Radiculopathy
| Radiculopathy | |
|---|---|
 | |
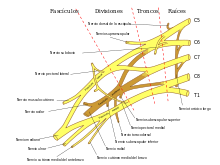
| C5-C6, followed by C6-C7, is the most common location for radiculopathy in the neck. | |
| Classification and external resources | |
| Specialty | Neurosurgery |
| ICD-10 | G54, M54.1 |
| ICD-9-CM | 723.4, 724.4, 729.2 |
| DiseasesDB | 29522 |
| MeSH | D011843 |
Radiculopathy refers to a set of conditions in which one or more nerves are affected and do not work properly (a neuropathy). The location of the injury is at the level of the nerve root (radix = "root"). This can result in pain (radicular pain), weakness, numbness, or difficulty controlling specific muscles.[1]
In a radiculopathy, the problem occurs at or near the root of the nerve, shortly after its exit from the spinal cord. However, the pain or other symptoms often radiate to the part of the body served by that nerve. For example, a nerve root impingement in the neck can produce pain and weakness in the forearm. Likewise, an impingement in the lower back or lumbar-sacral spine can be manifested with symptoms in the foot.
The radicular pain that results from a radiculopathy should not be confused with referred pain, which is different both in mechanism and clinical features.
Polyradiculopathy refers to the condition where more than one spinal nerve root is affected.
Causes
Radiculopathy is a mechanical compression of a nerve root usually at the exit foramen or lateral recess. It may be secondary to degenerative disc disease, osteoarthritis, facet joint degeneration/hypertrophy, ligamentous hypertrophy, spondylolisthesis, or a combination of these factors. Rarer causes of radiculopathy may include radiation, diabetes mellitus, neoplastic disease, or any meningeal-based disease process. Second-stage Lyme meningitis resembles aseptic meningitis and is often associated with radiculopathies.
Mechanism of injury
Most often the radiculopathy found in the patients are located in the cervical spine, most commonly affecting C6-C8 spinal nerves.[2]
Certain injuries can also lead to radiculopathy. These injuries include lifting heavy objects improperly or suffering from a minor trauma such as a car accident. Less common causes of radiculopathy include injury caused by tumor (which can compress nerve roots locally) and diabetes (which can effectively cause ischemia or lack of blood flow to nerves).
Diagnosis

Radiculopathy is a diagnosis commonly made by physicians in primary care specialities, Chiropractic, orthopedics, physiatry, and neurology. The diagnosis may be suggested by symptoms of pain, numbness, and weakness in a pattern consistent with the distribution of a particular nerve root. Neck pain or back pain may also be present. Physical examination may reveal motor and sensory deficits in the distribution of a nerve root. In the case of cervical radiculopathy, Spurling's test may elicit or reproduce symptoms radiating down the arm. In the case of lumbosacral radiculopathy, a Straight leg raise maneuver may exacerbate radiculopathic symptoms. Deep tendon reflexes (also known as a Stretch reflex) may be diminished or absent in areas innervated by a particular nerve root.
