-30.
- ↑ T A Wehr (1991-10-01). "Sleep-loss as a possible mediator of diverse causes of mania". Bjp.rcpsych.org. Retrieved 2015-01-30.
- ↑ Neural Link Between Sleep Loss And Psychiatric Disorders. ts-si.org (24 October 2007)
- ↑ "Sleep and Disease Risk". Healthy Sleep. Harvard Medical School. 2007.
- ↑ Gottlieb DJ; Punjabi NM; Newman AB; Resnick, HE; Redline, S; Baldwin, CM; Nieto, FJ (April 2005). "Association of sleep time with diabetes mellitus and impaired glucose tolerance". Arch. Intern. Med. 165 (8): 863–7. PMID 15851636. doi:10.1001/archinte.165.8.863.
- ↑ Spiegel, K.; R. Leproult; E. Van Cauter (23 October 1999). "Impact of sleep debt on metabolic and endocrine function". The Lancet. 354 (9188): 1435–9. PMID 10543671. doi:10.1016/S0140-6736(99)01376-8.
- ↑ Fincher, Marcelo. "Not Sleeping Enough Is Dangerous". Retrieved 24 July 2017.
- ↑ "Renew – Sleep and Stress". The Franklin Institute Online. 2004.
- ↑ "Brain Activity is Visibly Altered Following Sleep Deprivation". UC San Diego Health System. 3 February 2006. Archived from the original on 2011-03-10.
- ↑ "Lack of Sleep Takes Toll on Brain Power". WebMD. Retrieved 2010-12-14.
- ↑ "Effects of Sleep Deprivation". http://www.easynight.org. Retrieved 21 November 2014. External link in
|website=(help) - ↑ Yoo, Seung-Schik; Gujar, Ninad; Hu, Peter; Jolesz, Ferenc; Walker, Matthew (2007). "The human emotional brain without sleep- a prefrontal amygdala disconnect". Current Biology. 17 (20): R877–R878. PMID 17956744. doi:10.1016/j.cub.2007.08.007.
- 1 2 Thomas, M., Sing, H., Belenky, G., Holcomb, H., Mayberg, H., Dannals, R., Wagner JR., H., Thorne, D., Popp, K., Rowland, L., Welsh, A., Balwinski, S. and Redmond, D. (2000). "Neural basis of alertness and cognitive performance impairments during sleepiness. I. Effects of 24 h of sleep deprivation on waking human regional brain activity". Journal of Sleep Research. 9 (4): 335–52. PMID 11123521. doi:10.1046/j.1365-2869.2000.00225.x.
- ↑ Siegel, Jerome M. (November 2003). "Why We Sleep" (PDF). Scientific American. Retrieved 2008-04-03.
- ↑ No sleep means no new brain cells. BBC (10 February 2007)
- ↑ Vgontzas AN, Mastorakos G, Bixler EO, Kales A, Gold PW, Chrousos GP; Mastorakos; Bixler; Kales; Gold; Chrousos (August 1999). "Sleep deprivation effects on the activity of the hypothalamic-pituitary-adrenal and growth axes: potential clinical implications". Clin. Endocrinol. 51 (2): 205–15. PMID 10468992. doi:10.1046/j.1365-2265.1999.00763.x.
- ↑ Mostaghimi, L.; Obermeyer, WH; Ballamudi, B; Martinez-Gonzalez, D; Benca, RM (2005). "Effects of sleep deprivation on wound healing". Journal of Sleep Research. 14 (3): 213–9. PMID 16120095. doi:10.1111/j.1365-2869.2005.00455.x.
- ↑ Gümüştekín K; Seven B; Karabulut N; Aktas, Ömer; Gürsan, Nesrin; Aslan, Sahin; Keles, Mustafa; Varoglu, Erhan; Dane, Senol (November 2004). "Effects of sleep deprivation, nicotine, and selenium on wound healing in rats". Int. J. Neurosci. 114 (11): 1433–42. PMID 15636354. doi:10.1080/00207450490509168.
- ↑ Kolb, Bryan; Whishaw, Ian (2014). An Introduction to Brain and Behavior (4th ed.). New York, New York: Worth Publishers. pp. 468–469. ISBN 9781429242288.
- ↑ Van Dongen HA; Maislin, G; Mullington, JM; Dinges, DF (2002). "The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation" (PDF). Sleep. 26 (2): 117–26. PMID 12683469.
