Dermatomyositis
| Dermatomyositis | |
|---|---|
 | |
| Discrete red areas overlying the knuckles in a person with juvenile dermatomyositis. These are known as Gottron's papules. | |
| Specialty | Rheumatology |
| Symptoms | Rash, muscle weakness, weight loss, fever[1] |
| Complications | Calcinosis, lung inflammation, heart disease[1][2] |
| Usual onset | 40s to 50s[3] |
| Duration | Long term[1] |
| Causes | Unknown[1] |
| Diagnostic method | Based on symptoms, blood tests, electromyography, muscle biopsies[3] |
| Similar conditions | Polymyositis, inclusion body myositis, scleroderma[3] |
| Treatment | Medication, physical therapy, exercise, heat therapy, orthotics, assistive devices, rest[1] |
| Medication | Corticosteroids, methotrexate, azathioprine[1] |
| Frequency | ~ 1 per 100,000 people per year[3] |
Dermatomyositis (DM) is a long term inflammatory disorder which affects muscles.[1] Symptoms generally a skin rash and worsening muscle weakness over time.[1] Symptoms may occur suddenly or develop over months.[1] Other symptoms may include weight loss, fever, lung inflammation, or light sensitivity.[1] Complications may include calcium deposits in muscles or skin.[1]
The cause is unknown.[1] Theories include that it is an autoimmune disease or a result of a viral infection.[1] It is a type of inflammatory myopathy.[1] Diagnosis is typically based on some combination of symptoms, blood tests, electromyography, and muscle biopsies.[3]
While there is no cure for the condition, treatments generally improve symptoms.[1] Treatments may include medication, physical therapy, exercise, heat therapy, orthotics, and assistive devices, and rest.[1] Medications in the corticosteroids family are typically used with other agents like methotrexate or azathioprine recommended if steroids are not working well.[1] Intravenous immunoglobulin may also improve outcomes.[1] Most people improve with treatment and in some the condition resolves completely.[1]
About 1 per 100,000 people per year are newly affected.[3] The condition usually occurs in those in their 40s and 50s with women being affected more often than men.[3] People of any age, however, may be affected.[3] The condition was first described in the 1800s.[4]
Signs and symptoms
The main symptoms include several kinds of skin rash along with muscle weakness in both upper arms or thighs.[2]
Skin
One form the rashes take is called "heliotrope" (a purplish color) or lilac, but may also be red. It can occur around the eyes along with swelling, but also occurs on the upper chest or back what is called the "shawl" (around the neck) or "V-sign" above the breasts and may also occur on the face, upper arms, thighs, or hands.[5] Another form the rash takes is called Gottron's sign which are red, sometimes scaly, papules that erupt on any of the finger joints (the metacarpophalangeal joints or the interphalangeal joints).[5][6] All these rashes are made worse by exposure to sunlight, and are often very itchy, painful, and may bleed.[6]
If a person exhibits only skin findings characteristic of DM, without weakness or abnormal muscle enzymes, then he or she may be experiencing amyopathic dermatomyositis (ADM, formerly known as "dermatomyositis sine myositis".[7]
Muscles
People with DM experience progressively worsening muscle weakness in the proximal muscles (for example, the shoulders and thighs).[8] Tasks that use these muscles: standing from sitting, lifting, and climbing stairs, can prove challenging for people with DM.[8]
Other
Around 30% of people have swollen, painful joints, but this is generally mild.[9]
In some people the condition affects the lungs, and they may have a cough or difficulty breathing. If the condition affects the heart, there may be arrhythmias. If it affects the blood vessels in the stomach or intestines, which is more common in juvenile DM, the person might vomit blood, have black, tarry bowel movements, or may develop a hole somewhere in their GI tract.[9]
 Gottron's papules on finger joints.
Gottron's papules on finger joints. Gottron's papules on the elbows of a person with juvenile DM
Gottron's papules on the elbows of a person with juvenile DM Gottron's papules
Gottron's papules Gottron's papules on a person with juvenile DM
Gottron's papules on a person with juvenile DM Gottron's papules in severe case of juvenile dermatomyositis
Gottron's papules in severe case of juvenile dermatomyositis Heliotrope with swelling around the eyes.
