Hemolytic-uremic syndrome
| Hemolytic-uremic syndrome | |
|---|---|
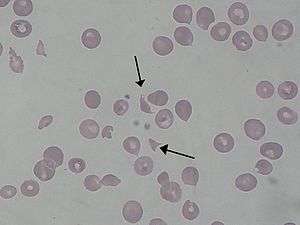 | |
| Schistocytes as seen in a person with hemolytic-uremic syndrome | |
| Classification and external resources | |
| Specialty | Nephrology |
| ICD-10 | D59.3 |
| ICD-9-CM | 283.11 |
| OMIM | 235400 |
| DiseasesDB | 13052 |
| MedlinePlus | 000510 |
| eMedicine | ped/960 |
| MeSH | D006463 |
Hemolytic-uremic syndrome (or haemolytic-uraemic syndrome), abbreviated HUS, is a disease characterized by a triad of hemolytic anemia (anemia caused by destruction of red blood cells), acute kidney failure (uremia), and a low platelet count (thrombocytopenia). It predominantly, but not exclusively, affects children. Most cases are preceded by an episode of infectious, sometimes bloody, diarrhea acquired as a foodborne illness or from a contaminated water supply caused by E. coli O157:H7, other non-o157:H7 E. coli serotypes, Shigella, and Campylobacter. A variety of viruses have also been implicated as a causative agent. It is now the most common cause of acquired acute renal failure in childhood. It is a medical emergency and carries a 5–10% mortality rate; of the remainder, the majority recover without major consequences, approximately 30% suffer residual renal injury. The primary target appears to be the vascular endothelial cell. This may explain the pathogenesis of HUS, in which a characteristic renal lesion is capillary microangiopathy.[1]
HUS was first defined as a syndrome in 1955.[2][3] The more common form of the disease, Shiga-like toxin-producing E. coli HUS (STEC-HUS), is triggered by the infectious agent E. coli O157:H7, and several other non-O157:H7 E. coli serotypes. Certain Shiga toxin-secreting strains of Shigella dysenteriae can also cause HUS.[4] Approximately 5% of cases are classified as pneumococcal HUS, which results from infection by Streptococcus pneumoniae, the agent that causes traditional lobar pneumonia.[5] There is also a rare, chronic, and severe form known as atypical hemolytic uremic syndrome (aHUS), which is caused by genetic defects resulting in chronic, uncontrolled complement activation.[6] Both STEC-HUS and aHUS cause endothelial damage, leukocyte activation, platelet activation, and widespread inflammation and multiple thromboses in the small blood vessels, a condition known as systemic thrombotic microangiopathy (TMA), which leads to thrombotic events as well as organ damage/failure and death.[7][8]
Signs and symptoms
STEC-HUS occurs after ingestion of a strain of bacteria expressing Shiga toxin(s), usually types of E. coli, that expresses verotoxin (also called Shiga-like toxin). E. coli can produce stx1 and/or stx2 Shiga toxins, the latter being more dangerous and a combination of both toxins in certain ratios is usually associated with HUS. These Shiga toxins bind GB3 receptors, globotriaosylceramide, which are present in renal tissue more than any other tissue and are also found in central nervous system neurons and other tissue. Children have more GB3 receptors than adults which may be why children are more susceptible to HUS. Cattle, swine, deer, and other mammals do not have GB3 receptors, but can be asymptomatic carriers of Shiga toxin-producing bacteria. Some humans can also be asymptomatic carriers. Once the bacteria colonizes, diarrhea followed by bloody diarrhea, hemorrhagic colitis, typically follows. HUS develops about 5–10 days after onset of diarrhea, with decreased urine output (oliguria), blood in the urine (hematuria), kidney failure, thrombocytopenia (low levels of platelets) and destruction of red blood cells (microangiopathic hemolytic anemia). Hypertension is common. In some cases, there are prominent neurologic changes.[9][10][11]
Patients with HUS commonly exhibit the signs and symptoms of thrombotic microangiopathy (TMA), which can include abdominal pain,[12] low platelet count,[13] elevated lactate dehydrogenase LDH, a chemical released from damaged cells, and which is therefore a marker of cellular damage)[14] decreased haptoglobin (indicative of the breakdown of red blood cells)[14] anemia (low red blood cell count)/schistocytes (damaged red blood cells),[13][14] elevated creatinine (a protein waste product generated by muscle metabolism and eliminated renally,[15] proteinuria (indicative of kidney injury),[16] confusion,[12] fatigue,[17] edema (swelling),[18] nausea/vomiting,[19] and diarrhea.[20] Additionally, patients with aHUS typically present with an abrupt onset of systemic signs and symptoms such as acute kidney failure,[13] hypertension (high blood pressure),[17] myocardial infarction (heart attack),[21] stroke,[12] lung complications,[21] pancreatitis (inflammation of the pancreas),[19] liver necrosis (death of liver cells or tissue),[13][17] encephalopathy (brain dysfunction),[17] seizure,[22] and coma.[23] Failure of neurologic, cardiac, renal, and gastrointestinal (GI) organs, as well as death, can occur unpredictably at any time, either very quickly or following prolonged symptomatic or asymptomatic disease progression.[6][7][13][16][24]
