Dipping tobacco
Dipping tobacco is a type of finely ground or shredded, moistened smokeless tobacco product. It is commonly and idiomatically known by various terms—most often as dip and sometimes as rub. It is used by placing a lump, pinch, or "dip" of tobacco between the lip and the gum. The act of using it is called dipping. Typically, before dipping, the act of "packing" is performed, where the user places the "can" in between their thumb and middle finger, then flicks their index finger onto the lid of the can. Dip is colloquially called "chew", "snuff", or "chaw" among other terms; because of this, it is sometimes confused with other tobacco products—namely nasal/dry snuff.
History
Dipping tobacco evolved from the use of dry snuff in early American history. Up until the late 1700s, dry snuff was taken nasally, but then early Americans would take snuff orally by chewing the end of a twig until it resembled a brush, and then "dipping" the twig in the snuff and placing it in their mouths until the snuff dissolved.[1] Using dry snuff orally eventually evolved into modern day moist snuff, with Copenhagen introduced in 1822, and Skoal introduced in 1934. Most varieties of dipping tobacco are much more recent inventions.
Today, moist snuff is available throughout the United States. However, it is typically more popular in rural areas and the South than in large cities. Dipping tobacco is predominately used by males. Also, dipping tobacco has a similar presence in Canada.
Description


Dipping tobacco is packaged in "tins", although they are not typically completely metal anymore. Dipping tobacco is also available in "rolls", "logs", or "sleeves", which is a package of 5 tins of tobacco, a similar concept to that of a carton of cigarettes. Ten tin rolls were also available in the past. Another package of dipping tobacco is the "tub", available in only select brands, equivalent to 6, 10, or 12 tins.
Before opening the can/tin of tobacco, users typically "pack" the tin, similar to how cigarette smokers pack a pack of cigarettes. This is done by placing one's thumb and middle finger on the sides of the tin, and then quickly turning the tin and flicking the wrist so that one's index finger taps the top of the tin.
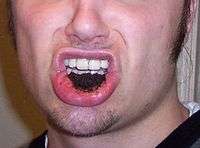
Unlike snus, which is most often placed between the upper lip and gum, dip users or "dippers" tend to use the lower. Dipping in the upper lip is unusual, though when done, it is colloquially termed an "upper decker" or "top lip dip". The dip rests on the inside lining of the mouth for a period depending upon the user's preference—often 20–40 minutes. Nicotine and other alkaloids found in tobacco are absorbed in saliva sublabially by the inferior or superior labial arteries. Buccal and sublingual absorption may also occur.
Unlike snus, dip often causes the user to produce excess saliva during the act of dipping. This is typically expectorated onto the ground or in a container, because swallowing the saliva-tobacco mixture can cause irritation to the esophagus and induce nausea and vomiting. Spittoons can be used, but often users will simply use an empty plastic bottle or a mudjug, a portable spittoon. Smokeless tobacco is sometimes used in the workplace by employees, especially if the employer does not provide many cigarette breaks or if the employee is consistently using both hands during work (which doesn't provide opportunities for cigarette smoking). Smokeless tobacco is popular in many industrial areas where there is a safety risk in having an open flame, such as oil rigs or refineries.
Etymology and terminology
Dipping tobacco was first popularized and marketed as moist snuff in the 1800s. The term "snuff" in this context is an English cognate of the aforementioned "snus", from Swedish. Dipping tobacco's Scandinavian roots impart a noticeable legacy on modern American brands such as Copenhagen and Skoal (referring to the interlinguistic term skål, which in Norwegian, Danish, Icelandic, Faroese and Swedish roughly translates to "cheers", implying a toast).
Cut sizes
The difference between cut sizes are the length of the strands of dip.
Common cut sizes
- Fat cuts are a little longer, flatter, and softer than long cut.
- Extra Long cuts are a little longer than long cut.
- Wide cuts are long cut, just a little wider.
- Long cuts are the most widely available cut size.
- Fine cuts/snuffs are slightly larger than sand or coffee grounds.
