Overdiagnosis
Overdiagnosis is the diagnosis of "disease" that will never cause symptoms or death during a patient's ordinarily expected lifetime.[1] Overdiagnosis is a side effect of screening for early forms of disease. Although screening saves lives in some cases, in others it may turn people into patients unnecessarily and may lead to treatments that do no good and perhaps do harm. Given the tremendous variability that is normal in biology, it is inherent that the more one screens, the more incidental findings will be found. For a large percentage of them, the most appropriate medical response is to recognize them as something that does not require intervention; but determining which action a particular finding warrants ("ignoring", watchful waiting, or intervention) can be very difficult, whether because the differential diagnosis is uncertain or because the risk ratio is uncertain (risks posed by intervention, namely, adverse events, versus risks posed by not intervening).
Overdiagnosis occurs when a disease is diagnosed correctly, but the diagnosis is irrelevant. A correct diagnosis may be irrelevant because treatment for the disease is not available, not needed, or not wanted. Some people contend that the term "overdiagnosis" is inappropriate, and that "overtreatment" is more representative of the phenomenon.
Because most people who are diagnosed are also treated, it is difficult to assess whether overdiagnosis has occurred in an individual. Overdiagnosis in an individual cannot be determined during life. Overdiagnosis is only certain when an individual remains untreated, never develops symptoms of the disease and dies of something else. Thus most of the inferences about overdiagnosis comes from the study of populations. Rapidly rising rates of testing and disease diagnosis in the setting of stable rates of the feared outcome of the disease (e.g. death) are highly suggestive of overdiagnosis. Most compelling, however, is evidence from a randomized trial of a screening test intended to detect pre-clinical disease. A persistent excess of detected disease in the tested group years after the trial is completed constitutes the best evidence that overdiagnosis has occurred.
Although overdiagnosis is potentially applicable to the diagnosis of any disease, its origin is in cancer screening – the systematic evaluation of asymptomatic patients to detect early forms of cancer.[2] The central harm of cancer screening is overdiagnosis – the detection of abnormalities that meet the pathologic definition of cancer (under the microscope) but will never progress to cause symptoms or death during a patient's ordinarily expected lifetime.
Overdiagnosis and the variability of cancer progression
Cancer screening is the effort to detect cancer early, during its pre-clinical phase — the time period that begins with an abnormal cell and ends when the patient notices symptoms from the cancer. It has long been known that some people have cancers with short pre-clinical phases (fast-growing, aggressive cancers), while others have cancers with long pre-clinical phases (slow-growing cancers). And this heterogeneity has an unfortunate implication: namely, screening tends to disproportionately detect slow-growing cancers (because they are accessible to be detected for a long period of time) and disproportionately miss the fast-growing cancers (because they are only accessible to be detected for a short period of time) – the very cancers we would most like to catch. For more information, see Screening (medicine)#Length time bias.
This long-standing model has a hidden assumption: namely, that all cancers inevitably progress. But some pre-clinical cancers will not progress to cause problems for patients. And if screening (or testing for some other reason) detects these cancers, overdiagnosis has occurred.
The figure below depicts the heterogeneity of cancer progression using 4 arrows to represent 4 categories of cancer progression.
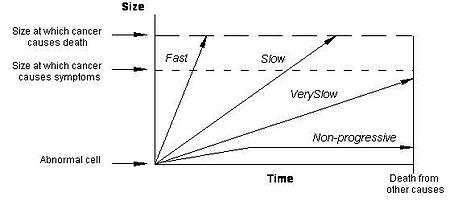
The arrow labeled "Fast" represents a fast-growing cancer, one that quickly leads to symptoms and to death. These are the worst forms of cancer and unfortunately often appear in the interval between screening tests. The arrow labeled "Slow" represents a slow-growing cancer, one that leads to symptoms and death but only after many years. These are the cancers for which screening has arguably the greatest beneficial impact.
