Intervertebral disc
| Intervertebral disc | |
|---|---|
 Intervertebral disc | |
| Details | |
| Identifiers | |
| Latin | Disci intervertebrales |
| MeSH | A02.165.308.410 |
| Dorlands /Elsevier | 12300697 |
| TA | A03.2.02.003 |
| FMA | 10446 |
An intervertebral disc (or intervertebral fibrocartilage) lies between adjacent vertebrae in the vertebral column. Each disc forms a fibrocartilaginous joint (a symphysis), to allow slight movement of the vertebrae, and acts as a ligament to hold the vertebrae together. Their role as shock absorbers in the spine is crucial.
Structure

Intervertebral discs consist of an outer fibrous ring, the annulus fibrosus disci intervertebralis, which surrounds an inner gel-like center, the nucleus pulposus. The anulus fibrosus consists of several layers (laminae) of fibrocartilage made up of both type I and type II collagen. Type I is concentrated towards the edge of the ring where it provides greater strength. The stiff laminae can withstand compressive forces. The fibrous intervertebral disc contains the nucleus pulposus and this helps to distribute pressure evenly across the disc. This prevents the development of stress concentrations which could cause damage to the underlying vertebrae or to their endplates. The nucleus pulposus contains loose fibers suspended in a mucoprotein gel. The nucleus of the disc acts as a shock absorber, absorbing the impact of the body's activities and keeping the two vertebrae separated. It is the remnant of the notochord.[1]
There is one disc between each pair of vertebrae, except for the first cervical segment, the atlas. The atlas is a ring around the roughly cone-shaped extension of the axis (second cervical segment). The axis acts as a post around which the atlas can rotate, allowing the neck to swivel. There are 23 discs in the human spine: 6 in the neck (cervical region), 12 in the middle back (thoracic region), and 5 in the lower back (lumbar region). For example, the disc between the fifth and sixth cervical vertebrae is designated "C5-6".
Development
During development and at birth, vertebral discs have some vascular supply to the cartilage endplates and the annulus fibrosus. These quickly deteriorate leaving almost no direct blood supply in healthy adults.[2]
Function
The intervertebral disc functions to separate the vertebrae from each other and provides the surface for the shock-absorbing gel of the nucleus pulposus. The nucleus pulposus of the disc functions to distribute hydraulic pressure in all directions within each intervertebral disc under compressive loads. The nucleus pulposus consists of large vacuolated notochord cells, small chondrocyte-like cells, collagen fibrils, and aggrecan, a proteoglycan that aggregates by binding to hyaluronan. Attached to each aggrecan molecule are glycosaminoglycan (GAG) chains of chondroitin sulfate and keratan sulfate.[3] Aggrecan is highly negatively charged, allowing the nucleus pulposus to swell by imbibing water. The amount of glycosaminoglycans (and hence water) decreases with age and degeneration.[4]
Clinical significance
Herniation
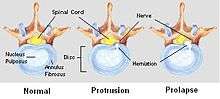
A spinal disc herniation, commonly referred to as a slipped disc, can happen when unbalanced mechanical pressures substantially deform the anulus fibrosus, allowing part of the nucleus to obtrude. These events can occur during peak physical performance, during traumas, or as a result of chronic deterioration, typically characterised by poor posture and has been associated with a Propionbacterium acnes infection.[5] Both the deformed anulus and the gel-like material of the nucleus pulposus can be forced laterally, or posteriorly, distorting local muscle function, and putting pressure on the nearby nerve. This can give the symptoms typical of nerve root entrapment. These symptoms can vary between parasthaesia, numbness, chronic and/or acute pain, either locally or along the dermatome served by the entrapped nerve, loss of muscle tone and decreased homeostatic performance . The disc is not physically slipped; it bulges, usually in just one direction. Risk of Cauda Equina.
Another kind of herniation, of the nucleus pulposus, can also happen as a result of the formation of Schmorl's nodes on the intervertebral disc.[6] This is referred to as vertical disc herniation.
Degeneration

Before age 40 approximately 25% of people show evidence of disc degeneration at one or more levels. Beyond age 40, more than 60% of people show evidence of disc degeneration at one or more levels on magnetic resonance imaging (MRI).[7] It is important to study clinically, as intervertebral discs degenerate sooner than any other connective tissue, often leading to back pain.[8]
One effect of ageing and disc degeneration is that the nucleus pulposus begins to dehydrate and the concentration of proteoglycans in the matrix decreases, thus limiting the ability of the disc to absorb shock. This general shrinking of disc size is partially responsible for the common decrease in height as humans age. The anulus fibrosus also becomes weaker with age and has an increased risk of tearing. In addition, the cartilage endplates begin thinning, fissures begin to form, and there is sclerosis of the subchondral bone.[2] As the fissures are formed in the anulus fibrosis due to osteo-arthritic bones or degeneration in general, the inner nucleus pulposus can seep out and put pressure on any number of vertebral nerves.[9] A herniated disc can cause mild to severe pain such as sciatica and treatment for herniated discs range from physical therapy to surgery. Other degeneration of the vertebral column includes diffuse idiopathic skeletal hyperostosis (DISH)[10] which is the calcification or ossification of the ligaments surrounding the vertebrae. This degeneration causes stiffness and sometimes even curvature in the lumbar and thoraco-lumbar spinal region.