- Pouches hold fine cut or snuff tobacco in a small, teabag-like pouch. They are initially less messy because the tobacco won't fall out of the user's fingers and mouth. Dipping tobacco in pouches resemble snus "portions", but the difference between these two products lies in the way the tobacco is processed. Dipping tobacco (including pouched products) undergoes fermentation, whereas tobacco in snus is pasteurized. In addition to regular sized pouches, smaller sized pouches, known as Bandits, are also available in the Skoal brand, Grizzly brand, and Copenhagen brand.
Unique cut sizes
The following cuts are either unique to one brand of dipping tobacco or are extremely rare.
- Mid cuts are comparable to small granules at about 1 mm cubed. Mid cuts are extremely rare; the original version of Copenhagen Black is the only dip marketed as a mid cut that has made it to the market. However, many consider some products marketed as long cuts to be mid cuts, notably Copenhagen Long Cut Original.
- ReadyCut is a cut produced only by Skoal (introduced in 2012) which consists of a compressed cube of long cut. As it gets moist from saliva in the mouth, it automatically conforms to the user's mouth.
- Wide cut is a new cut introduced by Grizzly in select markets. It consists of wider strands than long cut. Grizzly Wide Cut Wintergreen is the only wide cut available.
Flavoring
Dipping tobacco is typically flavored. Most common flavors include wintergreen, mint, straight, and natural. Fruit flavors are also available and can include peach, citrus, berry, cherry, apple, and grape. Copenhagen also produces two alcohol-flavored dips, Cope Whiskey Blend and Copenhagen Black (bourbon flavored).
Health issues
Effects
Dipping tobacco, like other tobacco products, contains the stimulant nicotine. Effects include increased heart rate, an increase in systolic blood pressure, and an increase in adrenaline.[2]
Long-term effects
Long term use results in whitening of the oral mucosa, termed smokeless tobacco keratosis. There is relatively low risk of transformation of this lesion into mouth cancer (sometimes verrucous carcinoma). Dipping tobacco is believed to cause fatal oral cancers, tooth and gum loss. Associated cancers include: tongue cancer, lip cancer, cheek cancer, gum cancer, throat cancer, and cancer in the roof and floor of the mouth.[3]
In a comprehensive review of all reports from previous years, one study noted "The use of moist snuff and chewing tobacco imposes minimal risks for cancers of the oral cavity and other upper respiratory sites, with relative risks ranging from 0.6 to 1.7."[4] SEER, the Surveillance Epidemiology and End Results program of the National Cancer Institute, noted in 2012 that there were 3.6 cases of oral cancer among 100,000 smokeless tobacco users each year, the same rate seen in non-exposed men.[5]
Cardiovascular effects
Studies are inconclusive as to how significantly smokeless tobacco affects users' cardiovascular systems, but it has been suggested that it may have less nicotine than cigarettes. One study states that, "Although the evidence is not conclusive, the adverse cardiovascular effects of smokeless tobacco use are less than those caused by smoking but are more than those found in non-users."[6] Other studies also indicate that smokeless tobacco related cardiovascular risks are lower than that of smoked tobacco.[7][8] One study states that smokeless tobacco use has a "positive effect on cardiovascular risk factors in young physically fit men."[9] However, one Indian study from the state of Rajasthan states, "There is a significantly greater prevalence of multiple cardiovascular risk factors obesity, resting tachycardia, hypertension, high total and LDL cholesterol, and low HDL cholesterol, and electrocardiographic changes in tobacco users, chewing or smoking, as compared-to tobacco non-users. Chewing tobacco is associated with similar cardiovascular risk as smoking."[10]
Due to contrasting results in studies, many conclude that further research should be done on the cardiovascular risks of smokeless tobacco.[11][12]
Addiction potential
Smokeless tobacco contains nicotine, which is addictive thus the primary reinforcing agent.
According to European Union policy advice, Scandinavian or some American smokeless tobaccos (specifically snus) may be up to 90% less hazardous than cigarette smoking.[13] However, the habit is still addictive.