Atypical HUS
Atypical HUS (aHUS) represents 5–10% of HUS cases[6] and is largely due to one or several genetic mutations that cause chronic, uncontrolled, and excessive activation of complement.[6] This results in platelet activation endothelial cell damage, and white blood cell activation, leading to systemic TMA, which manifests as decreased platelet count, hemolysis (breakdown of red blood cells), damage to multiple organs, and ultimately death.[7][16][25] Early signs of systemic complement-mediated TMA include thrombocytopenia (platelet count below 150,000 or a decrease from baseline of at least 25%)[14] and evidence of microangiopathic hemolysis, which is characterized by elevated LDH levels, decreased haptoglobin, decreased hemoglobin (the oxygen-containing component of blood), and/or the presence of schistocytes.[7][8][14] Despite the use of supportive care, an estimated 33–40% of patients will die or have end-stage renal disease (ESRD) with the first clinical manifestation of aHUS,[20][21] and 65% of patients will die, require dialysis, or have permanent renal damage within the first year after diagnosis despite plasma exchange or plasma infusion (PE/PI) therapy.[20] Patients who survive the presenting signs and symptoms of aHUS endure a chronic thrombotic and inflammatory state, which puts them at lifelong elevated risk of sudden blood clotting, kidney failure, other severe complications and premature death.[8][18]
Historically, treatment options for aHUS were limited to plasma exchange or plasma infusion (PE/PI) therapy, which carries significant safety risks[26][27] and has not been proven effective in any controlled clinical trials. Patients with aHUS and ESRD have also had to undergo lifelong dialysis, which has a 5-year survival rate of 34–38%.[28][29] In recent years the monoclonal antibody eculizumab (INN and USAN, trade name Soliris), a first-in-class terminal complement inhibitor, has been shown in clinical studies to block terminal complement activity in children and adults with aHUS, and to eliminate the need for PE/PI and new dialysis. In these studies eculizumab was associated with reduced TMA activity, as shown by improvement in platelet counts and kidney function, as well as hematologic normalization, complete TMA response, and TMA event-free status in a majority of patients.[30]
Pathogenesis
HUS is one of the thrombotic microangiopathies, a category of disorders that includes STEC-HUS, aHUS, and thrombotic thrombocytopenic purpura (TTP). STEC-HUS is usually preceded by a prodrome of diarrhea, which is often bloody, and is caused by Shiga-like toxin-producing bacteria such as enterohemorrhagic Escherichia coli (EHEC), of which E. coli O157:H7 is the most common serotype.[31] Other serotypes also cause disease and can emerge as new causes of STEC-HUS, as occurred with E. coli O104:H4, which triggered a 2011 epidemic of STEC-HUS in Germany.[32]
The typical pathophysiology of HUS involves the binding of Shiga-toxin to the globotriaosylceramide (Gb3; also called ceramide trihexoside which accumulates in Fabry disease) receptor on the surface of the glomerular endothelium.[33] This action includes a cascade of signaling events leading to apoptosis and binding of leukocytes to endothelial cells. The Shiga-toxin-activated endothelial cells then become thrombogenic (clot-producing) by mechanism that is not fully understood,[34] though they have been shown to induce the release of cytokines and chemokines that are implicated in platelet activation.[35] Additionally, the binding action of Shiga-toxin inactivates a metalloproteinase called ADAMTS13, the deficiency of which causes the closely related TTP. Once ADAMTS13 is disabled, multimers of von Willebrand Factor (vWF) form and initiate platelet activation, causing microthrombus formation. The activation of platelets resulting from inhibition of ADAMTS13 is due to the hyperactivity of large multimers of uncleaved vWF. The arterioles and capillaries of the body become obstructed by the resulting complexes of activated platelets, which have adhered to the endothelium via large multimeric vWF. Through a mechanism known as microangiopathic hemolysis, the growing thrombi lodged in smaller vessels destroy red blood cells (RBCs) as they squeeze through the narrowed blood vessels, forming schistocytes, or fragments of sheared RBCs.[25] The presence of schistocytes is a key finding that helps to diagnose HUS. Typically, this hemolysis results in a hemoglobin level of less than 80 g/L.
