Hyperthermic intraperitoneal chemotherapy
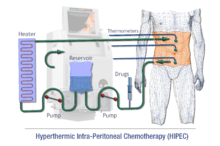
Intraperitoneal hyperthermic chemoperfusion (IPHC) is a type of hyperthermia therapy used in combination with surgery in the treatment of advanced abdominal cancers.[1] In this procedure, warmed anti-cancer drugs are infused and circulated in the peritoneal cavity (abdomen) for a short period of time. The chemotherapeutic agents generally infused during IPHC are mitomycin-C and cisplatin.
IPHC is also called hyperthermic intraperitoneal chemotherapy (HIPEC), intra-abdominal hyperthermic chemoperfusion, intraoperative chemohyperthermic peritoneal perfusion (CHPP), or the Sugarbaker technique, after Paul Sugarbaker, developer and advocate of this procedure.
History
In 1934, Joe Vincent Meigs in New York originally described tumor debulking surgery (cytoreductive surgery) for ovarian cancer under the premise of reducing macroscopic disease.[2] It took until the 1960-1970s for this aggressive cytoreductive approach to be widely accepted. During this time, Dr. Griffths at the National Cancer Institute also reported on prognostic indicators of survival in stage II and III ovarian cancer patients, importantly noting that residual tumor mass size (<1.6 cm) after cytoreductive surgery was significantly associated with extended survival.[2] During this time research started to show hyperthermia as well as intraperitoneal chemotherapy was effective in killing cancer cells. Spratt et al. in the 1980s, at the University of Louisville in Kentucky combined these concepts into a thermal transfusion infiltration system (TIFS) for delivery of heated chemotherapy into the peritoneal space of canines.[3] The first human was subjected to TIFS with administration of hyperthermic chemotherapy for locally advanced abdominal malignancy in 1979.[4] Further studies in the 1980s delivered chemotherapeutic agents at concentrations up to 30 times greater than those safely administered via IV route. In the mid to late 1980s, Dr. Sugarbaker spearheaded at the Washington Cancer Institute further investigation into therapy for gastrointestinal malignancies with peritoneal dissemination and was able to report survival benefits.[5] It became apparent early that completness of cytoreduction was associated with survival benefits.[2] So in 1995, Dr. Sugarbaker created a stepwise approach to cytoreduction, in an attempt to standardize and optimize this process.[6]
The HIPEC technique was also further improved upon by suggesting multiple modalities of delivery. The "Coliseum" technique as well as a similar approach described by Dr. Sugarbaker in 1999 were open abdominal techniques where heated chemotherapy was poured in. Benefits of this open approach included direct access by the surgeon to the cavity during administration of the hyperthermic agents to manipulate the fluid and bowel in order to achieve a quick and homogenous temperature and distribution of drug within the abdomen. Additionally, care can be taken to ensure that all peritoneal surfaces are exposed equally throughout the duration of the therapy as well as avoid dangerous temperatures or over-exposure to normal tissues. In comparison, the closed technique involves the closure of the abdominal wall prior to infusion of the chemotherapy reducing the issue of heat loss from peritoneal surfaces. In attempts to combine potential advantages of these two techniques, Dr. Sugarbaker employed a semi-open method by developing a new containment instrument (Thompson retractor) described in 2005 to support watertight elevation of the abdominal skin edges. More recently, a laparoscopic approach for CRS with HIPEC in highly selected patients with minimal disease burden has been described.
A further advance was made in 2016, when Lotti M. et al described a new technique, the Laparoscopy-Enhanced HIPEC (LE-HIPEC) technique, in which the hyperthermic chemotherapy is delivered after the closure of the abdominal wound, and a laparoscopic approach is used to stir the abdominal content during the perfusion[7][8]. Lotti M called into question the statement that the Coliseum technique could achieve the homogeneous distribution of heat[9]. The aim of the LE-HIPEC is to achieve a better heat delivery and preservation (as is in the closed technique) and a better circulation of the perfusion fluid (as is in the open technique)[10]. Compared to the standard closed-abdomen technique, the LE-HIPEC technique allows the surgeon to open the abdominal compartments to let the inflow of the heated perfusion fluid. Moreover, it allows the identification and division of the early intra-abdominal adhesions that can hamper the circulation of the perfusion fluid during a standard closed-abdomen perfusion. In a further study, Lotti M et al showed that after CRS early intra-abdominal adhesions occur in 70% of the patients, soon after the closure of the wound [11][12].
