Ranitidine
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | /rəˈnɪtɪdiːn/ |
| Trade names | Zantac, others |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a601106 |
| License data |
|
| Pregnancy category | |
| Routes of administration | Oral, IV |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 39 to 88% |
| Protein binding | 15% |
| Metabolism | Hepatic: FMOs, including FMO3; other enzymes |
| Onset of action |
55–65 minutes (150 mg dose)[1] 55–115 minutes (75 mg dose)[1] |
| Biological half-life | 2–3 hours |
| Excretion | 30–70% Renal |
| Identifiers | |
| |
| Synonyms |
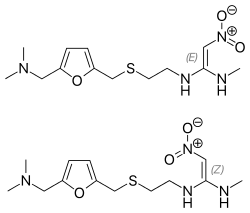
Dimethyl [(5-{[(2-{[1-(methylamino)- 2-nitroethenyl]amino}ethyl)sulfanyl] methyl}furan-2-yl)methyl]amine |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| ECHA InfoCard | 100.060.283 |
| Chemical and physical data | |
| Formula | C13H22N4O3S |
| Molar mass | 314.4 g/mol |
| 3D model (JSmol) | |
| |
| |
| | |
Ranitidine, sold under the trade name Zantac among others, is a medication that decreases stomach acid production.[2] It is commonly used in treatment of peptic ulcer disease, gastroesophageal reflux disease, and Zollinger–Ellison syndrome.[2] There is also tentative evidence of benefit for hives.[3] It can be taken by mouth, by injection into a muscle, or into a vein.[2]
Common side effects include headaches and pain or burning if given by injection. Serious side effects may include liver problems, a slow heart rate, pneumonia, and the potential of masking stomach cancer.[2] It is also linked to an increased risk of Clostridium difficile colitis.[4] It is generally safe in pregnancy. Ranitidine is an H2 histamine receptor antagonist that works by blocking histamine and thus decreasing the amount of acid released by cells of the stomach.[2]
Ranitidine was discovered in 1976 and came into commercial use in 1981.[5] It is on the World Health Organization's List of Essential Medicines, the most effective and safe medicines needed in a health system.[6] It is available as a generic medication.[2] The 2015 wholesale price in the developing world was about 0.01 to 0.05 USD per pill.[7] In the United States it is about 0.05 USD per dose.[2]
Medical uses
- Relief of heartburn
- Short-term and maintenance therapy of gastric and duodenal ulcers
- Ranitidine can also be given with NSAIDs to reduce the risk of ulceration. Proton-pump inhibitors (PPIs) are more effective for the prevention of NSAID-induced ulcers.[8]
- Pathologic gastrointestinal (GI) hypersecretory conditions such as Zollinger–Ellison syndrome
- Gastroesophageal reflux disease (GERD)
- Erosive esophagitis
- Part of a multidrug regimen for Helicobacter pylori eradication to reduce the risk of duodenal ulcer recurrence
- Recurrent postoperative ulcer
- Upper GI bleeding
- Prevention of acid-aspiration pneumonitis during surgery: ranitidine can be administered preoperatively to reduce the risk of aspiration pneumonia. The drug not only increases gastric pH, but also reduces the total output of gastric juice. In a 2009 meta-analysis comparing the net benefit of proton pump inhibitors and ranitidine to reduce the risk of aspiration before anesthesia, ranitidine was found to be more effective than proton pump inhibitors in reducing the volume of gastric secretions.[9] Ranitidine may have an antiemetic effect when administered preoperatively.
- Prevention of stress-induced ulcers in critically ill patients[10]
- Used together with diphenhydramine as secondary treatment for anaphylaxis; after first-line epinephrine.[11][12]
Preparations
Certain preparations of ranitidine are available over the counter (OTC) in various countries. In the United States, 75- and 150-mg tablets are available OTC. Zantac OTC is manufactured by Boehringer Ingelheim. In Australia and the UK, packs containing seven or 14 doses of the 150-mg tablet are available in supermarkets, small packs of 150-mg and 300-mg tablets are schedule 2 pharmacy medicines. Larger doses and pack sizes still require a prescription.