The arrow labeled "Very Slow" represents a cancer that never causes problems because it is growing very slowly. If a cancer grows slowly enough, then patients will die of some other cause before the cancer gets big enough to produce symptoms. This is particularly likely with small cancers in the elderly – prostate cancer in older men serves as the most prominent clinical example.
The arrow labeled "Non-progressive" represents a cancer that never causes problems because it is not growing at all. In other words, there are cellular abnormalities that meet the pathologic definition of cancer but never grow to cause symptoms – alternatively, they may grow and then regress. Although the concept of non-progressive cancers may seem implausible, basic scientists have begun to uncover biologic mechanisms that halt the progression of cancer.[3][4][5] Some cancers outgrow their blood supply (and are starved), others are recognized by the host's immune system (and are successfully contained), and some are not that aggressive in the first place.
Overdiagnosis occurs when either "Non-progressive" cancers or "Very Slow" growing cancers (more precisely, at a slow enough pace that individuals die from something else before the cancer ever causes symptoms) are detected. These two forms of cancer are collectively referred to as pseudodisease - literally false disease. Since the word "disease" implies something that makes, or will make, a person feel sick (something that causes symptoms), pseudodisease is an appropriate word for describing these abnormalities. Thus, another definition of overdiagnosis is simply the detection of pseudodisease.
Evidence for overdiagnosis in cancer
The phenomenon of overdiagnosis is most widely understood in prostate cancer.[6] A dramatic increase in the number of new cases of prostate cancer was observed following the introduction of the PSA (prostate specific antigen) screening test. Because of the problem of overdiagnosis most organizations recommend against prostate cancer screening in men with limited life expectancy - generally defined as less than 10 years (see also prostate cancer screening).
Overdiagnosis has been identified in mammographic screening for breast cancer.[7][8] Long-term follow-up of the Malmo randomized trial of mammography found a persistent excess of 115 breast cancers in the screened group 15 years after the trial was completed (a 10% rate of overdiagnosis).[9] In a letter to the editor, authors not associated with the original study of the data from the randomized clinical trial argued that one-quarter of mammographically detected breast cancers represent overdiagnosis.[10]
Overdiagnosis has also been identified in chest x-ray screening for lung cancer.[11] Long-term follow-up of the Mayo Clinic randomized trial of screening with chest x-rays and sputum cytology found a persistent excess of 46 lung cancer cases in the screened group 13 years after the trial was completed,[12] suggesting that 20-40% of lung cancers detected by conventional x-ray screening represent overdiagnosis. There is considerable evidence that the problem of overdiagnosis is much greater for lung cancer screening using spiral-CT scans[13]
Overdiagnosis has also been associated with early detection in a variety of other cancers, including neuroblastoma,[14][15] melanoma,[16] and thyroid cancer.[17] In fact, some degree of overdiagnosis in cancer early detection is probably the rule, not the exception.
Evidence for overdiagnosis of infectious diseases
Issues with overdiagnosis of infectious diseases, such as malaria or typhoid fever, persist in many regions around the world. For example, malaria overdiagnosis is well-documented in African countries [18][19] and results in over-inflation of actual malaria rates reported at the local and national levels.[20] Health facilities tend to over-diagnose malaria in patients presenting with symptoms such as fever, due to traditional perceptions (for example any fever being equivalent to malaria) and issues related to laboratory testing (see Diagnosis of malaria).[21][22] Therefore, malaria overdiagnosis leads to under management of other fever-inducing conditions,[19] but also to over-prescription of antimalarial drugs.[23]
Harms of overdiagnosis
Overdiagnosed patients cannot benefit from the detection and treatment of their "cancer", because the cancer was never destined to cause symptoms or death. They can only be harmed. There are three categories of harm associated with overdiagnosis:
- Physical effects of unnecessary diagnosis and treatment: All medical interventions have side effects. This is particularly true of cancer treatments. Surgery, radiation and chemotherapy all pose varying morbidity and mortality risks.
- Psychological effects: there is a burden for an individual simply being labeled as "diseased" (e.g. the burden of being labeled a "cancer patient") and an associated increased sense of vulnerability.