Scoliosis
While this may not cause pain in some people, in others it may cause chronic pain. Other spinal disorders can affect the morphology of intervertebral discs. For example, patients with scoliosis commonly have calcium deposits (ectopic calcification) in the cartilage endplate and sometimes in the disc itself.[11] Herniated discs are also found to have a higher degree of cellular senescence than non-herniated discs.[2] In addition to scoliosis, which is the lateral 'S' curvature of the spine, the fused vertebrae can also experience other abnormalities such as kyphosis[9] (hunchback) which shows in old age, or lordosis[9] (swayback), which is often present in pregnancy and obesity.
Intervertebral disc space
The intervertebral disc space is typically defined on an X-ray photograph as the space between adjacent vertebrae. In healthy patients, this corresponds to the size of the intervertebral disc. The size of the space can be altered in pathological conditions such as discitis (infection of the intervertebral disc).[12]
Spelling note
Historically the word anulus was written (mistakenly) as annulus but has now been in use as anulus since it is derived from the Latin anus meaning ring.[13]
See also
Additional images
 Annulus fibrosus.
Annulus fibrosus. Artificial intervertebral disc.
Artificial intervertebral disc. Posterior longitudinal ligament, in the thoracic region.
Posterior longitudinal ligament, in the thoracic region. Median sagittal section through the occipital bone and first three cervical vertebrae.
Median sagittal section through the occipital bone and first three cervical vertebrae.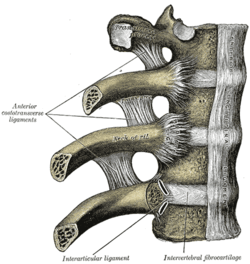 Costovertebral articulations. Anterior view.
Costovertebral articulations. Anterior view. Lumbar and sacral plexus. Deep dissection. Anterior view.
Lumbar and sacral plexus. Deep dissection. Anterior view. Lumbar and sacral plexus. Deep dissection. Anterior view.
Lumbar and sacral plexus. Deep dissection. Anterior view.
References
- ↑ McCann, Matthew; Owen J. Tamplin; Janet Rossant; Cheryle A. Séguin (25 October 2011). "Tracing notochord-derived cells using a Noto-cre mouse: implications for intervertebral disc development". Disease Models & Mechanisms. 5: 73. doi:10.1242/dmm.008128.
- 1 2 3 Roberts S, Evans H, Trivedi J, Menage J (April 2006). "Histology and pathology of the human intervertebral disc". J Bone Joint Surg Am. 88 (Suppl 2): 10–4. PMID 16595436. doi:10.2106/JBJS.F.00019.
- ↑ See Figure 1 in US patent application 2007/0003525.
- ↑ Antoniou, J.; Steffen, T.; Nelson, F.; Winterbottom, N.; Hollander, A. P.; Poole, R. A.; Aebi, M.; Alini, M. (1996). "The human lumbar intervertebral disc: Evidence for changes in the biosynthesis and denaturation of the extracellular matrix with growth, maturation, ageing, and degeneration". Journal of Clinical Investigation. 98 (4): 996–1003. PMC 507515
 . PMID 8770872. doi:10.1172/JCI118884.
. PMID 8770872. doi:10.1172/JCI118884. - ↑ Capoor, Manu N.; Ruzicka, Filip; Schmitz, Jonathan E.; James, Garth A.; Machackova, Tana; Jancalek, Radim; Smrcka, Martin; Lipina, Radim; Ahmed, Fahad S. (2017-04-03). "Propionibacterium acnes biofilm is present in intervertebral discs of patients undergoing microdiscectomy". PLOS ONE. 12 (4): e0174518. ISSN 1932-6203. PMC 5378350 . PMID 28369127. doi:10.1371/journal.pone.0174518.
- ↑ Williams, F. M. K.; Manek, N. J.; Sambrook, P. N.; Spector, T. D.; MacGregor, A. J. (2007). "Schmorl's nodes: Common, highly heritable, and related to lumbar disc disease". Arthritis & Rheumatism. 57 (5): 855. PMID 17530687. doi:10.1002/art.22789.
- ↑ "Intervertebral Disc Disorders". MDGuidelines. Reed Group. 1 December 2012.
- ↑ Urban, Jill PG; Roberts, Sally (1 January 2003). "Degeneration of the intervertebral disc". Arthritis Research & Therapy: 120–130. PMC 165040 . doi:10.1186/ar629.
- 1 2 3 "McGraw-Hill Connect". connect.mheducation.com. Retrieved 2015-11-29.
- ↑ Resnick, D (1978). "Diffuse idiopathic skeletal hyperostosis". American Journal of Roentgenology. 130 (3): 588–589. doi:10.2214/ajr.130.3.588.
- ↑ Giachelli CM (March 1999). "Ectopic calcification: gathering hard facts about soft tissue mineralization". Am. J. Pathol. 154 (3): 671–5. PMC 1866412 . PMID 10079244. doi:10.1016/S0002-9440(10)65313-8.
- ↑ "Endoscopic intervertebral disc surgery". Retrieved 2017-04-07.
- ↑ Federative Committee on Anatomical Terminology (FCAT) (1998). Terminologia Anatomica. Stuttgart: Thieme
External links
| Wikimedia Commons has media related to Intervertebral discs. |
- Intervertebral Discs
- Spinal Disc Summary
- Cross section image: pembody/body12a—Plastination Laboratory at the Medical University of Vienna
- From Occiput to Coccyx