- 1 2 "Drowsy Driving Fact Sheet" (PDF). American Academy of Sleep Medicine. 2 December 2009.
- 1 2 Carpenter, Siri (2001). "Sleep deprivation may be undermining teen health". Monitor on Psychology. 32 (9): 42.
- ↑ Williamson AM, Feyer AM; Feyer (2000). "Moderate sleep deprivation produces impairments in cognitive and motor performance equivalent to legally prescribed levels of alcohol intoxication". Occup. Environ. Med. 57 (10): 649–55. PMC 1739867 . PMID 10984335. doi:10.1136/oem.57.10.649.
- ↑ Dawson, Drew; Kathryn Reid (1997). "Fatigue, alcohol and performance impairment". Nature. 388 (6639): 235. PMID 9230429. doi:10.1038/40775.
- ↑ Drummond, SEAN P.A.; Paulus, MP; Tapert, SF (September 2006). "Effects of two nights sleep deprivation and two nights recovery sleep on response inhibition". Journal of Sleep Research. 15 (3): 261–5. PMID 16911028. doi:10.1111/j.1365-2869.2006.00535.x.
- ↑ Timothy Roehrs; Beare, David; Zorick, Frank; Roth, Thomas (February 1994). "Sleepiness and ethanol effects on simulated driving". Alcoholism: Clinical and Experimental Research. 18 (1): 154–158. doi:10.1111/j.1530-0277.1994.tb00896.x.
- ↑ "Drowsy Driving:Key Messages and Talking Points" (PDF). National Sleep Foundation. 2 December 2009.
- ↑ "Fact Sheet – Pilot Fatigue". Federal Aviation Administration. 10 September 2010.
- ↑ Baldwinn, DeWitt C. Jr.; Steven R. Daugherty (2004). "Sleep Deprivation and Fatigue in Residency Training: Results of a National Survey of First- and Second-Year Residents". Sleep. 27 (2): 217–223. PMID 15124713.
- ↑ Engle-Friedman, Mindy; Suzanne Riela; Rama Golan; Ana M. Ventuneac2; Christine M. Davis1; Angela D. Jefferson; Donna Major (June 2003). "The effect of sleep loss on next day effort". Journal of Sleep Research. 12 (2): 113–124. PMID 12753348. doi:10.1046/j.1365-2869.2003.00351.x.
- ↑ Engle Friedman, Mindy; Palencar, V; Riela, S (2010). "Sleep and effort in adolescent athletes". J. Child Health Care. 14 (2): 131–41. PMID 20435615. doi:10.1177/1367493510362129.
- 1 2 3 Coren, Stanley (1 March 1998). "Sleep Deprivation, Psychosis and Mental Efficiency". Psychiatric Times. 15 (3). Retrieved 2009-11-25.
- ↑ Whitmire, A.M.; Leveton, L.B; Barger, L.; Brainard, G.; Dinges, D.F.; Klerman, E.; Shea, C. "Risk of Performance Errors due to Sleep Loss, Circadian Desynchronization, Fatigue, and Work Overload" (PDF). Human Health and Performance Risks of Space Exploration Missions: Evidence reviewed by the NASA Human Research Program. Retrieved 25 June 2012.
- ↑ "Glossary K-M". Get Sleep. Harvard Medical School. 2012.
- ↑ "Microsleep | Microsleeps". www.sleepdex.org. Retrieved 2016-02-14.
- ↑ Vyazovskiy VV, Olcese U, Hanlon EC, Nir Y, Cirelli C, Tononi G; Olcese; Hanlon; Nir; Cirelli; Tononi (2011). "Local sleep in awake rats". Nature. 472 (7344): 443–447. Bibcode:2011Natur.472..443V. PMC 3085007 . PMID 21525926. doi:10.1038/nature10009. Lay summary.
- ↑ Everson CA, Bergmann BM, Rechtschaffen A; Bergmann; Rechtschaffen (February 1989). "Sleep deprivation in the rat: III. Total sleep deprivation". Sleep. 12 (1): 13–21. PMID 2928622.
- ↑ Does the lack of sleep make you fat?, Bristol University Press Release, 7 December 2004
- ↑ Hasler G; Buysse DJ; Klaghofer R; Gamma, A; Ajdacic, V; Eich, D; Rössler, W; Angst, J (June 2004). "The association between short sleep duration and obesity in young adults: a 13-year prospective study". Sleep. 27 (4): 661–6. PMID 15283000.