Taxation and restriction of smoking is causing more smokeless tobacco use as "substitution." There have been public health debates regarding risk-reduction for smokers and the reconsideration of smokeless tobacco risks. "...There is a substantial body of informed and independent opinion that sees the value of harm reduction strategies based on smokeless tobacco."[14]
Additives
The amount of nicotine absorbed can be controlled by different cutting of the tobacco, increasing the nicotine concentration and raising the pH of the tobacco by adding various salts.[15] An alkaline pH causes more nicotine to be absorbed, especially the free, unprotonated form, but is irritating to the mucosa. Nicotine itself can also irritate the mucosa.
List of brands
The following is a partial list of brands of dipping tobacco. Other tobacco products, such as chewing tobacco and snus, are excluded.[16]
- Copenhagen
- Grizzly
- Happy Days
- Husky
- Kodiak
- Red Man
- Red Seal
- Rooster (discontinued in 2009)
- Skoal
- Timber Wolf
Legality
Several countries have banned the sale (and in some cases the import) of dipping tobacco. Sale of dipping tobacco was banned in South Australia in 1986 and across the country in 1991[17] and in most of the EU nations in 1993.[18] Sweden was exempt from this ban because of the traditionally high usage of snus in that country.
In the United States, the Family Smoking Prevention and Tobacco Control Act gives the Food and Drug Administration the power to regulate the tobacco industry.[19] This law prohibits the sale of dipping tobacco to anyone under the age of 18, restricts tobacco product advertising and marketing directed to younger audiences, and requires bigger, more prominent warning labels for dipping tobacco products.[20]
Taxation
In the United States, the federal government taxes dipping tobacco at $0.5033 per pound or $0.0315 per ounce, tin or pouch.[21] Excise taxes are also levied at the state level (Pennsylvania being the only exception), and in some instances, at the local level. Sales tax is also applied to the full retail price of dipping tobacco in most jurisdictions. The price of a tin of tobacco can range anywhere from under $1 per tin to more than $8. Price is affected by factors such as brand and especially the varying excise taxes from state to state.
See also
References
- ↑ "American Snuff Company - Est. 1900 - Timeline".
- ↑ Wolk, Robert; Shamsuzzaman, Abu S.M.; Svatikova, Anna; Huyber, Christine M.; Huck, Corey; Narkiewicz, Krzysztof; Somers, Virend K. (2005). "Hemodynamic and autonomic effects of smokeless tobacco in healthy young men". Journal of the American College of Cardiology. 45 (6): 910–4. PMID 15766828. doi:10.1016/j.jacc.2004.11.056. Lay summary – ScienceDaily (March 31, 2005).
- ↑ "Smokeless Tobacco – National Cancer Institute". Retrieved 19 June 2011.
- ↑ Rodu, Brad; Cole, Philip (2002). "Smokeless tobacco use and cancer of the upper respiratory tract". Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 93 (5): 511–5. PMID 12075196. doi:10.1067/moe.2002.123497.
- ↑ Bouquot, J.E; Meckstroth, R.L (1998). "Oral cancer in a tobacco-chewing US population—no apparent increased incidence or mortality". Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 86 (6): 697–706. PMID 9868728. doi:10.1016/S1079-2104(98)90207-4.
- ↑ Gupta, Ritesh; Gurm, Hitinder; Bartholomew, John R. (September 2004). "Smokeless Tobacco and Cardiovascular Risk". Archives of Internal Medicine. 164 (17): 1845–9. PMID 15451758. doi:10.1001/archinte.164.17.1845.
- ↑ Asplund, Kjell (2003). "Smokeless tobacco and cardiovascular disease". Progress in Cardiovascular Diseases. 45 (5): 383–94. PMID 12704595. doi:10.1053/pcad.2003.00102.
- ↑ Bolinder, Bolinder (1997). "Snusning en kontroversiell folkhälsofråga" [Overview of knowledge of health effects of smokeless tobacco. Increased risk of cardiovascular diseases and mortality because of snuff]. Läkartidningen (in Swedish). 94 (42): 3725–31. PMID 9411127.
