Ingrown nail
| Ingrown nail | |
|---|---|
 | |
| An ingrown toenail | |
| Classification and external resources | |
| Specialty | Orthopedics |
| ICD-10 | L60.0 |
| ICD-9-CM | 703.0 |
| DiseasesDB | 29440 |
| MedlinePlus | 001237 |
| eMedicine | emerg/593 ped/942 |
An ingrown nail (also known as onychocryptosis from Greek: ὄνυξ (onyx, "nail") + κρυπτός (kryptos, "hidden") or unguis incarnates)[1] is a common form of nail disease. It is an often painful condition in which the nail grows so that it cuts into one or both sides of the paronychium or nail bed.
The common opinion is that the nail enters inside the paronychium, but an ingrown toenail can simply be overgrown toe skin.[2] The condition starts from a microbial inflammation of the paronychium, then a granuloma, which results in a nail buried inside of the granuloma. While ingrown nails can occur in the nails of both the hands and the feet , they occur most commonly with the toenails.
A true ingrown toenail, is caused by the actual penetration of flesh by a sliver of nail.[3]
Signs and symptoms
Symptoms of an ingrown nail include pain along the margins of the nail (caused by hypergranulation that occurs around the aforementioned margins), worsening of pain when wearing tight footwear, and sensitivity to pressure of any kind, even the weight of bedsheets. Bumping of an affected toe can produce sharp and even excruciating pain as the tissue is punctured further by the nail. By the very nature of the condition, ingrown nails become easily infected unless special care is taken early to treat the condition by keeping the area clean. Signs of infection include redness and swelling of the area around the nail, drainage of [pus], and watery discharge tinged with blood. The main symptom is swelling at the base of the nail on the side the nail is ingrowing (may be both sides).
Ingrown nail should not be confused with a similar nail disorder: convex nail, Nor with other painful nail conditions such as involuted nails, or the presence of small corns, callus or debris down the nail sulci (grooves on either .
Causes
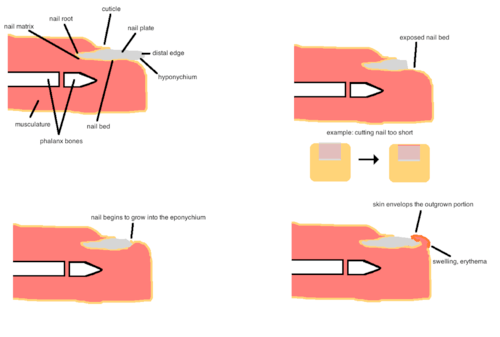
The main cause of onychocryptosis is footwear, particularly ill-fitting, that includes shoes with inadequate toe-box room and tight stockings that apply pressure to the top or side of the foot.[4][5] Other causes may include the damp atmosphere of enclosed shoes, which soften the nail-plate and cause swelling on the epidermal keratin, which eventually increases the convex arch permanently, genetics, trauma, and disease. Improper cutting of the nail may cause the nail to cut into the side-fold skin from growth and impact, whether or not the nail is "ingrown" (true onychocryptosis). The nail bends inwards or upwards depending on the angle of its cut. If the cutting tool, such as scissors, is in an attitude where the lower blade is closer to the toe than the upper blade, that will cause the toenail to grow upwards from its base, and vice versa. The process is visible along the nail as it grows, appearing as a warp advancing to the end of the nail. The upper corners turn more easily than the center of the nail tip. As people cut their nails by holding the tool always at the same angle, they induce these conditions by accident; as the nail turns closer to the skin, it becomes harder to fit the lower blade in the right attitude under the nail. When cutting a nail, it is not just the correct angle that is important, but also how short it is cut. A shorter cut will bend the nail more, unless the cut is even on both top and bottom of the nail.
Causes may include:
- Shoes causing a bunching of the toes in the developmental stages of the foot (frequently in people under 21), which can cause the nail to curl and dig into the skin. This is particularly the case in ill-fitting shoes that are too narrow or too short, but any toed shoes may cause an ingrown nail.
- Poor nail-care, including cutting the nail too short, rounded off at the tip or peeled off at the edges instead of being cut straight across, or breaking a toenail.
- Trauma to the nail plate or toe, which can occur by stubbing the toenail, dropping things on the toe or going through the end of the shoes (as during sports or other vigorous activity), can cause the flesh to become injured and the nail to grow irregularly and press into the flesh
- Predisposition, such as abnormally shaped nail beds, nail deformities caused by diseases, or a genetic susceptibility increases the chance of an ingrown nail, but the ingrowth cannot occur without pressure from a shoe.
- A bacterial infection, treatable with antibiotics. See "treatments".
One study compared patients with ingrown toenails to healthy controls and found no difference in the shape of toenails between patients and the control group, they suggested that treatment should not be based on the correction of a non-existent nail deformity.[6] Ingrown toenails are caused by weight-bearing (activities such as walking, running, etc.) in patients that have too much soft skin tissue on the sides of their nail. Weight bearing causes this excessive amount of skin to bulge up along the sides of the nail. The pressure on the skin around the nail results in the tissue being damaged, resulting in swelling, redness and infection. In the past (and currently) the most common treatments are mainly directed at the nail (paradigm paralysis). Treatments often include part or full removal of the nail. Since the nail is normal and the problem of too much skin around the nail was not treated, the results are; return of the problem, a deformity in the nail, or the mutilation of the nail.