Dosing
For ulcer treatment, a night-time dose is especially important — as the increase in gastric/duodenal pH promotes healing overnight when the stomach and duodenum are empty. Conversely, for treating reflux, smaller and more frequent doses are more effective.
Ranitidine used to be administered long-term for reflux treatment, sometimes indefinitely. However, PPIs have taken over this role. In addition, a fairly rapid tachyphylaxis can develop within 6 weeks of initiation of treatment, further limiting its potential for long-term use.[13]
People with Zollinger–Ellison syndrome have been given very high doses without any harm.[14]
Contraindications
Ranitidine is contraindicated for patients known to have hypersensitivity to the drug.
Adverse effects
The following adverse effects have been reported as events in clinical trials:
Central nervous system
Rare reports have been made of malaise, dizziness, somnolence, insomnia, and vertigo. In severely ill, elderly patients, cases of reversible mental confusion, agitation, depression, and hallucinations have been reported.[15] Ranitidine causes fewer CNS adverse reactions and drug interactions compared to cimetidine.
Cardiovascular
Arrhythmias such as tachycardia, bradycardia, atrioventricular block, and premature ventricular beats have also been reported.[15]
Gastrointestinal
All drugs in its class have the potential to cause vitamin B12 deficiency secondary to a reduction in food-bound vitamin B12 absorption.[16] Elderly patients taking H2 receptor antagonists are more likely to require B12 supplementation than those not taking such drugs.[17] H2 blockers may also reduce the absorption of drugs (azole antifungals, calcium carbonate) that require an acidic stomach.[18] In addition, multiple studies suggest the use of H2 receptor antagonists such as raniditine may increase the risk of infectious diarrhoea, including traveller's diarrhoea and salmonellosis.[19][20][21][22][23] Finally, by suppressing acid-mediated breakdown of proteins, ranitidine may lead to an elevated risk of developing food or drug allergies, due to undigested proteins then passing into the gastrointestinal tract, where sensitisation occurs. Patients who take these agents develop higher levels of immunoglobulin E against food, whether they had prior antibodies or not.[24] Even months after discontinuation, an elevated level of IgE in 6% of patients was still found in this study.
Liver
Cholestatic hepatitis, liver failure, hepatitis, and jaundice have been noted, and require immediate discontinuation of the drug.[15] Blood tests can reveal an increase in liver enzymes or eosinophilia, although in rare instances, severe cases of hepatotoxicity may require a liver biopsy.[25]
Lungs
Ranitidine and other histamine H2 receptor antagonists may increase the risk of pneumonia in hospitalized patients.[26] They may also increase the risk of community-acquired pneumonia in adults and children.[27]
Blood
Thrombocytopenia is a rare but known side effect. Drug-induced thrombocytopenia usually takes weeks or months to appear, but may appear within 12 hours of drug intake in a sensitized individual. Typically, the platelet count falls to 80% of normal, and thrombocytopenia may be associated with neutropenia and anemia.[28]
Skin
Rash, including rare cases of erythema multiforme and rare cases of hair loss and vasculitis have been seen.[15]
Warnings and precautions
Disease-related concerns
With gastric malignancies, relief of symptoms due to the use of ranitidine does not exclude the presence of a gastric malignancy. In addition, with kidney or liver impairment, ranitidine must be used with caution. Finally, ranitidine should be avoided in patients with porphyria, as it may precipitate an attack.[29]
Pregnancy
This drug is rated pregnancy category B in the United States.
Lactation
Ranitidine enters breast milk, with peak concentrations seen at 5.5 hours after the dose in breast milk. Caution should be exercised when prescribed to nursing women.[30]
Children
In children, the use of gastric acid inhibitors has been associated with an increased risk for development of acute gastroenteritis and community-acquired pneumonia.[31] A cohort analysis including over 11,000 neonates reported an association of H2 blocker use and an increased incidence of necrotizing enterocolitis in very-low-birth-weight (VLBW) neonates.[32] In addition, about a sixfold increase in mortality, necrotizing enterocolitis, and infection (such as sepsis, pneumonia, urinary tract infection) was reported in patients receiving ranitidine in a cohort analysis of 274 VLBW neonates.[33]
Pharmacology
Mechanism of action
Ranitidine is a competitive, reversible inhibitor of the action of histamine at the histamine H2 receptors found in gastric parietal cells. This results in decreased gastric acid secretion and gastric volume, and reduced hydrogen ion concentration.