- ↑ Siegel, D; Benowitz, N; Ernster, V L; Grady, D G; Hauck, W W (March 1992). "Smokeless tobacco, cardiovascular risk factors, and nicotine and cotinine levels in professional baseball players.". American Journal of Public Health. 82 (3): 417–21. PMC 1694380
 . PMID 1536359. doi:10.2105/AJPH.82.3.417.
. PMID 1536359. doi:10.2105/AJPH.82.3.417. - ↑ Gupta, BK; Kaushik, A; Panwar, RB; Chaddha, VS; Nayak, KC; Singh, VB; Gupta, R; Raja, S (January 2007). "Cardiovascular risk factors in tobacco-chewers: a controlled study". J Assoc Physicians India. 55: 27–31. PMID 17444341.
- ↑ Winn, D.M. (September 1997). "Epidemiology of Cancer and Other Systemic Effects Associated with the Use of Smokeless Tobacco". Advances in Dental Research. 11 (3): 313–21. PMID 9524431. doi:10.1177/08959374970110030201.
- ↑ Critchley, Julia A.; Unal, Belgin (April 2004). "Is smokeless tobacco a risk factor for coronary heart disease? A systematic review of epidemiological studies". European Journal of Cardiovascular Prevention & Rehabilitation. 11 (2): 101–12. PMID 15187813. doi:10.1097/01.hjr.0000114971.39211.d7.
- ↑ Bates, C; Fagerström, K; Jarvis, MJ; Kunze, M; McNeill, A; Ramström, L (December 2003). "European Union policy on smokeless tobacco: a statement in favour of evidence based regulation for public health". Tobacco Control. 12 (4): 360–7. PMC 1747769 . PMID 14660767. doi:10.1136/tc.12.4.360.
- ↑ UK's Action on Smoking & Health (ASH..) Archived 10 February 2006 at the Wayback Machine. Accessed on 31 July 2007.
- ↑ Centers for Disease Control and Prevention (1999). "Determination of Nicotine, pH, and Moisture Content of Six US Commercial Moist Snuff Products--Florida, January-February 1999". JAMA. 281 (24): 2279–80. PMID 10386544. doi:10.1001/jama.281.24.2279.
- ↑ http://www.doj.state.or.us/tobacco/pdf/smokeless_tobacco_directory.pdf%5B%5D
- ↑ Sachdev, Preeti; Chapman, Simon (September 2005). "Availability of smokeless tobacco products in South Asian grocery shops in Sydney, 2004". Medical Journal of Australia. 183 (6): 334. PMID 16167879.
- ↑ "British American Tobacco – EU Social Reporting – Issues". Batresponsibility.eu. Retrieved 2012-01-26.
- ↑ "The Family Smoking Prevention and Tobacco Control Act" (PDF).
- ↑ "Overview of the Family Smoking Prevention and Tobacco Control Act: Consumer Fact Sheet".
- ↑ "TTBGov Tax and Fee Rates". Ttb.gov. Retrieved 2012-01-26.
External links
- Smokeout: Not as easy as ABC - Commentary - The Washington Times, America's Newspaper
- Foulds, J; Ramstrom, L; Burke, M; Fagerström, K (2003). "Effect of smokeless tobacco (snus) on smoking and public health in Sweden". Tobacco Control. 12 (4): 349–59. JSTOR 20747648. PMC 1747791 . PMID 14660766. doi:10.1136/tc.12.4.349.
- Rodu, Brad; Godshall, William T (2006). "Tobacco harm reduction: an alternative cessation strategy for inveterate smokers". Harm Reduction Journal. 3: 37. PMC 1779270 . PMID 17184539. doi:10.1186/1477-7517-3-37.
- SnusOn Community - The world's largest forum community centered around Swedish snus and smokeless tobacco. Contains reviews, tutorials, information and discussions.
- Snus Authority - A blog dedicated to snus, snuff, and other forms of smokeless tobacco.
- Snus Central - A popular news and information site on smokeless tobacco.