- ↑ Gangwisch JE, Malaspina D, Boden-Albala B, Heymsfield SB; Malaspina; Boden-Albala; Heymsfield (October 2005). "Inadequate sleep as a risk factor for obesity: analyses of the NHANES I". Sleep. 28 (10): 1289–96. PMID 16295214.
- ↑ Van Cauter E, Spiegel K; Spiegel (1999). "Sleep as a mediator of the relationship between socioeconomic status and health: a hypothesis". Ann. N. Y. Acad. Sci. 896: 254–61. Bibcode:1999NYASA.896..254V. PMID 10681902. doi:10.1111/j.1749-6632.1999.tb08120.x.
- ↑ Benedict C, Hallschmid M, Lassen A, Mahnke C, Schultes B, Schiöth HB, Born J, Lange T; Hallschmid; Lassen; Mahnke; Schultes; Schiöth; Born; Lange (June 2011). "Acute sleep deprivation reduces energy expenditure in healthy men". Am. J. Clin. Nutr. 93 (6): 1229–36. PMID 21471283. doi:10.3945/ajcn.110.006460.
- ↑ Benedict C, Brooks SJ, O'Daly OG, Almèn MS, Morell A, Åberg K, Gingnell M, Schultes B, Hallschmid M, Broman JE, Larsson EM, Schiöth HB; Brooks; O'Daly; Almèn; Morell; Åberg; Gingnell; Schultes; Hallschmid; Broman; Larsson; Schiöth (January 2012). "Acute sleep deprivation enhances the brain's response to hedonic food stimuli: an fMRI study". J. Clin. Endocrinol. Metab. 97 (3): E443–7. PMID 22259064. doi:10.1210/jc.2011-2759.
- ↑ Hogenkamp PS, Nilsson E, Nilsson VC, Chapman CD, Vogel H, Lundberg LS, Zarei S, Cedernaes J, Rångtell FH, Broman JE, Dickson SL, Brunstrom JM, Benedict C, Schiöth JB; Nilsson; Nilsson; Chapman; Vogel; Lundberg; Zarei; Cedernaes; Rångtell; Broman; Dickson; Brunstrom; Benedict; Schiöth (2013). "Acute sleep deprivation increases portion size and affects food choice in young men". Psychoneuroendocrinology. 38 (9): 1668–74. PMID 23428257. doi:10.1016/j.psyneuen.2013.01.012.
- ↑ Schmid, Sebastian M.; Hallschmid, Manfred; Jauch-Chara, Kamila; Born, JAN; Schultes, Bernd (2008). "A single night of sleep deprivation increases ghrelin levels and feelings of hunger in normal-weight healthy men". Journal of Sleep Research. 17 (3): 331–4. PMID 18564298. doi:10.1111/j.1365-2869.2008.00662.x.
- ↑ Franken, P; Dijk, DJ; Tobler, I; Borbély, AA (1991). "Sleep deprivation in rats: effects on EEG power spectra, vigilance states, and cortical temperature". Am. J. Physiol. Regul. Integr. Comp. Physiol. 261 (1 Pt 2): R198–R208. PMID 1858947.
- ↑ Rechtschaffen A, Bergmann BM, Gilliland MA, Bauer K; Bergmann; Gilliland; Bauer (1999). "Effects of method, duration, and sleep stage on rebounds from sleep deprivation in the rat". Sleep. 22 (1): 11–31. PMID 9989363.
- ↑ Jouvet D, Vimont P, Delorme F, Jouvet M; Vimont; Delorme; Jouvet (1964). "[Study of selective deprivation of the paradoxal sleep phase in the cat.]". C. R. Séances Soc. Biol. Fil. (in French). 158: 756–9. PMID 14186938.
- ↑ Harry B. Cohen; William C. Dement (1965). "Sleep: Changes in Threshold to Electroconvulsive Shock in Rats after Deprivation of "Paradoxical" Phase". Science. 150 (3701): 1318–9. Bibcode:1965Sci...150.1318C. PMID 5857002. doi:10.1126/science.150.3701.1318.
- ↑ van Hulzen ZJ, Coenen AM; Coenen (October 1981). "Paradoxical sleep deprivation and locomotor activity in rats". Physiol. Behav. 27 (4): 741–4. PMID 7323178. doi:10.1016/0031-9384(81)90250-X.