Shiga-toxin directly activates the alternative complement pathway and also interferes with complement regulation by binding to complement factor H, an inhibitor of the complement cascade. Shiga-toxin causes complement-mediated platelet, leukocyte, and endothelial cell activation, resulting in systemic hemolysis, inflammation and thrombosis.[36][37][38] Severe clinical complications of TMA have been reported in patients from 2 weeks to more than 44 days after presentation with STEC-HUS, with improvements in clinical condition extending beyond this time frame, suggesting that complement activation persists beyond the acute clinical presentation and for at least 4 months.[39]
The consumption of platelets as they adhere to the thrombi lodged in the small vessels typically leads to mild or moderate thrombocytopenia with a platelet count of less than 60,000 per microliter.[40] As in the related condition TTP, reduced blood flow through the narrowed blood vessels of the microvasculature leads to reduced blood flow to vital organs, and ischemia may develop.[9] The kidneys and the central nervous system (brain and spinal cord) are the parts of the body most critically dependent on high blood flow, and are thus the most likely organs to be affected. However, in comparison to TTP, the kidneys tend to be more severely affected in HUS, and the central nervous system is less commonly affected.[41]
In contrast with typical disseminated intravascular coagulation seen with other causes of septicemia and occasionally with advanced cancer, coagulation factors are not consumed in HUS (or TTP) and the coagulation screen, fibrinogen level, and assays for fibrin degradation products such as "D-Dimers", are generally normal despite the low platelet count (thrombocytopenia).[41]
HUS occurs after 3–7% of all sporadic E. coli O157:H7 infections and up to approximately 20% or more of epidemic infections.[42] Children and adolescents are commonly affected.[43] Grossly, the kidneys may show patchy or diffuse renal cortical necrosis. Histologically, the glomeruli show thickened and sometimes split capillary walls due largely to endothelial swelling. Large deposits of fibrin-related materials in the capillary lumens, subendothelially, and in the mesangium are also found along with mesangiolysis. Interlobular and afferent arterioles show fibrinoid necrosis and intimal hyperplasia and are often occluded by thrombi.[10]
STEC-HUS most often affects infants and young children, but also occurs in adults. The most common form of transmission is ingestion of undercooked meat, unpasteurized fruits and juices, contaminated produce, contact with unchlorinated water, and person-to-person transmission in daycare or long-term care facilities.[23]
Unlike typical HUS, aHUS does not follow STEC infection and is thought to result from one or several genetic mutations that cause chronic, uncontrolled, and excessive activation of complement.[6] This leads to platelet activation, endothelial cell damage, and white blood cell activation, leading to systemic TMA, which manifests as decreased platelet count, hemolysis, damage to multiple organs, and ultimately, death.[7][16][25] Early signs of systemic complement-mediated TMA include thrombocytopenia (platelet count below 150,000 or a decrease from baseline of at least 25%)[14] and evidence of microangiopathic hemolysis, which is characterized by elevated LDH levels, decreased haptoglobin, decreased hemoglobin, and/or the presence of schistocytes.[7][8][14]
Diagnosis
The similarities between HUS, aHUS, and TTP make differential diagnosis essential.[7][8] All three of these systemic TMA-causing diseases are characterized by thrombocytopenia[14] and microangiopathic hemolysis,[6][14] plus one or more of the following: neurological symptoms (e.g., confusion,[6][22] cerebral convulsions,[22] seizures[19]); renal impairment[14] (e.g., elevated creatinine,[15] decreased estimated glomerular filtration rate [eGFR],[15] abnormal urinalysis[44]); and gastrointestinal (GI) symptoms (e.g., diarrhea,[17][20] nausea/vomiting,[19] abdominal pain,[19] gastroenteritis[14][17]).The presence of diarrhea does not exclude aHUS as the cause of TMA, as 28% of patients with aHUS present with diarrhea and/or gastroenteritis.[16][17] First diagnosis of aHUS is often made in the context of an initial, complement-triggering infection, and Shiga-toxin has also been implicated as a trigger that identifies patients with aHUS.[39] Additionally, in one study, mutations of genes encoding several complement regulatory proteins were detected in 8 of 36 (22%) patients diagnosed with STEC-HUS.[45] However, the absence of an identified complement regulatory gene mutation does not preclude aHUS as the cause of the TMA, as approximately 50% of patients with aHUS lack an identifiable mutation in complement regulatory genes.[17]
Diagnostic work-up supports the differential diagnosis of TMA-causing diseases. A positive Shiga-toxin/EHEC test confirms a cause for STEC-HUS,[23][31] and severe ADAMTS13 deficiency (i.e., ≤5% of normal ADAMTS13 levels) confirms a diagnosis of TTP.[46]
