Complete blood count
| Complete blood count | |
|---|---|
| Medical diagnostics | |
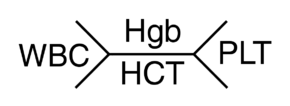 Schematics (also called "Fishbones") of shorthand for complete blood count commonly used by clinicians. The shorthand on the right is used more often in the US. Hgb=Hemoglobin, WBC=White blood cells, Plt=Platelets, Hct=Hematocrit. | |
| Reference range |
|
| MeSH | D001772 |
| MedlinePlus | 003642 |
| eMedicine | 94020 |
| LOINC | Codes for CBC, e.g., 57021-8 |
| HCPCS-L2 | G0306 |
A complete blood count (CBC), also known as a complete blood cell count, full blood count (FBC), or full blood exam (FBE), is a blood panel requested by a doctor or other medical professional that gives information about the cells in a patient's blood, such as the cell count for each cell type and the concentrations of various proteins and minerals. A scientist or lab technician performs the requested testing and provides the requesting medical professional with the results of the CBC.
Blood counts of various types have been used for clinical purposes since the 19th century. Automated equipment to carry out complete blood counts was developed in the 1950s and 1960s.[1]
The cells that circulate in the bloodstream are generally divided into three types: white blood cells (leukocytes), red blood cells (erythrocytes), and platelets (thrombocytes). Abnormally high or low counts may indicate the presence of many forms of disease, and hence blood counts are among the most commonly performed blood tests in medicine, as they can provide an overview of a patient's general health status. A CBC is routinely performed during annual physical examinations in some jurisdictions.
Medical uses
Complete blood counts are done to monitor overall health, to screen for some diseases, to confirm a diagnosis of some medical conditions, to monitor a medical condition, and to monitor changes in the body caused by medical treatments.[2]
For patients who need blood transfusion, a blood count may be used to get data which would help plan an amount of treatment.[3] In such cases, the person should have only one blood count for the day, and the transfusion of red blood cells or platelets should be planned based on that.[3] Multiple blood draws and counts throughout the day are an excessive use of phlebotomy and can lead to unnecessary additional transfusions, and the extra unnecessary treatment would be outside of medical guidelines.[3]
Procedure
A phlebotomist collects the sample through venipuncture, drawing the blood into a test tube containing an anticoagulant (EDTA, sometimes citrate) to stop it from clotting. The sample is then transported to a laboratory. Sometimes the sample is drawn off a finger prick using a Pasteur pipette for immediate processing by an automated counter.
In the past, counting the cells in a patient's blood was performed manually, by viewing a slide prepared with a sample of the patient's blood (a blood film, or peripheral smear) under a microscope. However, manual cell counts are becoming less common, and instead this process is generally automated by use of an automated analyzer. As few as 10–20% of samples are now examined manually.
Automated

Most blood counts today include a CBC count and leukocyte differential count (LDC) (that is, not just the total WBC count but also the broken down percentage of each WBC type, such as neutrophils, eosinophils, basophils, monocytes, and lymphocytes). More sophisticated modern analyzers can provide extended differential counts, which include hematopoietic progenitor cells, immature granulocytes, and erythroblasts.[4]
The blood is well mixed (though not shaken) and placed on a rack in the analyzer. This instrument has flow cells, photometers and apertures that analyze different elements in the blood. The cell counting component counts the numbers and types of different cells within the blood. The results are printed out or sent to a computer for review.
Blood counting machines aspirate a very small amount of the specimen through narrow tubing followed by an aperture and a laser flow cell. Laser eye sensors count the number of cells passing through the aperture, and can identify them; this is flow cytometry. The two main sensors used are light detectors and electrical impedance. The instrument measures the type of blood cell by analyzing data about the size and aspects of light as they pass through the cells (called front and side scatter). Other instruments measure different characteristics of the cells to categorize them.
Because an automated cell counter samples and counts so many cells, the results are very precise. However, certain abnormal cells in the blood may not be identified correctly, requiring manual review of the instrument's results and identification of any abnormal cells the instrument could not categorize.