Prevention
The most common place for ingrown nails is in the big toe, but ingrowth can occur on any nail. Ingrown nails can be avoided by cutting nails straight across; not along a curve, not too short, and no shorter than the flesh around it. Footwear that is too small or too narrow, or with too shallow of a 'toe box', will exacerbate any underlying problem with a toenail. Sharp square corners may be uncomfortable and cause snagging on socks. Proper cutting leaves the leading edge of the nail free of the flesh, precluding it from growing into the toe. Filing of the corner is reasonable. Some nails require cutting of the corners far back to remove edges that dig into the flesh, this is often done as a partial wedge resection at a podiatrist's office. Ingrown toe nails can be caused by injury, commonly blunt trauma where the flesh is pressed against the nail causing a small cut that swells. Also, injury to the nail can cause it to grow abnormally, making it wider or thicker than normal or even bulged or crooked.
Management
The treatment of an ingrown toenail partly depends on how severe it is.[7]
Conservative treatment
In mild to moderate cases conservative treatment with warm water and salt soaks, antibacterial ointment, and the use of dental floss, or a gutter splint to provide a track along which the nail may grow is possible. If conservative treatment of a minor ingrown toenail does not succeed or if the ingrown toenail is severe, surgical treatment may be required.[7] A "gutter splint" may be improvised by slicing a cotton tipped wooden applicator diagonally to form a bevel and using this to insert a wisp of cotton from the applicator head under the nail to lift it from the underlying skin after a foot soak.[8]
Surgery

Surgical treatment for an ingrown nail is carried out by a podiatrist – a foot and ankle specialist. This is typically an in-office procedure requiring local anesthesia and special surgical instruments. The surgical approach is the removal of the offending part of the nail plate known as a wedge resection.[7] If the ingrown toenail recurs despite this treatment, destruction of the sides of the nail with chemicals or excision is done; this is known as a matrixcestomy.[7] Antibiotics may be used post procedure but are not recommended as they may delay healing.[7]
Nail bracing
A less widely used treatment for ingrown toenails is nail bracing. Nail braces work by gently lifting the sides of the toenail and eventually retraining the nail to grow to a flatter shape over time. The total time needed for the nail to be reshaped is one full nail growth or about 18 months.[9] There are two main types of nail braces: adhesive and hooked. Adhesive nail braces are generally made of a thin strip of composite material that is glued to the top of the nail. The strip naturally tries to return to a flat state and lifts the edges of the nails in the process. Hooked nail braces consist of a hook (usually made of dental wire) placed under either side of the nail with some type of tensioning system pulling the hooks together.
Due to the curved shape of the nail, the tensioning device rests on the higher middle of the nail by applying upward pressure to the sides of the nail. In studies of diabetics, who need to avoid surgery when possible, nail bracing was found to be effective at providing immediate relief as well as long term relief.[10]
References
- ↑ James, William; Berger, Timothy; Elston, Dirk (2002). Andrews' Diseases of the Skin: Clinical Dermatology (10th ed.). Saunders. p. 789. ISBN 0-7216-2921-0.
- ↑ Chapeskie H (2008). "Ingrown toenail or overgrown toe skin?". Canadian Family Physician. 54 (11): 1561–2. PMC 2592332
 . PMID 19005128.
. PMID 19005128. - ↑ Ingrown Toenail: http://www.nhs.uk/conditions/ingrown-toenail/Pages/Introduction.aspx
- ↑ SHULMAN, Pod.D, SAMUEL B. (1949). "Survey in China and India of Feet That Have Never Worn Shoes". The Journal of the National Association of Chiropodists. Retrieved 27 September 2012.
- ↑ Howell, Phd, Dr Daniel (2010). The Barefoot Book. Hunter House.
- ↑ Pearson HJ, Bury RN, Wapples J, Watkin DF (November 1987). "Ingrowing toenails: is there a nail abnormality? A prospective study". J Bone Joint Surg Br. 69 (5): 840–2. PMID 3680356.
- 1 2 3 4 5 Heidelbaugh, JJ; Lee, H (15 February 2009). "Management of the ingrown toenail.". American family physician. 79 (4): 303–8. PMID 19235497.
- ↑ American Association of Orthopedic Specialists, "ingrown toenail" at http://orthoinfo.aaos.org/topic.cfm?topic=a00154
- ↑ http://toenail_brace.atheart.dk/method_braces_ingrown_toenails.htm: http://toenail_brace.atheart.dk/method_braces_ingrown_toenails.htm
- ↑ "Long-term results of nail brace application in diabetic patients with ingrown nails.". Dermatol Surg. 34 (1): 84–6; discussion 86–7. Jan 2008. PMID 18053045. doi:10.1111/j.1524-4725.2007.34013.x.
Further reading
- Aksakal AB, Ozsoy E, Gürer M (2003). "Silicone gel sheeting for the management and prevention of onychocryptosis". Dermatol Surg. 29 (3): 261–4. PMID 12614420. doi:10.1046/j.1524-4725.2003.29061.x.
- Boll OF (1945). "Surgical correction of ingrowing toenails". J Natl Assoc Chiroprod. 35: 8–9.
- Chapeskie H (2008). "Ingrown toenail or overgrown toe skin?". Canadian Family Physician. 54 (11): 1561–1562. PMC 2592332 . PMID 19005128.
- Kominsky SJ, Daniels MD (2000). "A modified approach to the phenol and alcohol chemical partial matrixectomy". J Am Podiatr Med Assoc. 90 (4): 208–10. PMID 10800276. doi:10.7547/87507315-90-4-208.
- Rounding C, Bloomfield S (2005). Rounding C, ed. "Surgical treatments for ingrowing toenails". Cochrane Database Syst Rev (2): CD001541. PMID 15846620. doi:10.1002/14651858.CD001541.pub2.
- Boberg JS, Frederiksen MS, Harton FM (2002). "Scientific analysis of phenol nail surgery". J Am Podiatr Med Assoc. 92 (10): 575–9. PMID 12438504.
| Wikimedia Commons has media related to Ingrown nail. |