- Economic burden: Not only the associated cost of treatment (from which the patient cannot benefit, because the disease posed no threat), but also - at least, in the current health care system in the United States - a potential increase in the cost of health insurance or even an inability to procure it (e.g. the diagnosis creates a pre-existing condition that affects health insurance). Similar issues may arise with life insurance. Unlike health insurance, life insurance does not fall under the scope of the Affordable Care Act, thus insurers have even more leeway in denying or reducing coverage or inflating premiums due to the patient's condition.
While many identify false positive results as the major downside to cancer screening, there are data to suggest that - when patients are informed about overdiagnosis - they are much more concerned about overdiagnosis than false positive results.[24]
Distinction among overdiagnosis, misdiagnosis, and false positive results
Overdiagnosis is often confused with the term "false positive" test results, and with misdiagnosis, but they are three distinct concepts. A false positive test result refers to a test that suggests the presence of disease, but is ultimately proved to be in error (usually by a second, more precise test). Patients with false positive test results are told they don't have disease and are not treated; overdiagnosed patients are told they have disease and generally receive treatment. Misdiagnosed patients do not have the condition at all, or have a totally different condition, but are treated anyway.
| Overdiagnosis | False Positive Results | Misdiagnosis | |
|---|---|---|---|
| Definition | Detection of a "disease" that will never cause symptoms or death during a patients lifetime | A "false alarm" – an initial test result that suggests the presence of disease, but it is later proved that no disease is present. | Diagnosis of a disease that the patient does not in fact have (either they are "normal" or they have a different condition) |
| Patient experience | Told they have the disease | Told that the test was wrong and they do not have the disease | Told they have the disease |
| Physician action | Generally, initiates treatment | Reassurance | Generally, initiates treatment |
| Potential Harms |
|
|
|
Overdiagnosis bias in survival statistics
Overdiagnosis, by contributing disproportionately to early diagnosis of lethal conditions, has the effect of inflating survival statistics.[25][26] The more overdiagnosis, the better survival appears and it seems that early diagnosis is doing good. More testing is encouraged, leading to more overdiagnosis.
Overdiagnosis always inflates survival statistics. Survival rates (e.g. 5-year survival, 10-year survival) are calculated as the proportion of patients that are alive after a fixed period (e.g. 5 or 10 years) following diagnosis. Overdiagnosis inflates both the numerator and denominator of the survival statistic. The figure below shows how overdiagnosis - the detection of pseudodisease - inflates the survival statistic even when the number of deaths is stable.
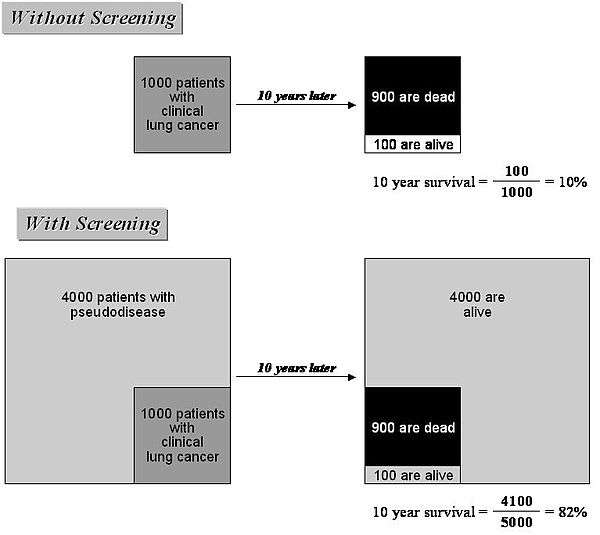
Imagine that there is no pseudodisease detected in current practice and that among 1000 patients diagnosed, only 100 are alive 10 years later (i.e. the 10-year survival is 100 divided by 1000 or 10%). Now imagine that in addition to identifying these cancers, spiral CT scanning also identifies 4000 patients with pseudodisease - all of whom survive 10 years, since they have non-progressive cancer. The new 10-year survival will include these patients in both the numerator and denominator - leading to a 10-year survival of 4100 divided by 5000 or 82%. Note that even though survival has changed dramatically, the number of people who die has not changed – under either condition 900 patients have died. This example demonstrates how survival rates can be increased by overdiagnosis, even if no one avoids death.