Treatment
The effect of antibiotics in E. coli O157:H7 colitis is controversial. Certain antibiotics may stimulate further verotoxin production and thereby increase the risk of HUS.[47][40][48] However, there is also tentative evidence that some antibiotics like quinolones may decrease the risk of hemolytic uremic syndrome.[48] In the 1990s a group of pediatricians from the University of Washington used a network of 47 cooperating laboratories in Washington, Oregon, Idaho, and Wyoming to prospectively identify 73 children younger than 10 years of age who had diarrhea caused by E. coli O157:H7 The hemolytic–uremic syndrome developed in 5 of the 9 children given antibiotics (56 percent), and in 5 of the 62 children who were not given antibiotics (8 percent, P<0.001).[49]
Treatment of HUS is generally supportive, with dialysis as needed. Platelet transfusion may actually worsen the outcome.
In most children with postdiarrheal HUS, there is a good chance of spontaneous resolution, so observation in a hospital is often all that is necessary, with supportive care such as hemodialysis where indicated. If a diagnosis of STEC-HUS is confirmed, plasmapheresis (plasma exchange) is contraindicated. However, plasmapheresis may be indicated when there is diagnostic uncertainty between HUS and TTP.
There are case reports of experimental treatments with eculizumab, a monoclonal antibody against CD5 that blocks part of the complement system, being used to treat congenital atypical hemolytic uremic syndrome,[50] as well as severe shiga-toxin associated hemolytic uremic syndrome.[51] These have shown promising results. Eculizeumab was approved by the U.S. Food and Drug Administration (FDA) on March 13, 2007 for the treatment of paroxysmal nocturnal hemoglobinuria (PNH), a rare, progressive, and sometimes life-threatening disease characterized by excessive hemolysis; and on September 23, 2011 for the treatment of atypical hemolytic uremic syndrome (aHUS) It was approved by the European Medicines Agency for the treatment of PNH on June 20, 2007, and on November 29, 2011 for the treatment of aHUS. However, of note is the exceedingly high cost of treatment, with one year of the drug costing over $500,000.
Scientists are trying to understand how useful it would be to immunize humans or cattles with vaccines.[52]
Prognosis
Acute renal failure occurs in 55–70% of patients with STEC-HUS, although up to 70–85% recover renal function.[53] Patients with aHUS generally have poor outcomes, with up to 50% progressing to ESRD or irreversible brain damage; as many as 25% die during the acute phase.[53] However, with aggressive treatment, more than 90% of patients survive the acute phase of HUS, and only about 9% may develop ESRD. Roughly one-third of persons with HUS have abnormal kidney function many years later, and a few require long-term dialysis. Another 8% of persons with HUS have other lifelong complications, such as high blood pressure, seizures, blindness, paralysis, and the effects of having part of their colon removed. The overall mortality rate from HUS is 5–15%. Children and the elderly have a worse prognosis.[54]
Epidemiology
The country with the highest incidence of HUS is Argentina[55][56][57][58] and it performs a key role in the research of this condition.
In the United States, the overall incidence of HUS is estimated at 2.1 cases per 100,000 persons/year, with a peak incidence between six months and four years of age.[1]
HUS and the E. coli infections that cause it have been the source of much negative publicity for the FDA, meat industries, and fast-food restaurants since the 1990s, especially in the contaminations linked to Jack in the Box restaurants. The disease was also featured in the Robin Cook novel Toxin. In 2006, an epidemic of harmful E. coli emerged in the United States due to contaminated spinach. In June, 2009, Nestle Toll House cookie dough was linked to an outbreak of E. coli O157:H7 in the United States, which sickened 70 people in 30 states.[1]
In May, 2011 an epidemic of bloody diarrhea caused by E. coli O104:H4-contaminated fenugreek seeds hit Germany. Tracing the epidemic revealed more than 3,800 cases, with HUS developing in more than 800 of the cases, including 36 fatal cases. Nearly 90% of the HUS cases were in adults.[59][60] In response to the crisis, Alexion Pharmaceuticals, Inc., the makers of Soliris (eculizumab), initiated of an open-label clinical trial to investigate eculizumab as a treatment for patients with Shiga-toxin-producing E. coli hemolytic uremic syndrome (STEC-HUS). Alexion also initiated an eculizumab access program whereby the company provided eculizumab free of charge throughout the crisis. The study was designed to include all patients treated with eculizumab during the 2011 STEC-HUS outbreak.[61]
See also
References
- 1 2 3 Corrigan JJ, Boineau FG (November 2001). "Hemolytic-uremic syndrome". Pediatr Rev. 22 (11): 365–9. PMID 11691946.