Pharmacokinetics
Absorption: Oral: 50% Protein binding: 15% Metabolism: N-oxide is the principal metabolite. Half-life elimination: With normal renal function, ranitidine taken orally has a half-life of 2.5–3.0 hours. If taken intravenously, the half-life is generally 2.0–2.5 hours in a patient with normal creatinine clearance. Excretion: The primary route of excretion is the urine. In addition, about 30% of the orally administered dose is collected in the urine as non-absorbed drug in 24 hours.
Elderly
In the elderly population, the plasma half-life of ranitidine is prolonged to 3–4 hours secondary to decreased kidney function causing decreased clearance.[34]
Children
In general, studies of pediatric patients (aged 1 month to 16 years) have shown no significant differences in pharmacokinetic parameter values in comparison to healthy adults, when correction is made for body weight.[34]
History

Ranitidine was first prepared as AH19065 by John Bradshaw in the summer of 1977 in the Ware research laboratories of Allen & Hanburys Ltd, part of the Glaxo organization.[35][36] Its development was a response to the first in class histamine H2 receptor antagonist, cimetidine, developed by Sir James Black at Smith, Kline and French, and launched in the United Kingdom as Tagamet in November 1976. Both companies would eventually become merged as GlaxoSmithKline following a sequence of mergers and acquisitions starting with the integration of Allen & Hanbury's Ltd and Glaxo to form Glaxo Group Research in 1979, and ultimately with the merger of Glaxo Wellcome and SmithKline Beecham in 2000. Ranitidine was the result of a rational drug-design process using what was by then a fairly refined model of the histamine H2 receptor and quantitative structure-activity relationships.
Glaxo refined the model further by replacing the imidazole ring of cimetidine with a furan ring with a nitrogen-containing substituent, and in doing so developed ranitidine. Ranitidine was found to have a far-improved tolerability profile (i.e. fewer adverse drug reactions), longer-lasting action, and 10 times the activity of cimetidine. Ranitidine has 10% of the affinity that cimetidine has to CYP450, so it causes fewer side effects, but other H2 blockers famotidine and nizatidine have no CYP450 significant interactions.[37]
Ranitidine was introduced in 1981 and was the world's biggest-selling prescription drug by 1987. It has since largely been superseded by the even more effective proton-pump inhibitors, with omeprazole becoming the biggest-selling drug for many years. When omeprazole and ranitidine were compared in a study of 144 people with severe inflammation and erosions or ulcers of the esophagus, 85% of those treated with omeprazole healed within eight weeks, compared to 50% of those given ranitidine. In addition, the omeprazole group reported earlier relief of heartburn symptoms.[38]
See also
- Famotidine (trade names Pepcid, Pepcidine) — another popular H2 receptor antagonist
- Nizatidine
References
- 1 2 Gardner JD, Ciociola AA, Robinson M, McIsaac RL (July 2002). "Determination of the time of onset of action of ranitidine and famotidine on intra-gastric acidity". Aliment. Pharmacol. Ther. 16 (7): 1317–1326. PMID 12144582. doi:10.1046/j.1365-2036.2002.01291.x.
- 1 2 3 4 5 6 7 "Ranitidine". The American Society of Health-System Pharmacists. Retrieved Dec 1, 2015.
- ↑ Fedorowicz, Z; van Zuuren, EJ; Hu, N (14 March 2012). "Histamine H2-receptor antagonists for urticaria.". The Cochrane database of systematic reviews. 3: CD008596. PMID 22419335. doi:10.1002/14651858.CD008596.pub2.
