Sacroiliac joint
| Sacroiliac joint | |
|---|---|
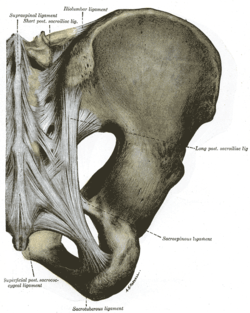
 Sacroiliac joint of the male pelvis, posterior view | |
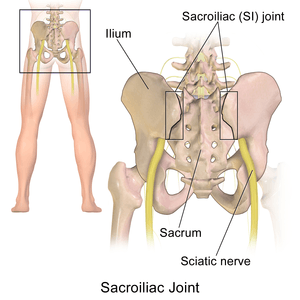
 Human female pelvis, anterior view, with sacroiliac joint within red ellipse. | |
| Details | |
| Identifiers | |
| Latin | articulatio sacroiliaca |
| TA | A03.6.03.001 |
| FMA | 21440 |
The sacroiliac joint or SI joint (SIJ) is the joint between the sacrum and the ilium bones of the pelvis, which are connected by strong ligaments. In humans, the sacrum supports the spine and is supported in turn by an ilium on each side. The joint is a strong, weight transferral synovial plane joint with irregular elevations and depressions that produce interlocking of the two bones.[1] The human body has two sacroiliac joints, one on the left and one on the right, that often match each other but are highly variable from person to person.[1]
Structure
Sacroiliac joints are paired C-shaped or L-shaped joints capable of a small amount of movement[2] (2–18 degrees, which is debatable at this time) that are formed between the auricular surfaces of the sacrum and the ilium bones. The joints are covered by two different kinds of cartilage; the sacral surface has hyaline cartilage and the ilial surface has fibrocartilage.[2] The SIJ's stability is maintained mainly through a combination of only some bony structure and very strong intrinsic and extrinsic ligaments.[3]
As we age the characteristics of the sacroiliac joint change.[4] The joint's surfaces are flat or planar in early life but as we start walking, the sacroiliac joint surfaces develop distinct angular orientations and lose their planar or flat topography.[2] They also develop an elevated ridge along the ilial surface and a depression along the sacral surface.[5] The ridge and corresponding depression, along with the very strong ligaments, increase the sacroiliac joints' stability and makes dislocations very rare. The fossae lumbales laterales ("dimples of Venus") correspond to the superficial topography of the sacroiliac joints.
Ligaments
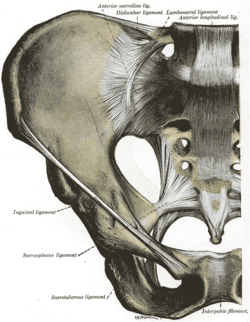
The ligaments of the sacroiliac joint include the following:[2]
- Anterior sacroiliac ligament
- Interosseous sacroiliac ligament
- Posterior sacroiliac ligament
- Sacrotuberous ligament
- Sacrospinous ligament
The anterior ligament is not much of a ligament at all and in most cases is just a slight thickening of the anterior joint capsule. The anterior ligament is thin and not as well defined as the posterior sacroiliac ligaments.
The posterior sacroiliac (SI) ligaments can be further divided into short (intrinsic) and long (extrinsic).[6] The dorsal interosseous ligaments are very strong ligaments. They are often stronger than bone, such that the pelvis may actually fracture before the ligament tears. The dorsal sacroiliac ligaments include both long and short ligaments. The long dorsal sacroiliac joint ligaments run in an oblique vertical direction while the short (interosseous) runs perpendicular from just behind the articular surfaces of the sacrum to the ilium and functions to keep the sacroiliac joint from distracting or opening. The sacrotuberous and sacrospinous ligaments (also known as the extrinsic sacroiliac joint ligaments) limit the amount the sacrum flexes.
The ligaments of the sacroiliac joint loosen during pregnancy due to the hormone relaxin; this loosening, along with that of the related symphysis pubis, permits the pelvic joints to widen during the birthing process. The long SI ligaments may be palpated in thin persons for pain and compared from one side of the body to the other; however, the reliability and the validity of comparing ligaments for pain have currently not been shown. The interosseous ligaments are very short and run perpendicular from the iliac surface to the sacrum, they keep the auricular surfaces from abducting or opening/distracting.
Function
Like most lower extremity joints, one of the SI joints' function is shock absorption (depending on the amount of available motion at the sacroiliac joint) for the spine, along with the job of torque conversion allowing the transverse rotations that take place in the lower extremity to be transmitted up the spine. The SI joint, like all lower extremity joints, provides a "self-locking" mechanism (where the joint occupies or attains its most congruent position, also called the close pack position) that helps with stability during the push-off phase of walking.[7] The joint locks (or rather becomes close packed) on one side as weight is transferred from one leg to the other, and through the pelvis the body weight is transmitted from the sacrum to the hip bone.