Heliotrope with swelling around the eyes. Heliotrope
Heliotrope Facial rash
Facial rash Severe rash on the hands, extending up the forearm
Severe rash on the hands, extending up the forearm Forearm rash
Forearm rash
Causes
The cause is unknown, but it may result from an initial viral infection or cancer, either of which could raise an autoimmune response.[9]
Between 7 and 30% of dermatomyositis arise from cancer, probably as an autoimmune response.[10] The most common associated cancers are ovarian cancer, breast cancer, and lung cancer.[10] 18 to 25% of people with amyopathic DM also have cancer.[6]
Some cases are inherited, and HLA subtypes HLA-DR3, HLA-DR52, and HLA-DR6 seem to create a disposition to dermatomyositis.[9]
Diagnosis


The diagnosis of dermatomyositis is based on five criteria which are also used to differentially diagnose with respect to polymyositis:[7]
- Muscle weakness in both thighs or both upper arms
- Using a blood test, finding higher levels of enzymes found in skeletal muscle, including creatinine kinase, aldolase, as well as glutamate oxaloacetate, pyruvate transaminases and lactate dehydrogenase
- Using testing of electric signalling in muscles, finding all three of the following: erratic, repetitive high frequency signals; short, low energy signals between skeletal muscles and motor neurons that have multiple phases; and sharp activity when a needle is inserted into the muscle
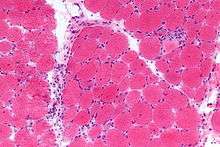
- Examining a muscle biopsy under a microscope and finding mononuclear white blood cells between the muscle cells, and finding abnormal muscle cell degeneration and regeneration, dying muscle cells, and muscle cells being consumed by other cells (phagocytosis)
- Rashes typical of dermatomyositis, which include heliotrope rash, Gottron sign and Gottron papules
The fifth criterion is what differentiates dermatomyositis from polymyositis; the diagnosis is considered definite for dermatomyositis if three of items 1 through 4 are present in addition to 5, probable with any two in addition to 5, and possible if just one is present in addition to 5.[7]
Dermatomyositis is associated with autoantibodies, especially antinuclear antibodies (ANA).[9] Around 80% of people with DM test positive for ANA and around 30% of people have myositis-specific autoantibodies which include antibodies to aminoacyl-tRNA synthetases (anti-synthetase antibodies), including antibodies against Histidine—tRNA ligase (also called Jo-1); antibodies to signal recognition particle (SRP); and anti-Mi-2 antibodies.[9]
Magnetic resonance imaging may be useful to guide muscle biopsy and to investigate involvement of internal organs;[11] X-ray may be used to investigate joint involvement and calcifications.[12]
A given case of dermatomyositis may be classified as amyopathic dermatomyositis if only skin is affected and there is no muscle weakness for longer than 6 months according to one 2016 review,[7] or two years according to another.[6]
Classification
Dermatomyositis is a form of systemic connective tissue disorder, a class of diseases that often involve autoimmune dysfunction.[9][13]
It has also been classified as an idiopathic inflammatory myopathy along with polymyositis, necrotizing autoimmune myositis, cancer-associated myositis, and sporadic inclusion body myositis.[14]
There is a form of this disorder that strikes children, known as juvenile dermatomyositis (JDM).[15]
Treatment
There is no cure for dermatomyositis, but the symptoms can be treated. Options include medication, physical therapy, exercise, heat therapy (including microwave and ultrasound), orthotics and assistive devices, and rest. The standard treatment for dermatomyositis is a corticosteroid drug, given either in pill form or intravenously. Immunosuppressant drugs, such as azathioprine and methotrexate, may reduce inflammation in people who do not respond well to prednisone. Periodic treatment using intravenous immunoglobulin can also improve recovery. Other immunosuppressive agents used to treat the inflammation associated with dermatomyositis include cyclosporine A, cyclophosphamide, and tacrolimus. Physical therapy is usually recommended to prevent muscle atrophy and to regain muscle strength and range of motion. Many individuals with dermatomyositis may need a topical ointment, such as topical corticosteroids, for their skin disorder. They should wear a high-protection sunscreen and protective clothing. Surgery may be required to remove calcium deposits that cause nerve pain and recurrent infections.[16]
Antimalarial medications, especially hydroxychloroquine and chloroquine, are used to treat the rashes, as they are in similar conditions.[6]
Rituximab is used when people don't respond to other treatments.[17][18]
As of 2016, treatments for amyopathic dermatomyositis in adults did not have a strong evidence base; published treatments included antimalarial medications, steroids, taken or orally or applied to the skin, calcineurin inhibitors applied to the skin, dapsone, Intravenous immunoglobulin (IVIG), methotrexate, azathioprine, and mycophenolate mofetil. None appear to be very effective but among them, IVIG has had the best outcomes.[7]
Prognosis
Before the advent of modern treatments such as prednisone, intravenous immunoglobulin, plasmapheresis, chemotherapies, and other drugs, the prognosis was poor.[19]
The cutaneous manifestations of dermatomyositis may or may not improve with therapy in parallel with the improvement of the myositis. In some people, the weakness and rash resolve together. In others, the two are not linked, with one or the other being more challenging to control. Often, cutaneous disease persists after adequate control of the muscle disease.