- ↑ Anagnou NP, Papanicolaou N, Fessas P (1991). "Recurrent attacks of hemolytic uremic syndrome". Haematologia (Budap). 24 (2): 101–5. PMID 1816053.
- ↑ Gasser C, Gautier E, Steck A, Siebenmann RE, Oechslin R (September 1955). "Hemolytic-uremic syndrome: bilateral necrosis of the renal cortex in acute acquired hemolytic anemia". Schweiz Med Wochenschr (in German). 85 (38–39): 905–9. PMID 13274004.
- ↑ Robbins and Cotran pathologic basis of disease. (2010) (8th ed.). Philadelphia, PA: Saunders/Elsevier.
- ↑ Shimizu, M; Yokoyama, T; Sakashita, N; Sato, A; Ueno, K; Akita, C; Ohta, K; Kitano, E; Hatanaka, M; Kitamura, H; Saikawa, Y; Yachie, A (October 2012). "Thomsen-Friedenreich antigen exposure as a cause of Streptococcus pyogenes-associated hemolytic-uremic syndrome". Clinical nephrology. 78 (4): 328–31. PMID 22981036. doi:10.5414/CN107205.
- 1 2 3 4 5 6 7 Noris, M; Remuzzi, G (2009). "Atypical hemolytic-uremic syndrome". N Engl J Med. 361 (17): 1676–1687. PMID 19846853. doi:10.1056/NEJMra0902814.
- 1 2 3 4 5 6 7 Benz, K; Amann, K (2010). "Thrombotic microangiopathy: new insights". Current Opinion in Nephrology and Hypertension. 19 (3): 242–247. PMID 20186056. doi:10.1097/MNH.0b013e3283378f25.
- 1 2 3 4 5 Zipfel, PF; Heinen, S; Skerka, C (2010). "Thrombotic microangiopathies: new insights and new challenges". Current Opinion in Nephrology and Hypertension. 19 (4): 372–378. PMID 20539230. doi:10.1097/MNH.0b013e32833aff4a.
- 1 2 Boyer, O; Niaudet, P (August 2011). "Hemolytic Uremic Syndrome: New Developments in Pathogenesis and Treatments". Int J Nephrol. 2011: 908407. PMC 3159990
 . PMID 21876803. doi:10.4061/2011/908407.
. PMID 21876803. doi:10.4061/2011/908407. - 1 2 Kumar, V; Cotran, RS; Robbins, SL, eds. (2002). Robbins Basic Pathology. Philadelphia, PA: Saunders. ISBN 0721692745.
- ↑ Nathanson, S.; Kwon, T.; Elmaleh, M.; et al. (2010). "Acute neurological involvement in diarrhea-associated hemolytic uremic syndrome". Clin J Am Soc Nephrol. 5 (7): 1218–1228. PMC 2893076 . PMID 20498239. doi:10.2215/CJN.08921209.
- 1 2 3 Ohanian, M; Cable, C; Halka, K (2011). "Eculizumab safely reverses neurologic impairment and eliminates the need for dialysis in severe atypical hemolytic uremic syndrome". Clin Pharmacol. 3: 5–12. PMC 3262387 . PMID 22287852. doi:10.2147/CPAA.S17904.
- 1 2 3 4 5 Loirat, C; Noris, M; Fremaux-Bacchi, V (2008). "Complement and the atypical hemolytic uremia syndrome in children". Pediatr Nephrol. 23 (11): 1957–1972. PMID 18594873. doi:10.1007/s00467-008-0872-4.
- 1 2 3 4 5 6 7 8 9 10 11 Caprioli, J.; Noris, M.; Brioschi, S.; et al. (2006). "Genetics of HUS: the impact of MCP, CFH, and IF mutations on clinical presentation, response to treatment, and outcome". Blood. 108 (4): 1267–1279. PMC 1895874 . PMID 16621965. doi:10.1182/blood-2005-10-007252.