- ↑ Tleyjeh, IM; Abdulhak, AB; Riaz, M; Garbati, MA; Al-Tannir, M; Alasmari, FA; Alghamdi, M; Khan, AR; Erwin, PJ; Sutton, AJ; Baddour, LM (2013). "The association between histamine 2 receptor antagonist use and Clostridium difficile infection: a systematic review and meta-analysis.". PLOS ONE. 8 (3): e56498. PMC 3587620
 . PMID 23469173. doi:10.1371/journal.pone.0056498.
. PMID 23469173. doi:10.1371/journal.pone.0056498. - ↑ Fischer, Janos; Ganellin, C. Robin (2006). Analogue-based Drug Discovery. John Wiley & Sons. p. 444. ISBN 9783527607495.
- ↑ "WHO Model List of Essential Medicines (19th List)" (PDF). World Health Organization. April 2015. Retrieved 8 December 2016.
- ↑ "Ranitidine". International Drug Price Indicator Guide. Retrieved 1 December 2015.
- ↑ "Reflux Remedies: ranitidine". PharmaSight OTC Health. PharmaSight.org. Retrieved 16 November 2011.
- ↑ Clark, K.; Lam, L. T.; Gibson, S.; Currow, D. (2009). "The effect of ranitidine versus proton pump inhibitors on gastric secretions: a meta-analysis of randomised control trials". Anaesthesia. 64: 652–657. PMID 19453319. doi:10.1111/j.1365-2044.2008.05861.x.
- ↑ Dellinger, R. Phillip; et al. (2013). "Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012". Intensive Care Medicine. 39 (2): 165–228.
- ↑ "A Practical Guide to Anaphylaxis". American Academy of Family Physicians. Retrieved 3 February 2017.
- ↑ "Anaphylaxis: Diagnosis and Management in the Rural Emergency Department" (PDF). American Journal of Clinical Medicine. Retrieved 3 February 2017.
- ↑ Lightdale, J. R.; Gremse, D. A.; Heitlinger, L. A.; Cabana, M.; Gilger, M. A.; Gugig, R.; Hill, I. D. (2013). "Gastroesophageal reflux: management guidance for the pediatrician". Pediatrics. 131 (5): e1684–e1695. PMID 23629618. doi:10.1542/peds.2013-0421.
- ↑ "Ranitidine Drug Information". Lexicomp. Retrieved 20 April 2014.
- 1 2 3 4 "ZANTAC Drug Insert" (PDF). GlaxoSmithKline. Retrieved 19 April 2014.
- ↑ Force, R. W., and M. C. Nahata. "Effect of histamine H2-receptor antagonists on vitamin B12 absorption." The Annals of Pharmacotherapy 26.10 (1992): 1283-1286.
- ↑ Mitchell SL, Rockwood K (2001). "The association between antiulcer medication and initiation of cobalamin replacement in older persons". J Clin Epidemiol. 54 (5): 531–534. doi:10.1016/S0895-4356(00)00340-1.
- ↑ "Reflux Remedies: ranitidine". PharmaSight OTC Health. PharmaSight.org. Retrieved 16 November 2011.
- ↑ Cobelens FG, Leentvarr-Kuijpers A, Kleijnen J, Coutinho RA (1998). "Incidence and risk factors of diarrhoea in Dutch travellers: Consequences for priorities in pre-travel health advice". Trop Med Intern Health. 3: 896–903.
- ↑ Neal KR, Briji SO, Slack RC, et al. (1994). "Recent treatment with H2-antagonists and antibiotics and gastric surgery as risk factors for Salmonella infection". Br Med J. 308 (6922): 176. PMC 2542523 . PMID 7906170. doi:10.1136/bmj.308.6922.176.
- ↑ Neal KR, Scott HM, Slack RC, Logan RF (1996). "Omeprazole as a risk factor for Campylobacter gastroenteritis: Case-control study". BMJ. 312 (7028): 414–415. PMC 2350063 . PMID 8601113. doi:10.1136/bmj.312.7028.414.
- ↑ Wickramasinghe LS, Basu SK (1984). "Salmonellosis during treatment with ranitidine". Br Med J. 289 (6454): 1272. doi:10.1136/bmj.289.6454.1272.
