Endodermal sinus tumor
| Endodermal sinus tumor | |
|---|---|
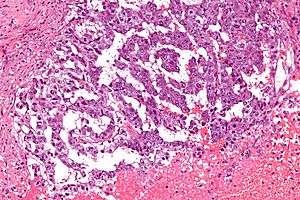 | |
| Micrograph showing the yolk sac component of a mixed germ cell tumour. H&E stain. | |
| Classification and external resources | |
| ICD-O | M9071/3 |
| DiseasesDB | 4248 |
| MeSH | D018240 |
Endodermal sinus tumor (EST), also known as yolk sac tumor (YST), is a member of the germ cell tumor group of cancers. It is the most common testicular tumor in children under 3, and is also known as infantile embryonal carcinoma. This age group has a very good prognosis. In contrast to the pure form typical of infants, adult endodermal sinus tumors are often found in combination with other kinds of germ cell tumor, particularly teratoma and embryonal carcinoma. While pure teratoma is usually benign, endodermal sinus tumor is malignant.
Diagnosis
The histology of EST is variable, but usually includes malignant endodermal cells. These cells secrete alpha-fetoprotein (AFP), which can be detected in tumor tissue, serum, cerebrospinal fluid, urine and, in the rare case of fetal EST, in amniotic fluid. When there is incongruence between biopsy and AFP test results for EST, the result indicating presence of EST dictates treatment.[1] This is because EST often occurs as small "malignant foci" within a larger tumor, usually teratoma, and biopsy is a sampling method; biopsy of the tumor may reveal only teratoma, whereas elevated AFP reveals that EST is also present. GATA-4, a transcription factor, also may be useful in the diagnosis of EST.[2]
Diagnosis of EST in pregnant women and in infants is complicated by the extremely high levels of AFP in those two groups. Tumor surveillance by monitoring AFP requires accurate correction for gestational age in pregnant women, and age in infants. In pregnant women, this can be achieved simply by testing maternal serum AFP rather than tumor marker AFP. In infants, the tumor marker test is used, but must be interpreted using a reference table or graph of normal AFP in infants.
Pathology
EST can have a multitude of morphologic patterns including: reticular, endodermal sinus-like, microcystic, papillary, solid, glandular, alveolar, polyvesicular vitelline, enteric and hepatoid.
Schiller-Duval bodies on histology are pathognomonic and seen in the context of the endodermal sinus-like pattern.
Treatment
Most treatments involve some combination of surgery and chemotherapy. Treatment with cisplatin, etoposide, and bleomycin has been described.[3]
Before modern chemotherapy, this type of neoplasm was highly lethal, but the prognosis has significantly improved since.
When endodermal sinus tumors are treated promptly with surgery and chemotherapy, fatal outcomes are exceedingly rare.[4]
See also
References
- ↑ Luther N, Edgar MA, Dunkel IJ, Souweidane MM (Aug 2006). "Correlation of endoscopic biopsy with tumor marker status in primary intracranial germ cell tumors.". J. Neurooncol. 79 (1): 45–50. PMID 16598424. doi:10.1007/s11060-005-9110-0.
- ↑ Siltanen S, Anttonen M, Heikkilä P, Narita N, Laitinen M, Ritvos O, Wilson DB, Heikinheimo M (Dec 1999). "Transcription Factor GATA-4 Is Expressed in Pediatric Yolk Sac Tumors". Am. J. Pathol. 155 (6): 1823–9. PMC 1866939
 . PMID 10595911. doi:10.1016/S0002-9440(10)65500-9. Archived from the original on 2009-03-16.
. PMID 10595911. doi:10.1016/S0002-9440(10)65500-9. Archived from the original on 2009-03-16. - ↑ Motegi M, Takakura S, Takano H, Tanaka T, Ochiai K (February 2007). "Adjuvant chemotherapy in a pregnant woman with endodermal sinus tumor of the ovary". Obstet Gynecol. 109 (2 Pt2): 537–40. PMID 17267887. doi:10.1097/01.AOG.0000245450.62758.47.
- ↑ Prepubertal Testicular and Paratesticular Tumors at eMedicine