The motions of the sacroiliac joint
- Anterior innominate tilt of both hip bones on the sacrum (where the left and right move as a unit)
- Posterior innominate tilt of both hip bones on the sacrum (where the left and right move together as a unit)
- Anterior innominate tilt of one innominate bone while the opposite innominate bone tilts posteriorly on the sacrum (antagonistic innominate tilt) which occurs during gait
- Sacral flexion (or nutation) Motions of the sacrum occur simultaneous with motion of the ilium so you must be careful in the description of these as isolated motions.
- Sacral extension (or counter-nutation).
The sacroiliac joints like all spinal joints (except the atlanto-axial) are bicondylar joints, meaning that movement of one side corresponds to a correlative movement of the other side.
Clinical significance
Inflammation and dysfunction
Sacroiliitis refers to inflammation of one or both sacroiliac joints, and is one cause of unilateral low back pain. With sacroiliitis, the individual may experience pain in the low back, buttock or thigh, depending on the amount of inflammation. Common problems of the sacroiliac joint are often called sacroiliac joint dysfunction (also termed SI joint dysfunction; SIJD). Sacroiliac joint dysfunction generally refers to pain in the sacroiliac joint region that is caused by abnormal motion in the sacroiliac joint, either too much motion or too little motion. It typically results in inflammation of the SI joint, or sacroiliitis.
Signs and symptoms
The following are signs and symptoms that may be associated with an SI joint (SIJ) problem:
- Mechanical SIJ dysfunction usually causes a dull unilateral low back pain.[8]
- The pain is often a mild to moderate ache around the dimple or posterior superior iliac spine (PSIS) region.[9]
- The pain may become worse and sharp while doing activities such as standing up from a seated position or lifting the knee towards the chest during stair climbing.
- Pain is typically on one side or the other (unilateral PSIS pain), but the pain can occasionally be bilateral.
- When the pain of SIJ dysfunction is severe (which is infrequent), there can be referred pain into the hip, groin, and occasionally down the leg, but rarely does the pain radiate below the knee.
- Pain can be referred from the SIJ down into the buttock or back of the thigh, and rarely to the foot.
- Low back pain and stiffness, often unilateral, that often increases with prolonged sitting or prolonged walking.
- Pain may occur during sexual intercourse; however, this is not specific to just sacroiliac joint problems.
Sacroiliac joint dysfunction is tested using provocative and nonprovocative maneuvers. Nonprovocative sacroiliac joint examination maneuvers would include Gillet Test, prone knee flexion test, supine long sitting test, standing flexion test, and seated flexion test. There is a lack of evidence that these sacroiliac joint mobility maneuvers detect motion abnormalities.[10][11]
Given the inherent technical limitations of the visible and palpable signs from these sacroiliac joint mobility maneuvers another broad category of clinical signs have been described called provocative maneuvers. These maneuvers are designed to reproduce or increase pain originating from within the sacroiliac joint. When the provocative maneuvers reproduce pain along the typical area raises suspicion for sacroiliac joint dysfunction. However no single test is very reliable in the diagnosis of sacroiliac joint dysfunction. Weakness, numbness, or the loss of a related reflex may indicate nervous system damage.
The current gold standard for diagnosis of sacroiliac joint dysfunction emanating within the joint is sacroiliac joint injection confirmed under fluoroscopy or CT-guidance using a local anesthetic solution. The diagnosis is confirmed when the patient reports a significant change in relief from pain and the diagnostic injection is performed on 2 separate visits. Published studies have used at least a 75 percent change in relief of pain before a response is considered positive and the sacroiliac joint deemed the source of pain.[12][13][14]
Pregnancy
The hormonal changes of menstruation, pregnancy, and lactation can affect the integrity of the ligament support around the SIJ, which is why women often find the days leading up to their period are when the pain is at its worst. During pregnancy, female hormones are released that allow the connective tissues in the body to relax. The relaxation is necessary so that during delivery, the female pelvis can stretch enough to allow birth. This stretching results in changes to the SIJs, making them overly mobile. Over a period of years, these changes can eventually lead to wear-and-tear arthritis. As would be expected, the more pregnancies a woman has, the higher her chances of SI joint problems. During the pregnancy, micro tears and small gas pockets can appear within the joint. [This paragraph needs citations]
Muscle imbalance, trauma (e.g., falling on the buttock) and hormonal changes can all lead to SIJ dysfunction. Sacroiliac joint pain may be felt anteriorly, however, care must be taken to differentiate this from hip joint pain.
Women are considered more likely to suffer from sacroiliac pain than men, mostly because of structural and hormonal differences between the sexes, but so far no credible evidence exists that confirms this notion. Female anatomy often allows one fewer sacral segment to lock with the pelvis, and this may increase instability.