- ↑ Ruddell WS, Axon AT, Findlay JM, et al. (1980). "Effect of cimetidine on gastric bacterial flora". Lancet. i: 672–674. doi:10.1016/s0140-6736(80)92826-3.
- ↑ Untersmayr E, Bakos N, Scholl I, et al. (2005). "Anti-ulcer drugs promote IgE formation toward dietary antigens in adult patients". FASEB J. 19 (6): 656–658. PMID 15671152. doi:10.1096/fj.04-3170fje.
- ↑ "Ranitidine: Hepatotoxicity". NIH official website. June 28, 2016. Retrieved August 25, 2016.
- ↑ Mallow S, Rebuck JA, Osler T, et al. (2004). "Do proton pump inhibitors increase the incidence of nosocomial pneumonia and related infectious complications when compared with histamine-2 receptor antagonists in critically ill trauma patients?". Curr Surg. 61 (5): 452–458. PMID 15475094. doi:10.1016/j.cursur.2004.03.014.
- ↑ Canani RB, Cirillo P, Roggero P, Romano C, Malamisura B, Terrin G, Passariello A, Manguso F, Morelli L, Guarino A (May 2006). "Therapy with gastric acidity inhibitors increases the risk of acute gastroenteritis and community-acquired pneumonia in children.". Pediatrics. 117 (5): e817–20. PMID 16651285. doi:10.1542/peds.2005-1655.
- ↑ Amit V Bangia; Narendra Kamath; Vidushi Mohan (2011). "Ranitidine-induced thrombocytopenia: A rare drug reaction". Indian J Pharmacol. 43 (1): 76–7. PMC 3062128 . PMID 21455428. doi:10.4103/0253-7613.75676.
- ↑ "Ranitidine Drug Information". Lexicomp. Retrieved 19 April 2014.
- ↑ "Ranitidine". Lexicomp. Retrieved 19 April 2014.
- ↑ Canani, RB; Cirillo, P; Roggero, P; et al. (2006). "Therapy With Gastric Acidity Inhibitors Increases the Risk of Acute Gastroenteritis and Community-Acquired Pneumonia in Children". Pediatrics. 117 (5): e817–20. PMID 16651285. doi:10.1542/peds.2005-1655.
- ↑ Guillet, R; Stoll, BJ; Cotten, CM; et al. (2006). "Association of H2-Blocker Therapy and Higher Incidence of Necrotizing Enterocolitis in Very Low Birth Weight Infants". Pediatrics. 117 (2): 137–42. PMID 16390920. doi:10.1542/peds.2005-1543.
- ↑ Terrin, G; Passariello, A; De Curtis, M; et al. (2012). "Ranitidine Is Associated With Infections, Necrotizing Enterocolitis, and Fatal Outcome in Newborns". Pediatrics. 129 (1): 40–5. PMID 22157140. doi:10.1542/peds.2011-0796.
- 1 2 "Zantac Package Insert" (PDF). FDA.
- ↑ Lednicer, Daniel (Editor). Chronicles of Drug Discovery. ACS Professional Reference Books, Volume 3, pages 45-81 1993. ISBN 0-8412-2733-0.
- ↑ US patent US4128658, "Aminoalkyl furan derivatives", 1978
- ↑ Laurence Brunton; John Lazo; Keith Parker (August 2005). Goodman & Gilman's The Pharmacological Basis of Therapeutics (11 ed.). McGraw-Hill. p. 972. ISBN 0-07-142280-3. doi:10.1036/0071422803.
- ↑ Pelot, Daniel, (M.D.). "Digestive System : New Drug for Heartburn". The New Book of Knowledge : Medicine & Health, Grolier : Danbury, Connecticut. 1990. p.262. ISBN 0-7172-8244-9. Library of Congress 82-645223
External links
| Subsidiaries | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Predecessors, acquisitions | |||||||||||
| Products |
| ||||||||||
| People |
| ||||||||||
| Litigation | |||||||||||
| Other | |||||||||||
| |||||||||||