Use
IPHC is generally used after surgical removal of as much cancer as possible (debulking), which may include the removal of all involved peritoneal areas. These procedures can be 8–10 hours long and carry a significant rate of complications. IPHC is used as a viable solution for certain advanced stage tumors in the abdomen that have spread many small tumors throughout the abdomen, when surgery is not likely to be possible or effective. It can also be applied, during surgery, directly on the area, for those whose abdominal cancer is advanced but is still considered surgically resectable, as an alternative to surgery and traditional chemotherapy alone.[13]
The diseases most often treated with this method are cancer of the appendix, colorectal cancer, ovarian cancer, desmoplastic small round cell tumor and gastric cancer. It is also used for:
- mucinous adenocarcinoma (MAC) of appendix
- mesothelioma
- low-grade sarcoma
Chemotherapy Agents
Various chemotherapies are used[14] and there is no clear consensus on which drugs should be used. Mitomycin C is the most commonly used agent because it was one of the first used drugs for this therapy and less expensive than some of the alternatives. With the advent of platinum based chemotherapeutics, oxaliplatin has started gaining more popularity. Although both have proven similar efficacy so far, some argue that oxaliplatin tends to have better results.
- Mitomycin C[15]
- 30 mg in 3L for 60min + 10 mg for 40min
- Oxaliplatin[16]
- Given bidirectionally with 5-FU intravenously and oxalplatin in the peritoneum
- 460 mg/m2 for 30min at 42°-43 °C
- + I.V. 5-FU 400 mg/m2 & leucovorin 20 mg/m2
- Given bidirectionally with 5-FU intravenously and oxalplatin in the peritoneum
- Cisplatin
- Irinotecan
Procedure
The procedure is divided into three stages:
- Exploration: Here the surgeon will open the abdomen evaluate the peritoneal cancer.
- Debulking: In the debulking, or cytoreduction, phase of the procedure the surgeon will remove the visible tumor implants. However, even when all of the visible tumor is removed it is possible for microscopic cancer cells to still remain. The final stage of the procedure is meant to eliminate those cells.
- Chemoperfusion: Here the abdominal cavity is rinsed with a heated chemotherapy solution. Unlike systemic chemotherapy that is delivered in the blood stream, throughout the whole body, the chemotherapy in the HIPEC procedure is largely isolated in the peritoneal cavity. Therefore, a much higher concentration of chemotherapy can be utilized, while the toxicity and side-effects associated with systemic chemotherapy are minimized.
Controversy
CRS (cytoreduction) +HIPEC is associated with morbidity and some mortality. In patients with extensive disease in the peritoneum, organs need to be fully or partially resected as well. Skeptics of this procedure argue there is no multi-centered randomized Phase 3 trial comparing CRS+HIPEC with complete cytoreduction followed by systemic therapy. Hence this therapy has not met the scientific bar to be considered standard of care. However, proponents of CRS+HIPEC argue that until now, there has been no systemic therapy that has provided prolonged survival for peritoneal metastases. Peritoneal metastases, based on the primary tumor and extent of the disease, has a median overall survival of around 12 months on systemic therapy alone. Yet CRS+HIPEC has seen 5 year survival in the range of 20-40%.
References
- ↑ Esquivel, Jesus (2010). "Technology of Hyperthermic Intraperitoneal Chemotherapy in the United States, Europe, China, Japan and Korea". In Vincent T. DeVita Jr.; Theodore S. Lawrence; Steven A. Rosenberg. Cancer: Principles & Practice of Oncology—Annual Advances in Oncology, Volume 1. Lippincott Williams & Wilkins. pp. 188–193. ISBN 978-1-4511-0314-4.
- 1 2 3 Neuwirth, Madalyn G.; Alexander, H. Richard; Karakousis, Giorgos C. (2016-02-01). "Then and now: cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC), a historical perspective". Journal of Gastrointestinal Oncology. 7 (1): 18–28. ISSN 2078-6891. PMC 4754315
 . PMID 26941981. doi:10.3978/j.issn.2078-6891.2015.106.
. PMID 26941981. doi:10.3978/j.issn.2078-6891.2015.106. - ↑ Spratt, John S.; Adcock, Robert A.; Sherrill, William; Travathen, S. (1980-02-01). "Hyperthermic Peritoneal Perfusion System in Canines". Cancer Research. 40 (2). ISSN 0008-5472.