Additional images
 Sacroiliac joint. Deep dissection. Serial cross section.
Sacroiliac joint. Deep dissection. Serial cross section.
See also
- Dimples of Venus
- Sacroiliac joint dysfunction
- Surgery for the dysfunctional sacroiliac joint
- Piriformis syndrome
References
- 1 2 Solonen, K. A. (1957). "The sacroiliac joint in the light of anatomical, roentgenological and clinical studies". Acta Orthopaedica Scandinavica Supplementum. 27: 1–127. PMID 13478452.
- 1 2 3 4 Vleeming, A.; Schuenke, M. D.; Masi, A. T.; Carreiro, J. E.; Danneels, L.; Willard, F. H. (2012). "The sacroiliac joint: An overview of its anatomy, function and potential clinical implications". Journal of Anatomy. 221 (6): 537–67. PMC 3512279
 . PMID 22994881. doi:10.1111/j.1469-7580.2012.01564.x.
. PMID 22994881. doi:10.1111/j.1469-7580.2012.01564.x. - ↑ Schunke, Gustave Bernard (1938). "The anatomy and development of the sacro-iliac joint in man". The Anatomical Record. 72 (3): 313–31. doi:10.1002/ar.1090720306.
- ↑ Walker, Joan M. (1986). "Age-Related Differences in the Human Sacroiliac Joint: A Histological Study; Implications for Therapy". Journal of Orthopaedic & Sports Physical Therapy. 7 (6): 325–34. PMID 18802258. doi:10.2519/jospt.1986.7.6.325.
- ↑ Alderink, Gordon J. (1991). "The Sacroiliac Joint: Review of Anatomy, Mechanics, and Function". Journal of Orthopaedic & Sports Physical Therapy. 13 (2): 71–84. PMID 18796854. doi:10.2519/jospt.1991.13.2.71.
- ↑ Weisl, H. (1954). "The Ligaments of the Sacro-Iliac Joint Examined with Particular Reference to Their Function". Cells Tissues Organs. 20 (3): 201–13. PMID 13137770. doi:10.1159/000140900.
- ↑ Dontigny, R. L. (1985). "Function and pathomechanics of the sacroiliac joint. A review". Physical therapy. 65 (1): 35–44. PMID 3155567.
- ↑ Cibulka MT; Delitto A & Erhard RE (1992). "Pain patterns in patients with and without sacroiliac joint dysfunction". In Vleeming A; Mooney V; Snijders CJ & Dorman T. First Interdisciplinary World Conference on Low Back Pain and its Relation to the Sacroiliac Joint. pp. 363–70. OCLC 28057865.
- ↑ Fortin, J. D.; Falco, F. J. (1997). "The Fortin finger test: An indicator of sacroiliac pain". American journal of orthopedics. 26 (7): 477–80. PMID 9247654.
- ↑ Sturesson, B; Selvik, G; Udén, A (1989). "Movements of the sacroiliac joints. A roentgen stereophotogrammetric analysis". Spine. 14 (2): 162–5. PMID 2922636. doi:10.1097/00007632-198902000-00004.
- ↑ Sturesson, B; Uden, A; Vleeming, A (2000). "A radiostereometric analysis of movements of the sacroiliac joints during the standing hip flexion test". Spine. 25 (3): 364–8. PMID 10703111. doi:10.1097/00007632-200002010-00018.
- ↑ Schwarzer, A. C.; Aprill, C. N.; Bogduk, N (1995). "The sacroiliac joint in chronic low back pain". Spine. 20 (1): 31–7. PMID 7709277. doi:10.1097/00007632-199501000-00007.
- ↑ Maigne, J. Y.; Boulahdour, H.; Chatellier, G. (1998). "Value of quantitative radionuclide bone scanning in the diagnosis of sacroiliac joint syndrome in 32 patients with low back pain". European Spine Journal. 7 (4): 328–31. PMC 3611275 . PMID 9765042. doi:10.1007/s005860050083.
- ↑ Maigne, J. Y.; Aivaliklis, A; Pfefer, F (1996). "Results of sacroiliac joint double block and value of sacroiliac pain provocation tests in 54 patients with low back pain". Spine. 21 (16): 1889–92. PMID 8875721. doi:10.1097/00007632-199608150-00012.
External links
- Huijbregts, Peter (2004). "Dysfunkcja stawu krzyżowo-biodrowego–diagnoza oparta na dowodach naukowych" [Sacroiliac joint dysfunction: evidence-based diagnosis]. Rehabilitacja Medyczna (in Polish). 8 (1): 14–37. Archived from the original on 2016-03-04.
- Anatomy image: apmalefrontal4-18 at the College of Medicine at SUNY Upstate Medical University