High Frequency QRS
HFQRS (High Frequency QRS ) refers to the analysis of the high frequency spectral components of the QRS complex in an electrocardiogram (ECG).

The HFQRS has been extensively researched and clinically validated as an important diagnostic tool for detection of supply and demaned ischemia during the last decades.[1][2][3] Scientific evidences indicates that identification of depolarization abnormalities, which can be quantified using analysis of HFQRS, is more sensitive in detecting Myocardial Ischemia than identification according to ST segment deviations which present limited diagnostic accuracy, particularly in women.[4][5][6] On August 2013, the AHA included HFQRS in its scientific statement on exercise standards for testing, pointing out that it has been found to have useful test performance for detection of CAD [2]
Historic and Scientific Background
The diagnostic value of the HFQRS has been studied since the 1960's. The first studies correlate between incidence of notching and sluring in the QRS complexes to the existence and severity of coronary heart disease.[7] In 1979, a novel signal processing technique, including spatial filtering, averaging and alignment was used to show that HFQRS from patients in coronary care unit are less stable than in healthy subjects.[8] Later, Goldberger et al. identified reduction in the RMS (Root Mean Square) levels of the QRS (within frequency band of 80–300 Hz) in patients with Myocardial Infarction comparing to normal subjects.[9]
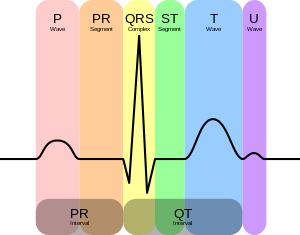
Significant research efforts during the 80-90s have shown that myocardial ischemia also induces changes to the depolarization phase and confirmed the use of HFQRS-RMS as a quantitative diagnostic measure of supply myocardial ischemia [1][10][11][12] and demand myocardial (stress-induced) ischemia.[5][13][14] These high frequency components, resulting from the fragmented waveform of electrical activation of the myocardium, can be filtered from high resolution ECG signals in the 150 to 250 Hz frequency band. Since these components are very low in amplitude (measured in µV), sophisticated computer analysis is required to reliably extract them. Yet, the conventional diagnosis of ischemia still relies upon recognition of abnormal alterations in the repolarization phase of the cardiac cycle, manifested as changes in the ST segment of the ECG.
Clinical Data
Several clinical studies showed that HFQRS is valuable in detecting supply ischemia[1] and stress induced ischemia (demand ischemia).[5][6][15] They also show that HFQRS performs significantly better than standard ST segment based analysis in detecting myocardial ischemia in stress ECG testing, both in terms of sensitivity and in specificity.[6][16] Another study even showed that HFQRS analysis performs equally well in women,[17] a population in which standard, ST segment based stress ECG analysis, is notoriously inaccurate.[18]
Economics of High Frequency QRS
Coronary artery disease (CAD) is a major healthcare problem worldwide, being the leading cause of death (more than 8 million deaths annually[19]) and imposing an enormous global economic burden.[20] In the US alone, there are 17.6 million CAD patients, and the estimated annual incidence of new and recurrent myocardial infarction is estimated to be 935,000. The estimated direct and indirect cost of CAD is $177 billion in 2010.[21] Accurate early diagnosis of CAD plays a crucial role in improving the prognosis of patients and in reducing the long-term costs of medical treatment. The current first line diagnostic test, standard stress ECG, lacks the desired accuracy and often leads to further testing. HFQRS may be significant for insurance companies, because it can potentially save thousands of dollars per patient by reducing the number of costly imaging procedures which also unnecessarily expose the patient to radiation.[22] Patients are sometimes referred even to invasive coronary angiography as a result of false positive stress ECG and imaging tests.
References
- 1 2 3 Abboud S., Cohen RJ., Selwyn A., Ganz P., Sadeh D., Friedman PL. Detection of transient myocardial ischemia by computer analysis of standard and signal-averaged high-frequency electrocardiograms in patients undergoing percutaneous transluminal coronary angioplasty.Circulation 1987;76(3):585–96.
- 1 2 Gerald F., Philip A., Kligfield P., et al. Exercise Standards for Testing and Training A Scientific Statement From the American Heart Association. Circulation. 2013; 128: 873-934.
- ↑ Abboud S., Berenfeld O., Sadeh D. Simulation of high-resolution QRS complex using a ventricular model with a fractal conduction system. Effects of ischemia on high-frequency QRS potentials Circ Res 1991;68 (6):1751-60.