The risk of death from the condition is much higher if the heart or lungs are affected.[14][16]
Epidemiology
Incidence of DM peaks at ages 40–50, but the disease can affect people of all ages.[20] The prevalence of DM ranges from 1 to 22 per 100,000 people.[21][22][23]
History
The diagnostic criteria were proposed in 1975 and became widely adopted.[6][24] Amyopathic DM, also called DM sine myositis, was named in 2002.[6]
Society and culture
- The opera singer Maria Callas (1923 - 1977) suffered from dermatomyositis from 1975 until her death.[25]
- The actor Laurence Olivier (1907 – 1989) suffered from dermatomyositis from 1974 until his death.[26]
- The American football running back Ricky Bell (1955 - 1984), the runner-up for the Heisman Trophy in 1976, and the number-one choice in the NFL draft in 1977, died at the age of 29 from heart failure caused by this disease.[27]
- Rob Buckman (1948 - 2011) a doctor, comedian, author, and the president of the Humanist Association of Canada.[28][29]
Research
As of 2016, research was ongoing into causes for DM, as well as biomarkers;[30] clinical trials were ongoing for use of the following drugs in DM: ajulemic acid (Phase II), adrenocorticotropic hormone gel (Phase IV, open label), IMO-8400, an antagonist of Toll-like receptor 7,8 and 9 (Ph II), abatacept (Phase IV, open label), and sodium thiosulfate (Phase II).[6]
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 "Dermatomyositis". GARD. 2017. Retrieved 13 July 2017.
- 1 2 Callen, Jeffrey P.; Wortmann, Robert L. (2006-09-01). "Dermatomyositis". Clinics in Dermatology. 24 (5): 363–373. ISSN 0738-081X. PMID 16966018. doi:10.1016/j.clindermatol.2006.07.001.
- 1 2 3 4 5 6 7 8 "Dermatomyositis". NORD (National Organization for Rare Disorders). 2015. Retrieved 13 July 2017.
- ↑ Dourmishev, Lyubomir A.; Dourmishev, Assen Lyubenov (2009). Dermatomyositis: Advances in Recognition, Understanding and Management. Springer Science & Business Media. p. 5. ISBN 9783540793137.
- 1 2 Callen, Jeffrey P. (2010-06-01). "Cutaneous manifestations of dermatomyositis and their management". Current Rheumatology Reports. 12 (3): 192–197. ISSN 1534-6307. PMID 20425525. doi:10.1007/s11926-010-0100-7.
- 1 2 3 4 5 6 7 8 Kuhn, A; Landmann, A; Bonsmann, G (October 2016). "The skin in autoimmune diseases-Unmet needs.". Autoimmunity reviews. 15 (10): 948–54. PMID 27481041. doi:10.1016/j.autrev.2016.07.013.
- 1 2 3 4 5 Callander, J; Robson, Y; Ingram, J; Piguet, V (11 May 2016). "Treatment of clinically amyopathic dermatomyositis in adults: a systematic review.". The British journal of dermatology. PMID 27167896. doi:10.1111/bjd.14726.
- 1 2 Dalakas, Marinos C. (2015-04-30). "Inflammatory Muscle Diseases". New England Journal of Medicine. 372 (18): 1734–1747. ISSN 0028-4793. PMID 25923553. doi:10.1056/NEJMra1402225.
- 1 2 3 4 5 6 7 Hajj-ali, Rula A. (June 2013). "Polymyositis and Dermatomyositis - Musculoskeletal and Connective Tissue Disorders". Merck Manuals Professional Edition.
- 1 2 Di Rollo, D; Abeni, D; Tracanna, M; Capo, A; Amerio, P (October 2014). "Cancer risk in dermatomyositis: a systematic review of the literature.". Giornale italiano di dermatologia e venereologia : organo ufficiale, Societa italiana di dermatologia e sifilografia. 149 (5): 525–37. PMID 24975953.
- ↑ Simon, JP; Marie, I; Jouen, F; Boyer, O; Martinet, J (14 June 2016). "Autoimmune Myopathies: Where Do We Stand?". Frontiers in immunology. 7: 234. PMC 4905946
 . PMID 27379096. doi:10.3389/fimmu.2016.00234.
. PMID 27379096. doi:10.3389/fimmu.2016.00234. - ↑ Ramos-E-Silva, M; Lima Pinto, AP; Pirmez, R; Cuzzi, T; Carneiro, S (1 October 2016). "Dermatomyositis-Part 2: Diagnosis, Association With Malignancy, and Treatment.". Skinmed. 14 (5): 354–358. PMID 27871347.
- ↑ "ICD-10 Systemic connective tissue disorders (M30-M36)". WHO. Retrieved 9 December 2016.