- 1 2 3 Ariceta, Gema; Besbas, Nesrin; Johnson, Sally; et al. (2009). "Guideline for the investigation and initial therapy of diarrhea-negative hemolytic uremic syndrome". Pediatr Nephrol. 24 (4): 687–696. PMID 18800230. doi:10.1007/s00467-008-0964-1.
- 1 2 3 4 5 Sellier-Leclers, A.-L.; Fremeaux-Bacchi, V.; Dragon-Durey, M.-A.; et al. (2007). "Differential impact of complement mutations on clinical characteristics in atypical hemolytic uremic syndrome". J Am Soc Nephrol. 18 (8): 2392–2400. PMID 17599974. doi:10.1681/ASN.2006080811.
- 1 2 3 4 5 6 7 8 Noris, M.; Caprioli, J.; Bresin, E.; et al. (2010). "Relative role of genetic complement abnormalities in infrequent and familial aHUS and their impact on clinical phemotype". Clin J Am Soc Nephrol. 5 (10): 1844–1859. PMC 2974386 . PMID 20595690. doi:10.2215/CJN.02210310.
- 1 2 Ståhl, A.-L.; Vazir-Sani, F.; Heinen, S.; et al. (2008). "Factor H dysfunction in patients with atypical hemolytic uremic syndrome contributes to complement deposition on platelets and their activation". Blood. 111 (11): 5307–5317. PMID 18268093. doi:10.1182/blood-2007-08-106153.
- 1 2 3 4 5 Dragon-Durey, M.-A.; Sethi, S. K.; Bagga, A.; et al. (2010). "Clinical features of anti-factor H autoantibody-associated hemolytic uremic syndrome". J Am Soc Nephrol. 21 (12): 2180–2187. PMC 3014031 . PMID 21051740. doi:10.1681/ASN.2010030315.
- 1 2 3 4 Zuber, J; Le Quintrec, M; Sberro-Scussan, R; Loirat, C; Fremaux-Bacchi, V; Legendre, C (2011). "New insights into postrenal transplant hemolytic uremic syndrome". Nature Reviews Nephrology. 7 (1): 23–35. PMID 21102542. doi:10.1038/nrneph.2010.155.
- 1 2 3 Sallee, M; et al. (2010). "Myocardial infarction is a complication of factor H-associated atypical HUS". Nephrol Dial Transplant. 25 (6): 2028–2032. PMID 20305136. doi:10.1093/ndt/gfq160.
- 1 2 3 Neuhaus, TJ; Calonder, S; Leumann, EP (1997). "Heterogeneity of atypical haemolytic uraemis syndromes". Arch Dis Child. 76 (6): 518–521. PMC 1717216 . PMID 9245850. doi:10.1136/adc.76.6.518.
- 1 2 3 Noris, M; Remuzzi, G (2005). "Hemolytic uremic syndrome". J Am Soc Nephrol. 16 (4): 1035–1050. PMID 15728781. doi:10.1681/ASN.2004100861.
- ↑ Mache, CJ; et al. (2009). "Complement inhibitor eculizumab in atypical hemolytic uremic syndrome". Clin J Amer Soc Nephrol. 4 (8): 1312–1316. doi:10.2215/CJN.01090209.
- 1 2 3 Tsai, H-M (2010). "Pathophysiology of thrombotic thrombocytopenic purpura". Int J Hematol. 91 (1): 1–19. PMC 3159000 . PMID 20058209. doi:10.1007/s12185-009-0476-1.
- ↑ George, JN (2010). "How I treat my patients with thrombotic thrombocytopenic purpura". Blood. 116 (20): 4060–4069. PMID 20686117. doi:10.1182/blood-2010-07-271445.
- ↑ Michon, B; et al. (2007). "Complications of apheresis in children". Transfusion. 47 (10): 1837–1842. PMID 17880609. doi:10.1111/j.1537-2995.2007.01405.x.
- ↑ Collins, Allan J.; et al. (2010). "Excerpts from the US Renal Data System 2009 Annual Data Report". Am J Kidney Dis. 55: S1–S7. doi:10.1053/j.ajkd.2009.10.009.
- ↑ European Renal Association- European Dialysis and Transplant Association Registry (2011). ERA-EDTA Registry Annual Report 2009. Amsterdam, The Netherlands: Academic Medical Center Department of Medical Informatics.
- ↑ "Soliris (eculizumab) prescribing information" (PDF). Cheshire, CT: Alexion Pharmaceuticals. 2011.