For further workup, the American College of Radiology recommends that projectional radiography is the most appropriate initial study in all patients with chronic neck pain.[3] Two additional diagnostic tests that may be of use are magnetic resonance imaging and electrodiagnostic testing. Magnetic resonance imaging (MRI) of the portion of the spine where radiculopathy is suspected may reveal evidence of degenerative change, arthritic disease, or another explanatory lesion responsible for the patient's symptoms. Electrodiagnostic testing, consisting of NCS (Nerve conduction study) and EMG (Electromyography), is also a powerful diagnostic tool that may show nerve root injury in suspected areas. On nerve conduction studies, the pattern of diminished Compound muscle action potential and normal sensory nerve action potential may be seen given that the lesion is proximal to the Posterior root ganglion. Needle EMG is the more sensitive portion of the test, and may reveal active denervation in the distribution of the involved nerve root, and neurogenic-appearing voluntary motor units in more chronic radiculopathies. Given the key role of electrodiagnostic testing in the diagnosis of acute and chronic radiculopathies, the American Association of Neuromuscular & Electrodiagnostic Medicine has issued evidence-based practice guidelines, for the diagnosis of both cervical and lumbosacral radiculopathies.[4][5] The American Association of Neuromuscular & Electrodiagnostic Medicine has also participated in the Choosing Wisely Campaign and several of their recommendations relate to what tests are unnecessary for neck and back pain.[6]
Treatment
Ideally, effective treatment aims to resolve the underlying cause and restores the nerve root to normal function. Common conservative treatment approaches include physical therapy and chiropractic. A systematic review found moderate quality evidence that spinal manipulation is effective for the treatment of acute lumbar radiculopathy[7] and cervical radiculopathy.[8] Only low level evidence was found to support spinal manipulation for the treatment of chronic lumbar radiculopathies, and no evidence was found to exist for treatment of thoracic radiculopathy.[7]

Rehabilitation
Therapeutic exercises are frequently used in combination with many of the previously mentioned modalities and with great results. A variety of exercise regimens are available in patient treatment. An exercise regimen should be modified according to the abilities and weaknesses of the patient.[9] Stabilization of the cervicothoracic region is helpful in limiting pain and preventing re-injury. Cervical and lumbar support braces typically are not indicated for radiculopathy, and may lead to weakness of support musculature.[10] The first part of the stabilization procedure is achieving a pain free full range of motion which can be accomplished through stretching exercises. Subsequently a strengthening exercise program should be designed to restore the deconditioned cervical, shoulder girdle, and upper trunk musculature.[11] As reliance on the neck brace diminishes, an isometric exercise regimen should be introduced. This is a preferred method of exercise during the sub-acute phase because it resists atrophy and is least likely to exacerbate the condition. Single plane resistance exercises against cervical flexion, extension, bending, and rotation are used.
Surgery
While conservative approaches for rehabilitation are ideal, some patients will not improve and surgery is still an option. Patients with large cervical disk bulges may be recommended for surgery, however most often conservative management will help the herniation regress naturally.[12] Procedures such as foraminotomy, laminotomy, or discectomy may be considered by neurosurgeons and orthopedic surgeons.
Epidemiology
Cervical radiculopathy is less prevalent in the United States than lumbar radiculopathy with an occurrence rate of 83 cases per 100,000. According to the AHRQ’s 2010 National Statistics for cervical radiculopathy the most affected age group is between 45 and 64 years with 51.03% of incidents. Females are affected more frequently than males and account for 53.69% of cases. Private insurance was the payer in 41.69% of the incidents followed by Medicare with 38.81%. In 71.61% of cases the patients’ income was considered not low for their zipcode. Additionally over 50% of patients lived in large metropolitans (inner city or suburb). The South is the most severely affected region in the US with 39.27% of cases. According to a study performed in Minnesota, the most common manifestation of this set of conditions is the C7 monoradiculopathy, followed by C6.[13]
See also
References
- ↑ Eck, Jason C. "Radiculopathy". MedicineNet.com. Retrieved 12 April 2012.
- ↑ Oh, Sein; Kim, Hyung Kuk; Kwak, Jehwan; Kim, Taikon; Jang, Seong Ho; Lee, Kyu Hoon; Kim, Mi Jung; Park, Si-Bog; Han, Seung Hoon (2013). "Causes of Hand Tingling in Visual Display Terminal Workers". Annals of Rehabilitation Medicine. 37 (2): 221–8. PMC 3660483
 . PMID 23705117. doi:10.5535/arm.2013.37.2.221.
. PMID 23705117. doi:10.5535/arm.2013.37.2.221. - ↑ Gerard A Malanga. "Cervical Radiculopathy Workup". Retrieved 2017-06-29. Updated: Dec 14, 2016
- ↑ American Association of Electrodiagnostic Medicine.; So, Y. T. (1999). "Guidelines in electrodiagnostic medicine. Practice parameter for needle electromyographic evaluation of patients with suspected cervical radiculopathy" (PDF). Muscle & Nerve. Supplement. 8: S209–21. PMID 16921635.