- 1 2 Danieli, MG; Gelardi, C; Guerra, F; Cardinaletti, P; Pedini, V; Gabrielli, A (May 2016). "Cardiac involvement in polymyositis and dermatomyositis.". Autoimmunity reviews. 15 (5): 462–5. PMID 26826433. doi:10.1016/j.autrev.2016.01.015.
- ↑ Feldman BM, Rider LG, Reed AM, Pachman LM (June 2008). "Juvenile dermatomyositis and other idiopathic inflammatory myopathies of childhood". Lancet. 371 (9631): 2201–2212. PMID 18586175. doi:10.1016/S0140-6736(08)60955-1.
- 1 2 "Dermatomyositis Information". National Institute of Neurological Disorders and Stroke. July 27, 2015.
- ↑ Malik, A; Hayat, G; Kalia, JS; Guzman, MA (20 May 2016). "Idiopathic Inflammatory Myopathies: Clinical Approach and Management.". Frontiers in neurology. 7: 64. PMC 4873503 . PMID 27242652. doi:10.3389/fneur.2016.00064.
- ↑ Wright, NA; Vleugels, RA; Callen, JP (January 2016). "Cutaneous dermatomyositis in the era of biologicals.". Seminars in immunopathology. 38 (1): 113–21. PMID 26563285. doi:10.1007/s00281-015-0543-z.
- ↑ Page 285 in: Thomson and Cotton Lecture Notes in Pathology, Blackwell Scientific. Third Edition
- ↑ Tymms, K. E.; Webb, J. (1985-12-01). "Dermatopolymyositis and other connective tissue diseases: a review of 105 cases". The Journal of Rheumatology. 12 (6): 1140–1148. ISSN 0315-162X. PMID 4093921.
- ↑ Cooper, Glinda S.; Stroehla, Berrit C. (2003-05-01). "The epidemiology of autoimmune diseases". Autoimmunity Reviews. 2 (3): 119–125. ISSN 1568-9972. PMID 12848952.
- ↑ Bernatsky, S.; Joseph, L.; Pineau, C. A.; Bélisle, P.; Boivin, J. F.; Banerjee, D.; Clarke, A. E. (2009-07-01). "Estimating the prevalence of polymyositis and dermatomyositis from administrative data: age, sex and regional differences". Annals of the Rheumatic Diseases. 68 (7): 1192–1196. ISSN 1468-2060. PMID 18713785. doi:10.1136/ard.2008.093161.
- ↑ Bendewald, Margo J.; Wetter, David A.; Li, Xujian; Davis, Mark D. P. (2010-01-01). "Incidence of dermatomyositis and clinically amyopathic dermatomyositis: a population-based study in Olmsted County, Minnesota". Archives of Dermatology. 146 (1): 26–30. ISSN 1538-3652. PMC 2886726 . PMID 20083689. doi:10.1001/archdermatol.2009.328.
- ↑ Bohan, A; Peter, JB (13 February 1975). "Polymyositis and dermatomyositis (first of two parts).". The New England Journal of Medicine. 292 (7): 344–7. PMID 1090839. doi:10.1056/nejm197502132920706. and Bohan, A; Peter, JB (20 February 1975). "Polymyositis and dermatomyositis (second of two parts).". The New England Journal of Medicine. 292 (8): 403–7. PMID 1089199. doi:10.1056/nejm197502202920807.
- ↑ "Greek Reporter: 'Maria Callas did not kill herself from grief for Onassis, a rare disease cost her career and life'". GR Reporter. 28 December 2010. Retrieved 1 January 2015.
- ↑ "Laurence Olivier Dies: 'The Rest Is Silence'". People Magazine. 24 July 1989. Retrieved 16 July 2012.
- ↑ "Forgotten: Ricky Bell". Pro Football Weekly. 8 January 2010. Retrieved 26 January 2010.
- ↑ "Rob Buckman obituary". The Guardian Newspaper. 12 October 2011. Retrieved 16 July 2012.
- ↑ "Dr. Robert Buckman, renowned oncologist, comedian and Star columnist, dead at 63". The Toronto Star Newspaper. 10 October 2011. Retrieved 16 July 2012.
- ↑ Ramos-E-Silva, M; Pinto, AP; Pirmez, R; Cuzzi, T; Carneiro, SC (1 August 2016). "Dermatomyositis--Part 1: Definition, Epidemiology, Etiology and Pathogenesis, and Clinics.". Skinmed. 14 (4): 273–279. PMID 27784516.
![]() This article incorporates public domain material from the United States Department of Health and Human Services document "NINDS Dermatomyositis Information Page" (retrieved on 2016-12-12).
This article incorporates public domain material from the United States Department of Health and Human Services document "NINDS Dermatomyositis Information Page" (retrieved on 2016-12-12).
External links
| Classification |
V · T · D |
|---|---|
| External resources |