- 1 2 Palermo, MS; Exeni, RA; Fernandez, GC (2009). "Hemolytic Uremic Syndrome: pathogenesis and update of interventions". Expert Rev Anti Infect Ther. 7 (6): 697–707. PMID 19681698. doi:10.1586/eri.09.49.
- ↑ Robert Koch Institute. "Technical Report: EHEC/HUS O104:H4 Outbreak, Germany, May/June 2011" (PDF). Berlin, Germany: Robert Koch Institute.
- ↑ Psotka, MA; et al. (2009). "Shiga toxin 2 targets the murine renal collecting duct epithelium". Infect Immun. 77 (3): 959–969. PMC 2643625 . PMID 19124603. doi:10.1128/IAI.00679-08.
- ↑ Zoja, C; Buelli, S; Morigi, M (2010). "Shoga toxin-associated hemolytic uremic syndrome: pathophysiology of endothelial dysfunction". Pediatr Nephrol. 25 (11): 2231–2240. PMID 20424866. doi:10.1007/s00467-010-1522-1.
- ↑ Guessous, F; et al. (2005). "Shiga toxin 2 and lipopolysaccharide induce human microvascular endothelial cells to release chemokines and factor that stimulate platelet function". Infect Immun. 73 (12): 8306–8316. PMC 1307066 . PMID 16299328. doi:10.1128/IAI.73.12.8306-8316.2005.
- ↑ Orth, D; Würzner, R (2010). "Complement in typical hemolytic uremic syndrome". Semin thromb Hemost. 36 (3): 620–624. doi:10.1055/s-0030-1262883.
- ↑ Stahl, AL; Startz, L; Karpman, D (2011). "Complement activation on platelet-leukocyte complexes and microparticles in enterohemorrhagic Escherichia coli-induced hemolytic uremic syndrome". Blood. 117 (20): 5503–5513. PMID 21447825. doi:10.1182/blood-2010-09-309161.
- ↑ Thurman, J.M.; et al. (2009). "Alternative pathway of complement in children with diarrhea-associated hemolytic uremic syndrome". Clin J Am Soc Nephrol. 4 (12): 1920–1924. PMC 2798880 . PMID 19820137. doi:10.2215/CJN.02730409.
- 1 2 Mache, C; et al. (June 2010). "Eculizumab in diarrhea-associated hemolytic uremic syndrome". Presented at the 2nd International Conference on HUS-MPGN-PNH. Innsbruck, Austria.
- 1 2 Tan, AJ. "Hemolytic uremic syndrome in emergency medicine". Medscape eMedicine.
- 1 2 Kanso, AA; Abou Hassan, NM; Badr, KF (2008). "Micro and macrovascular disease of the kidney". In: Brenner BM, ed. the Kidney, 8th edition. Philadelphia, PA: Saunders Elsevier: chapter 32.
- ↑ Mead, PS; Griffin, PM (1998). "Escherichia coli O157:H7". Lancet. 352 (9135): 1207–1212. PMID 9777854. doi:10.1016/S0140-6736(98)01267-7.
- ↑ Ruggenenti, P; Noris, M; Remuzzi, G (2001). "Thrombotic microangiopathy, hemolytic uremic syndrome, and thrombotic thrombocytopenic purpura". Kidney Int. 60 (3): 831–846. PMID 11532079. doi:10.1046/j.1523-1755.2001.060003831.x.
- ↑ Al-Akash, AI; Almond, PS; Savell, VH Jr; Gharaybeth, SI; Hogue, C (2011). "Eculizumab includes long-term remission in recurrent post-transpant HUS associated with C3 gene mutation". Pediatr Nephrol. 26 (4): 613–619. PMID 21125405. doi:10.1007/s00467-010-1708-6.
- ↑ Gangnadoux, MF; Habib, R; Gubler, MC; Bacri, JL; Broyer, M (1996). "Long-term (15-25 years) outcome of childhood hemolytic-uremic syndrome". Clin Nephrol. 46 (1): 39–41. PMID 8832149.
- ↑ Zhen,, XL; et al. (2010). "Multiple domains of ADAMTS13 are targeted by autoantibodies against ADAMTS13 in patients with acquired idiopathic thrombotic thrombocytopenic purpura". Haematologica. 95 (9): 1555–1562. PMC 2930958 . PMID 20378566. doi:10.3324/haematol.2009.019299.