In addition to counting, measuring and analyzing red blood cells, white blood cells and platelets, automated hematology analyzers also measure the amount of hemoglobin in the blood and within each red blood cell. This is done by adding a diluent that lyses the cells which is then pumped into a spectro-photometric measuring cuvette. The change in color of the lysate equates to the hemoglobin content of the blood. This information can be very helpful to a physician who, for example, is trying to identify the cause of a patient's anemia. If the red cells are smaller or larger than normal, or if there is a lot of variation in the size of the red cells, this data can help guide the direction of further testing and expedite the diagnostic process so patients can get the treatment they need quickly.
Manual


Hemocytometers (counting chambers that hold a specified volume of diluted blood and divide it with grid lines) are used to calculate the number of red and white cells per litre of blood. (The dilution and grid lines are needed because there are far too many cells without those aids.)
To identify the numbers of different white cells, a blood film is made, and a large number of white blood cells (at least 100) are counted. This gives the percentage of cells that are of each type. By multiplying the percentage with the total number of white blood cells, the absolute number of each type of white cell can be obtained.
Manual counting is useful in cases where automated analyzers cannot reliably count abnormal cells, such as those cells that are not present in normal patients and are only seen in peripheral blood with certain haematological conditions. Manual counting is subject to sampling error because so few cells are counted compared with automated analysis. A manual count will also give information about other cells that are not normally present in peripheral blood, but may be released in certain disease processes.
Medical technologists examine blood film via a microscope for some CBCs, not only to find abnormal white cells, but also because variation in the shape of red cells is an important diagnostic tool. Although automated analysers give fast, reliable results regarding the number, average size, and variation in size of red blood cells, they do not detect cells' shapes. Also, some normal patients' platelets will clump in EDTA anticoagulated blood, which causes automatic analyses to give a falsely low platelet count. The person viewing the slide in these cases will see clumps of platelets and can estimate if there are low, normal, or high numbers of platelets.
Included tests

A complete blood count will normally include:
White cells
Total white blood cells are reported, and a differential reports all the white cell types as a percentage and as an absolute number per unit volume.[5] A high WBC may indicate an infection.
Neutrophils: May indicate bacterial infection. May also be raised in acute viral infections. Because of the segmented appearance of the nucleus, neutrophils are sometimes referred to as "segs". The nucleus of less mature neutrophils is not segmented, but has a band or rod-like shape. Less mature neutrophils—those that have recently been released from the bone marrow into the bloodstream—are known as "bands" or "stabs". Stab is a German term for rod.[6]
Lymphocytes: Higher with some viral infections such as glandular fever. Raised in chronic lymphocytic leukemia (CLL). Can be decreased by HIV infection. In adults, lymphocytes are the second most common WBC type after neutrophils. In young children under age 8, lymphocytes are more common than neutrophils.[6]
Monocytes: May be raised in bacterial infection, tuberculosis, malaria, Rocky Mountain spotted fever, monocytic leukemia, chronic ulcerative colitis and regional enteritis[6]
Eosinophils: Increased in parasitic infections, asthma, or allergic reaction.
Basophils: May be increased in bone marrow related conditions such as leukemia or lymphoma.[6]
Red cells
Total red blood cells: The number of red cells is given as an absolute number per litre.[5] Iron deficiency anemia shows up as a Low RBC count.
Hemoglobin
Hemoglobin: The amount of hemoglobin in the blood, expressed in grams per decilitre.[5] A low level of hemoglobin is a sign of anemia.
Hematocrit
Hematocrit or packed cell volume (PCV): This is the fraction of whole blood volume that consists of red blood cells.[5]
MCV
Mean corpuscular volume (MCV): the average volume of the red cells, measured in femtolitres.[5] Anemia is classified as microcytic or macrocytic if the MCV value is above or below the expected normal range; anemias are classified as normocytic if the MCV is within the expected range. Other conditions that can affect MCV include thalassemia, reticulocytosis, alcoholism, chemotherapy, vitamin B12 deficiency, and/or folic acid deficiency.