- ↑ Van Hulzen ZJ, Coenen AM; Coenen (December 1980). "The pendulum technique for paradoxical sleep deprivation in rats". Physiol. Behav. 25 (6): 807–11. PMID 7220622. doi:10.1016/0031-9384(80)90298-X.
- ↑ "Binyam Mohamed torture appeal lost by UK government...". BBC News. 2 October 2009.
- ↑ Begin, Menachem (1979). White nights: the story of a prisoner in Russia. San Francisco: Harper & Row. ISBN 0-06-010289-6.
- ↑ Ireland v. the United Kingdom paragraph 102
- ↑ "Explaining and Authorizing Specific Interrogation Techniques". The New York Times. 17 April 2009.
- ↑ Hassan T (3 October 2006). "Sleep deprivation remains red-hot question". PM. abc.net.au.
- ↑ "Sleep deprivation is torture: Amnesty". The Sydney Morning Herald. AAP. 3 October 2006.
- ↑ Carlson, Neil (2013). Physiology of Behavior (11th ed.). Boston: Pearson. pp. 578–579. ISBN 9780205239399.
- ↑ Gorgulu Y, Caliyurt O; Caliyurt (Sep 2009). "Rapid antidepressant effects of sleep deprivation therapy correlates with serum BDNF changes in major depression". Brain Res. Bull. 80 (3): 158–62. PMID 19576267. doi:10.1016/j.brainresbull.2009.06.016.
- ↑ Selvi, Yavuz; Mustafa Gulec; Mehmet Yucel Agargun; Lutfullah Besiroglu (2007). "Mood changes after sleep deprivation in morningness–eveningness chronotypes in healthy individuals" (PDF). Journal of Sleep Research. 16 (3): 241–4. PMID 17716271. doi:10.1111/j.1365-2869.2007.00596.x.
- ↑ Davies, S. K.; Ang, J. E.; Revell, V. L.; Holmes, B; Mann, A; Robertson, F. P.; Cui, N; Middleton, B; Ackermann, K; Kayser, M; Thumser, A. E.; Raynaud, F. I.; Skene, D. J. (Jul 22, 2014). "Effect of sleep deprivation on the human metabolome". Proc Natl Acad Sci USA. 111 (29): 10761–6. Bibcode:2014PNAS..11110761D. PMC 4115565 . PMID 25002497. doi:10.1073/pnas.1402663111.
- ↑ Wirz-Justice A, Van den Hoofdakker RH; Van Den Hoofdakker (August 1999). "Sleep deprivation in depression: what do we know, where do we go?". Biol. Psychiatry. 46 (4): 445–53. PMID 10459393. doi:10.1016/S0006-3223(99)00125-0.
- ↑ Disorders That Disrupt Sleep (Parasomnias). eMedicineHealth
- ↑ Miller, CB; et al. (October 2014). "The evidence base of sleep restriction therapy for treating insomnia disorder.". Sleep Redicine Reviews. 18 (5): 415–24. PMID 24629826. doi:10.1016/j.smrv.2014.01.006.
- ↑ Morphy, Hannah; Dunn, Kate M.; Lewis, Martyn; Boardman, Helen F.; Croft, Peter R. (2007). "Epidemiology of Insomnia: a Longitudinal Study in a UK Population". Sleep. 30 (3). Retrieved 13 December 2015.
- ↑ Kim, K; Uchiyama, M; Okawa, M; Liu, X; Ogihara, R (1 February 2000). "An epidemiological study of insomnia among the Japanese general population.". Sleep. 23 (1): 41–7. PMID 10678464. Retrieved 13 December 2015.
- 1 2 "Dyssomnias" (PDF). WHO. pp. 7–11. Retrieved 2009-01-25.
- ↑ Buysse, Daniel J. (2008). "Chronic Insomnia". Am. J. Psychiatry. 165 (6): 678–86. PMC 2859710 . PMID 18519533. doi:10.1176/appi.ajp.2008.08010129.
For this reason, the NIH conference [of 2005] commended the term "comorbid insomnia" as a preferable alternative to the term "secondary insomnia."
- ↑ Erman, Milton K. (2007). "Insomnia: Comorbidities and Consequences". Primary Psychiatry. 14 (6): 31–35.