- ↑ Goldwater, P N; Bettelheim, K A (2012). "Treatment of enterohemorrhagic Escherichia coli (EHEC) infection and hemolytic uremic syndrome (HUS)". BMC medicine. 10 (12).
- 1 2 Panos GZ, Betsi GI, Falagas ME (September 2006). "Systematic review: are antibiotics detrimental or beneficial for the treatment of patients with Escherichia coli O157:H7 infection?". Aliment. Pharmacol. Ther. 24 (5): 731–42. PMID 16918877. doi:10.1111/j.1365-2036.2006.03036.x.
- ↑ N Eng J Med 2000: 342:1930-1936 June 29, 2000. The risk of Hemolytic Uremic syndrome after antibiotic treatment of escherichia coli O157:H7 infections. Craig S. Wong, M.D., Srdjan Jelacic, B.S., Rebecca L. Habeeb, B.S., Sandra L. Watkins, M.D., and Phillip I. Tarr, M.D. N Engl J Med 2000; 342:1930-1936 June 29, 2000
- ↑ Gruppo RA, Rother RP (2009). "Eculizumab for congenital atypical hemolytic-uremic syndrome". N Engl J Med. 360 (5): 544–546. doi:10.1056/NEJMc0809959.
- ↑ Lapeyraque, A-L; et al. (2011). "Eculizumab in Severe Shiga-Toxin–Associated HUS". N Engl J Med. 364 (26): 2561–2563. PMID 21612462. doi:10.1056/NEJMc1100859.
- ↑ O'Ryan, M; Vidal, R; Del Canto, F; Salazar, J C; Montero, D (2015). "Vaccines for viral and bacterial pathogens causing acute gastroenteritis: Part II: Vaccines for Shigella, Salmonella, enterotoxigenic E. coli (ETEC) enterohemorragic E. coli (EHEC) and Campylobacter jejuni". Human Vaccines & Immunotherapeutics. 11 (3): 601–619.
- 1 2 Parmar, MS (2010). "Hemolytic-uremic syndrome". Medscape eMedicine.
- ↑ Chu, P; Hemphill, RR (2004). "222: Acquired hemolytic anemia". Emergency Medicine: A Comprehensive Study Guide (6th ed.). New York, NY: McGraw-Hill. ISBN 0-07-138875-3.
- ↑ Rivero, MA; Passucci, JA; Rodriguez, EM; Signorini, ML; Tarabla, HD; Parma, AE (2011). "Factors associated with sporadic verotoxigenic Escherichia coli infection in children with diarrhea from the Central Eastern Area of Argentina". Foodborne pathogens and disease. 8 (8): 901–6. PMID 21492023. doi:10.1089/fpd.2010.0800.
- ↑ Rivas, M; Caletti, MG; Chinen, I; Refi, SM; Roldán, CD; Chillemi, G; Fiorilli, G; Bertolotti, A; Aguerre, L; Sosa Estani, S (2003). "Home-prepared hamburger and sporadic hemolytic uremic syndrome, Argentina". Emerging Infectious Diseases. 9 (9): 1184–6. PMC 3016759 . PMID 14531383. doi:10.3201/eid0909.020563.
- ↑ Rivero, MA; Padola, NL; Etcheverría, AI; Parma, AE (2004). "Enterohemorrhagic Escherichia coli and hemolytic-uremic syndrome in Argentina". Medicina. 64 (4): 352–6. PMID 15338982.
- ↑ "What is HUS?" (PDF).
- ↑ Buchholz, U; et al. (2011). "German outbreak of escherichia coli O104:H4 associated with sprouts". N Engl J Med. 365 (19): 1763–1770. PMID 22029753. doi:10.1056/NEJMoa1106482.
- ↑ Frank, C; et al. (2011). "Epidemic profile of Shiga-toxin-producing Escherichia coli O104:H4 outbreak in Germany". N Engl J Med. 365 (19): 1711–1780. PMID 21696328. doi:10.1056/NEJMoa1106483.
- ↑ Alexion Pharmaceuticals Inc. (June 20, 2011). "Alexion initiates clinical trial of eculizumab as a potential treatment for patients with STEC-HUS in expanded response to EHEC crisis in Germany (press release)". Cheshire, CT.
External links
- GeneReviews/NCBI/NIH/UW entry on Atypical hemolytic-uremic syndrome
- Haemolytic Uraemic Syndrome Help (UK Based Charity for Information and Support)
- aHUS UK – A Patients and Families Support Group for atypical Haemolytic Uraemic Syndrome
- Atypical HUS and Complement Deficiencies - Clinical Immunology