- ↑ Cho, S. Charles; Ferrante, Mark A.; Levin, Kerry H.; Harmon, Robert L.; So, Yuen T. (2010). "Utility of electrodiagnostic testing in evaluating patients with lumbosacral radiculopathy: An evidence-based review". Muscle & Nerve. 42 (2): 276–82. PMID 20658602. doi:10.1002/mus.21759.
- ↑ http://www.choosingwisely.org/doctor-patient-lists/american-association-of-neuromuscular-electrodiagnostic-medicine/%5B%5D
- 1 2 Leininger, Brent; Bronfort, Gert; Evans, Roni; Reiter, Todd (2011). "Spinal Manipulation or Mobilization for Radiculopathy: A Systematic Review". Physical Medicine and Rehabilitation Clinics of North America. 22 (1): 105–25. PMID 21292148. doi:10.1016/j.pmr.2010.11.002.
- ↑ Zhu, Liguo; Wei, Xu; Wang, Shangquan (2015). "Does cervical spine manipulation reduce pain in people with degenerative cervical radiculopathy? A systematic review of the evidence, and a meta-analysis". Clinical Rehabilitation. 30 (2): 145–55. PMID 25681406. doi:10.1177/0269215515570382.
- ↑ Cleland, Joshua A.; Whitman, Julie M.; Fritz, Julie M.; Palmer, Jessica A. (2005). "Manual Physical Therapy, Cervical Traction, and Strengthening Exercises in Patients with Cervical Radiculopathy: A Case Series". Journal of Orthopaedic & Sports Physical Therapy. 35 (12): 802–11. PMID 16848101. doi:10.2519/jospt.2005.35.12.802.
- ↑ Muzin, S; Isaac, Z; Walker, J; Abd, O. E.; Baima, J (2007). "When should a cervical collar be used to treat neck pain?". Current Reviews in Musculoskeletal Medicine. 1 (2): 114–119. PMC 2684205 . doi:10.1007/s12178-007-9017-9.
- ↑ Saal, J. A.; Saal, J. S. (1989). "Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. An outcome study". Spine. 14 (4): 431–7. PMID 2718047. doi:10.1097/00007632-198904000-00018.
- ↑ Heckmann, J. G.; Lang, C. J.; Zöbelein, I; Laumer, R; Druschky, A; Neundörfer, B (1999). "Herniated cervical intervertebral discs with radiculopathy: An outcome study of conservatively or surgically treated patients". Journal of spinal disorders. 12 (5): 396–401. PMID 10549703. doi:10.1097/00002517-199910000-00008.
- ↑ Radhakrishnan, Kurupath; Litchy, William J.; O'Fallon, W. Michael; Kurland, Leonard T. (1994). "Epidemiology of cervical radiculopathy". Brain. 117 (2): 325–35. PMID 8186959. doi:10.1093/brain/117.2.325.
External links[1]
- Radiculopathy at the US National Library of Medicine Medical Subject Headings (MeSH)
- Symptoms
- More on Radiculopathy
- Youtube video: Spine & Nerve Health with Dr. Aaron Filler (comparing Sciatica and Piriformis Syndrome)
- Neck and Arm Pain Infographic, Cervical Radiculopathy from the Mount Sinai Hospital, New York
- Pinched nerve in neck
- Medical Terminology for Nerve Pain: Radiculopathy or Neuritis?
- Chou, Roger; Hashimoto, Robin; Friedly, Janna; Fu, Rongwei; Bougatsos, Christina; Dana, Tracy; Sullivan, Sean D.; Jarvik, Jeffrey (2015). "Epidural Corticosteroid Injections for Radiculopathy and Spinal Stenosis". Annals of Internal Medicine. 163 (5): 373–81. PMID 26302454. doi:10.7326/M15-0934. Lay summary – The New York Times (August 24, 2015).
- ↑ Pachner, A. R. (1989-10-01). "Neurologic manifestations of Lyme disease, the new "great imitator"". Reviews of Infectious Diseases. 11 Suppl 6: S1482–1486. ISSN 0162-0886. PMID 2682960. doi:10.1093/clinids/11.supplement_6.s1482.