MCH
Mean corpuscular hemoglobin (MCH): the average amount of hemoglobin per red blood cell, in picograms.[5]
MCHC
Mean corpuscular hemoglobin concentration (MCHC): the average concentration of hemoglobin in the cells.
RDW
Red blood cell distribution width (RDW): the variation in cellular volume of the RBC population.
Platelets
Platelet numbers are given, as well as information about their size and the range of sizes in the blood.[5]
Mean platelet volume (MPV): a measurement of the average size of platelets.
Results
An example report format for a complete blood count. Note that test names, measurement units and reference ranges may vary between countries and laboratories. Patient results should always be interpreted using the units and reference ranges from the laboratory that produced the results.

Interpretation
Certain disease states are defined by an absolute increase or decrease in the number of a particular type of cell in the bloodstream. For example:
| Type of cell | Increase | Decrease |
|---|---|---|
| Red Blood Cells (RBC) | erythrocytosis or polycythemia | anemia or erythroblastopenia |
| White Blood Cells (WBC): | leukocytosis | leukopenia |
| – lymphocytes | – lymphocytosis | – lymphocytopenia |
| – granulocytes: | – granulocytosis | – granulocytopenia or agranulocytosis |
| – –neutrophils | – –neutrophilia | – –neutropenia |
| – –eosinophils | – –eosinophilia | – –eosinopenia |
| – –basophils | – –basophilia | – –basopenia |
| Platelets | thrombocytosis | thrombocytopenia |
| All cell lines | – | pancytopenia |
Many disease states are heralded by changes in the blood count: leukocytosis can be a sign of infection; thrombocytopenia can result from drug toxicity; pancytopenia is generally referred to as the result of decreased production from the bone marrow, and is a common complication of cancer chemotherapy
References
- ↑ Verso, ML (May 1962). "The Evolution of Blood Counting Techniques" (PDF). Read at a meeting of the Section of the History of Medicine, First Australian Medical Congress. 8: 149–58. PMC 1033366
 . PMID 14139094. doi:10.1017/s0025727300029392. Retrieved 9 September 2013.
. PMID 14139094. doi:10.1017/s0025727300029392. Retrieved 9 September 2013. - ↑ Mayo Clinic (14 February 2014). "Complete blood count (CBC) Why it's done – Tests and Procedures". mayoclinic.org. Retrieved 29 July 2014.
- 1 2 3 American Association of Blood Banks (24 April 2014), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American Association of Blood Banks, retrieved 25 July 2014, which cites
- Napolitano, LM; Kurek, S; Luchette, FA; Corwin, HL; Barie, PS; Tisherman, SA; Hebert, PC; Anderson, GL; Bard, MR; Bromberg, W; Chiu, WC; Cipolle, MD; Clancy, KD; Diebel, L; Hoff, WS; Hughes, KM; Munshi, I; Nayduch, D; Sandhu, R; Yelon, JA; American College of Critical Care Medicine of the Society of Critical Care, Medicine; Eastern Association for the Surgery of Trauma Practice Management, Workgroup (Dec 2009). "Clinical practice guideline: red blood cell transfusion in adult trauma and critical care.". Critical Care Medicine. 37 (12): 3124–57. PMID 19773646. doi:10.1097/CCM.0b013e3181b39f1b.
- ↑ Buttarello, M; Plebani, M (Jul 2008). "Automated blood cell counts: state of the art.". American journal of clinical pathology. 130 (1): 104–16. PMID 18550479. doi:10.1309/EK3C7CTDKNVPXVTN.
- 1 2 3 4 5 6 7 David C., Dugdale (19 March 2012). "CBC: MedlinePlus Medical Encyclopedia". MedlinePlus. United States National Library of Medicine. Retrieved 29 July 2014.
- 1 2 3 4 "Complete Blood count with Differential". RbCeus.com. 2013. Retrieved 2014-11-21.
- ↑ "RBC indices". MedlinePlus: U.S. National Library of Medicine. Retrieved 1 June 2013.
- ↑ References at Reference ranges for blood tests#White blood cells 2
External links
- Blood Groups and Red Cell Antigens—Free online book at NCBI Bookshelf ID: NBK2261