- ↑ Gibbons RJ., Balady GJ., Bricker JT., et al. ACC/AHA 2002 guideline update for exercise testing: summary article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). J Am Coll Cardiol 2002; 40:1531-40.
- 1 2 3 Toledo E., Lipton JA., Warren SG., et al. Detection of stress-induced myocardial ischemia from the depolarization phase of the cardiac cycle - a preliminary study. J Electrocardiol 2009; 42:240-7.
- 1 2 3 Sharir T., Merzon, K., Kruchin I., Bojko A., Toledo E., Asman A., et al, Use of ECG depolarization abnormalities for detection of stress-induced ischemia as defined by myocardial perfusion imaging. Am J Cardiol. 2012;109:642–650.
- ↑ Langner PH., Geselowitz DB., Mansure FT., Lauer JA. High-frequency components in the electrocardiograms of normal subjects and of patients with coronary heart disease. Am Heart J 1961;62:746–55.
- ↑ Uijen GJ., de Weerd JP., Vendrik AJ. Accuracy of QRS detection in relation to the analysis of high-frequency components in the electrocardiogram. Med Biol Eng Comput 1979;17(4):492–502.
- ↑ Goldberger AL., Bhargava V., Froelicher V., Covell J. Effect of myocardial infarction on high-frequency QRS potentials. Circulation 1981;64(1):34–42.
- ↑ Mor-Avi V., Shargorodsky B., Abboud S., Laniado S., Akselrod S. Effects of coronary occlusion on high-frequency content of the epicardial electrogram and body surface electrocardiogram. Circulation 1987;76(1):237–43.
- ↑ Abboud S., Smith JM., Shargorodsky B., Laniado S., Sadeh D., Cohen RJ. High frequency electrocardiography of three orthogonal leads in dogs during a coronary artery occlusion. Pacing Clin Electrophysiol 1989;12(4 Pt 1):574–81.
- ↑ Abboud S. , Cohen RJ. , Sadeh D. A spectral analysis of the high frequency QRS potentials during acute myocardial ischemia in dogs. International Journal of Cardiology, 26: 285-290, 1990.
- ↑ Beker A., Pinchas A., Erel J., Abboud S. Spectral Analysis of High Resolution QRS Complex During Exercise Induce Ischemia. Annals of Noninvasive Electrocardiology, 1(4): 386-392, 1996.
- ↑ Lipton JA., Warren SG., Broce M., Abboud S., Beker A., Sornmo L., Lilly DR., Maynard CC., Lucas DB., Wagner GS. High frequency QRS electrocardiogram analysis during exercise stress testing for detecting ischemia. International Journal of Cardiology 124: 198–203, 2008
- ↑ Amit G., Galante O., Davrath LR., Luria O., Abboud S., Zahger D. High frequency QRS analysis in patients with acute myocardial infarction: a preliminary study. Ann Noninvasive Electrocardiol 2013;18 (2):149–56.
- ↑ Pettersson J., Pahlm O., Carro E., Edenbrandt L., Ringborn M., Sornmo L., et al. Changes in high-frequency QRS components are more sensitive than ST-segment deviation for detecting acute coronary artery occlusion. J Am Coll Cardiol 2000;36(6):1827–34.
- ↑ Rosenman D., Mogilevski Y., Amit G., Davrath LR., Tzivoni D. High frequency QRS analysis improves the specificity of exrecise ECG testing in women referred for angiography. J Electrocardiol 2013;46(1):19-26.
- ↑ Kohli P., Gulati M. Exercise Stress Testing in Women: Going Back to the Basics Circulation 2010;122:2570-2580
- ↑ GBD 2013 Mortality and Causes of Death, Collaborators (17 December 2014). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013.". Lancet 385: 117–171. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
- ↑ McKay J., Mensah GA. The Atlas of Heart Disease and Stroke. World Health Organization, 2004.
- ↑ Lloyd-Jones D., Adams RJ., Brown TM., et al. Heart disease and stroke statistics-2010 update: a report from the american heart association. Circulation 2010; 121:e46-e215.
- ↑ Amit G.,Toren Y., et al . The cost-effectiveness of stress testing using high-frequency QRS analysis. Int. J. Medical Engineering and Informatics; 2013 Vol.5, No.1
Links
- American Heart Association American Heart Association