- ↑ Spratt, J. S.; Adcock, R. A.; Muskovin, M.; Sherrill, W.; McKeown, J. (1980-02-01). "Clinical delivery system for intraperitoneal hyperthermic chemotherapy". Cancer Research. 40 (2): 256–260. ISSN 0008-5472. PMID 6766084.
- ↑ Sugarbaker, P. H. (1988-01-01). "Surgical management of peritoneal carcinosis: diagnosis, prevention and treatment". Langenbecks Archiv Für Chirurgie. 373 (3): 189–196. ISSN 0023-8236. PMID 3288830. doi:10.1007/bf01274232.
- ↑ Sugarbaker, P. H. (1995-01-01). "Peritonectomy procedures". Annals of Surgery. 221 (1): 29–42. ISSN 0003-4932. PMC 1234492 . PMID 7826158. doi:10.1097/00000658-199501000-00004.
- ↑ Lotti, Marco; Capponi, Michela Giulii; Piazzalunga, Dario; Poiasina, Elia; Pisano, Michele; Manfredi, Roberto; Ansaloni, Luca (2016). "Laparoscopic HIPEC: A bridge between open and closed-techniques". Journal of Minimal Access Surgery. 12 (1): 86–89. ISSN 0972-9941. doi:10.4103/0972-9941.158965.
- ↑ Lotti, Marco (7 January 2016). "Laparoscopy-Enhanced Closed Abdomen Hyperthermic Intraperitoneal Chemotherapy". Journal of Laparoendoscopic & Advanced Surgical Techniques Part B, Videoscopy. doi:10.1089/vor.2015.0315.
- ↑ Lotti, Marco (15 June 2017). "A Coliseum with frail foundations: a critical analysis of the state-o…". slideshare.net.
- ↑ Lotti, Marco (18 September 2016). "the Laparoscopy-Enhanced HIPEC Concept". www.slideshare.net.
- ↑ Lotti, Marco; Giulii Capponi, Michela; Campanati, Luca; Poiasina, Elia; Ansaloni, Luca; Poletti, Eugenio; Frigerio, Luigi (December 2016). "The Onset of Intra-Abdominal Adhesions During Closed-Abdomen Hyperthermic Intraperitoneal Chemotherapy". Journal of Laparoendoscopic & Advanced Surgical Techniques. 26 (12): 997–1002. doi:10.1089/lap.2016.0396.
- ↑ Lotti, Marco (21 October 2016). "Intra-abdominal adhesions are formed during closed-abdomen HIPEC". www.youtube.com.
- ↑ http://healthnews.uc.edu/news/?/22745/
- ↑ Newton, Andrew D.; Bartlett, Edmund K.; Karakousis, Giorgos C. (2016-02-01). "Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: a review of factors contributing to morbidity and mortality". Journal of Gastrointestinal Oncology. 7 (1): 99–111. ISSN 2078-6891. PMC 4754303 . PMID 26941988. doi:10.3978/j.issn.2078-6891.2015.100.
- ↑ Franko, Jan; Ibrahim, Zuhaib; Gusani, Niraj J.; Holtzman, Matthew P.; Bartlett, David L.; Zeh, Herbert J. (2010-08-15). "Cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion versus systemic chemotherapy alone for colorectal peritoneal carcinomatosis". Cancer. 116 (16): 3756–3762. ISSN 1097-0142. doi:10.1002/cncr.25116.
- ↑ Klaver, Charlotte E L; Musters, Gijsbert D; Bemelman, Willem A; Punt, Cornelis J A; Verwaal, Victor J; Dijkgraaf, Marcel GW; Aalbers, Arend GJ; van der Bilt, Jarmila DW; Boerma, Djamila (2015-05-24). "Adjuvant hyperthermic intraperitoneal chemotherapy (HIPEC) in patients with colon cancer at high risk of peritoneal carcinomatosis; the COLOPEC randomized multicentre trial". BMC Cancer. 15. ISSN 1471-2407. PMC 4492087 . PMID 26003804. doi:10.1186/s12885-015-1430-7.
External links
- HIPEC Treatment Video Library A collection of videos featuring interviews with doctors who perform the HIPEC procedure and patients who have undergone it.
- HIPEC for peritoneal cancer patient information
- HIPEC, A Patient's Guide
- patient information on HIPEC