Two general categories of insomnia exist, primary insomnia and comorbid insomnia.
- ↑ World Health Organization (2007). "Quantifying burden of disease from environmental noise" (PDF). p. 20. Retrieved 2010-09-22.
- ↑ "Idiopathic Insomnia - American Sleep Association". www.sleepassociation.org. Retrieved 2016-04-19.
- ↑ Biological Rhythms, Sleep and Hypnosis by Simon Green
- ↑ Wehr, TA (1987). "Sleep reduction as a final common pathway in the genesis of mania". Am. J. Psychiatry. 144: 201–204. PMID 3812788. doi:10.1176/ajp.144.2.201.
- ↑ "National Sleep Foundation Key Messages/Talking Points" (PDF). Retrieved April 18, 2016.
- ↑ Shelley D Hershner; Ronald D Chervin (June 23, 2014). "Causes and consequences of sleepiness among college students". Nature and Science of Sleep. 6: 73–84. PMC 4075951 . PMID 25018659. doi:10.2147/NSS.S62907.
- ↑ Tsai LL, Li SP; Li (2004). "Sleep patterns in college students; Gender and grade differences". J. Psychosom. Res. 56 (2): 231–7. PMID 15016583. doi:10.1016/S0022-3999(03)00507-5.
- ↑ Randolph E. Schmid (28 March 2006). "Sleep-deprived teens dozing off at school". ABC News. Associated Press. Archived from the original on 8 December 2006.
- ↑ Giedd JN (October 2009). "Linking adolescent sleep, brain maturation, and behavior". Journal of Adolescent Health. 45 (4): 319–320. PMC 3018343 . PMID 19766933. doi:10.1016/j.jadohealth.2009.07.007.
- ↑ "Sleep Deprivation" (PDF). American Academy of Sleep Medicine. 2008. Retrieved March 25, 2015.
- ↑ "Sleep Deprivation Fact Sheet" (PDF). American Academy of Sleep Medicine. 2 December 2009.
- 1 2 Alex Boese (5 November 2007). "Eleven days awake". Elephants on Acid: And Other Bizarre Experiments. Harvest Books. pp. 90–93. ISBN 0-15-603135-3.
- ↑ Ross J (1965). "Neurological Findings After Prolonged Sleep Deprivation". Archives of Neurology. 12 (4): 399–403. PMID 14264871. doi:10.1001/archneur.1965.00460280069006.
- ↑ Thao, Vu Phuong. "Vietnam man handles three decades without sleep". Thanh Nien Daily. Vietnam National Youth Federation. Archived from the original on 13 May 2008. Retrieved 2008-05-26.
- ↑ "Ukrainian man has been lacking sleep for 20 years". Retrieved 2016-10-05.
- ↑ Dan Childs (30 March 2009). "11 Baffling Medical Conditions". ABC News. The Boy Who Couldn't Sleep.
- ↑ "Matters of dispute – Sleepless in Ukraine". The Guardian. 10 February 2005. Retrieved 11 May 2010.
- ↑ "Boy, 3, Sleeps for First Time After Experimental Surgery". FoxNews.com. 16 May 2008.
- ↑ Canning, Andrea (23 January 2009). "Mystery of Sleepless Boy Solved: Boy Who Couldn't Sleep Undergoes Risky, Life-Changing Operation". ABC News.
- ↑ Fischer-Perroudon C, Mouret J, Jouvet M; Mouret; Jouvet (1974). "One case of agrypnia (4 months without sleep) in a morvan disease, favourable action of 5-hydroxytryptophane". Electroencephalography and Clinical Neurophysiology. 36 (1): 1–18. PMID 4128428. doi:10.1016/0013-4694(74)90132-1.
External links
| Classification |
V · T · D |
|---|---|
| External resources |
- "How Much Sleep Do You Really Need?", U.S. National Sleep Foundation
- National Sleep Foundation 2005 Sleep in America Poll
- Why Do Humans and Many Other Animals Sleep?
- Effects of Sleep and Sleep Deprivation on Catecholamine And Interleukin-2 Levels in Humans: Clinical Implications
- Effects of Sleep and Sleep Deprivation on Interleukin-6, Growth Hormone, Cortisol, and Melatonin Levels in Humans
- Sleep Deprivation Julian Lim and David F. Dinges, Scholarpedia, 2(8):2433. doi:10.4249/scholarpedia.2433