Solutions to overdiagnosis
Removing "cancer" from names of low-risk diagnoses
It has been proposed that some pre-malignant conditions have the words cancer or carcinoma removed from their name.[27] Another proposal is to name conditions "IDLE (indolent lesions of epithelial origin)".[27]
An analogy can be made with Neisseria meningitides, a bacterium present in 5–15% of the adult population that can potentially cause life-threatening meningitis. To say that those who carry the microorganism "have meningitis" would be misleading.
See also
- Disease mongering
- False positive
- Medicalization
- Interventionism (medicine)
- Patient education
- Schooliosis
- Screening (medicine)
References
- ↑ Welch, H. Gilbert; Black, William C. (2010-05-05). "Overdiagnosis in cancer". Journal of the National Cancer Institute. 102 (9): 605–613. ISSN 1460-2105. PMID 20413742. doi:10.1093/jnci/djq099.
- ↑ Welch HG. Should I Be Tested for Cancer? Maybe Not and Here’s Why. University of California Press (2006 paperback, 2004 hardback)
- ↑ Mooi WJ, Peeper DS. Oncogene-induced cell senescence--halting on the road to cancer. N Engl J Med. 2006;355:1037-46
- ↑ Folkman J, Kalluri R. Cancer without disease. Nature. 2004;427:787.
- ↑ Serrano M. Cancer Regression by Senescence. New Engl J Med 2007 356:1996-97.
- ↑ Etzioni R, Penson DF, Legler JM, et al. Overdiagnosis due to prostate-specific antigen screening: lessons from U.S. prostate cancer incidence trends. J Natl Cancer Inst. 2002;94:981-90.
- ↑ Zahl PH, Strand BH, Mæhlen J. Breast cancer incidence in Norway and Sweden during introduction of nation-wide screening: prospective cohort study. BMJ 2004; 328: 921-4.
- ↑ Gotzsche P, Nielsen M. Screening for breast cancer with mammography. Cochrane Database of Systematic Reviews 2006.
- ↑ Zackrisson S, Andersson I, Janzon L, Manjer J, Garne JP. Rate of over-diagnosis of breast cancer 15 years after end of Malmö mammographic screening trial: follow-up study. BMJ 2006; 332: 689-692.
- ↑ Welch HG, Schwartz LM, Woloshin S. Ramifications of screening for breast cancer: 1 in 4 cancers detected by mammography are pseudocancers. BMJ. 2006;332:727.
- ↑ Black WC. Overdiagnosis: An underrecognized cause of confusion and harm in cancer screening. J Natl Cancer Inst. 2000 Aug 16;92(16):1280-2.
- ↑ Marcus PM, Bergstralh EJ, Fagerstrom RM, Williams DE, Fontana R, Taylor WF, Prorok PC. Lung cancer mortality in the Mayo Lung Project: impact of extended follow-up. J Natl Cancer Inst. 2000;92:1308-16.
- ↑ Welch HG, Woloshin S, Schwartz LM, Gordis L, Gøtzsche PC, Harris R, Kramer BS, Ransohoff DF. Overstating the evidence for lung cancer screening: the International Early Lung Cancer Action Program (I-ELCAP) study. Arch Intern Med. 2007;167:2289-95.
- ↑ Schilling FH, Spix C, Berthold F, et al. Neuroblastoma screening at one year of age. N Engl J Med 2002 346:1047-1053.
- ↑ Yamamoto K, Hanada R, Kikuchi A, et al. Spontaneous regression of localized neuroblastoma detected by mass screening. J Clin Oncol 1998;16:1265-69.
- ↑ Welch HG, Woloshin S, Schwartz LM. Skin biopsy rates and incidence of melanoma: population based ecological study. BMJ. 2005;331:481-4.
- ↑ Davies L, Welch HG. The increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA 2006;295;2164-7.
- ↑ Ghai, Ria R.; Thurber, Mary I.; El Bakry, Azza; Chapman, Colin A.; Goldberg, Tony L. (2016-09-07). "Multi-method assessment of patients with febrile illness reveals over-diagnosis of malaria in rural Uganda". Malaria Journal. 15: 460. ISSN 1475-2875. PMC 5015337
 . PMID 27604542. doi:10.1186/s12936-016-1502-4.
. PMID 27604542. doi:10.1186/s12936-016-1502-4. - 1 2 Reyburn, Hugh; Mbatia, Redepmta; Drakeley, Chris; Carneiro, Ilona; Mwakasungula, Emmanuel; Mwerinde, Ombeni; Saganda, Kapalala; Shao, John; Kitua, Andrew (2004-11-20). "Overdiagnosis of malaria in patients with severe febrile illness in Tanzania: a prospective study". BMJ (Clinical research ed.). 329 (7476): 1212. ISSN 1756-1833. PMC 529364 . PMID 15542534. doi:10.1136/bmj.38251.658229.55.
- ↑ Salomão, Cristolde A.; Sacarlal, Jahit; Chilundo, Baltazar; Gudo, Eduardo Samo (2015-12-01). "Prescription practices for malaria in Mozambique: poor adherence to the national protocols for malaria treatment in 22 public health facilities". Malaria Journal. 14: 483. ISSN 1475-2875. PMC 4667420 . PMID 26628068. doi:10.1186/s12936-015-0996-5.
- ↑ Yegorov, Sergey; Galiwango, Ronald M.; Ssemaganda, Aloysious; Muwanga, Moses; Wesonga, Irene; Miiro, George; Drajole, David A.; Kain, Kevin C.; Kiwanuka, Noah (2016-11-14). "Low prevalence of laboratory-confirmed malaria in clinically diagnosed adult women from the Wakiso district of Uganda". Malaria Journal. 15 (1): 555. ISSN 1475-2875. PMC 5109652 . PMID 27842555. doi:10.1186/s12936-016-1604-z.
- ↑ Bell, David; Wongsrichanalai, Chansuda; Barnwell, John W. (2006-09-01). "Ensuring quality and access for malaria diagnosis: how can it be achieved?". Nature Reviews. Microbiology. 4 (9): 682–695. ISSN 1740-1534. PMID 16912713. doi:10.1038/nrmicro1474.
- ↑ Mwanziva, Charles; Shekalaghe, Seif; Ndaro, Arnold; Mengerink, Bianca; Megiroo, Simon; Mosha, Frank; Sauerwein, Robert; Drakeley, Chris; Gosling, Roly (2008-11-05). "Overuse of artemisinin-combination therapy in Mto wa Mbu (river of mosquitoes), an area misinterpreted as high endemic for malaria". Malaria Journal. 7: 232. ISSN 1475-2875. PMC 2588630 . PMID 18986520. doi:10.1186/1475-2875-7-232.
- ↑ Schwartz LM, Woloshin S, Sox HC, Fischhoff B, Welch HG. US women's attitudes to false positive mammography results and detection of ductal carcinoma in situ: cross sectional survey. BMJ. 2000;320:1635-40.
- ↑ Black W, Welch H. Advances in diagnostic imaging and overestimations of disease prevalence and the benefits of therapy. N Engl J Med 1993;328:1237-43.
- ↑ Welch H, Schwartz L, Woloshin S. Are increasing 5-year survival rates evidence of success against cancer? . JAMA 2000;283:1975-78.
- 1 2 Esserman LJ, Thompson IM, Reid B (2013). "Overdiagnosis and Overtreatment in Cancer: An Opportunity for Improvement.". JAMA. 310 (8): 797–8. PMID 23896967. doi:10.1001/jama.2013.108415.
Further reading
- Welch, H. Gilbert, Schwartz, Lisa. Overdiagnosed: Making People Sick in the Pursuit of Health. Beacon Press; 2011-01-18. ISBN 9780807022009.