Médecins Sans Frontières
|
| |
| Founded | 20 December 1971 |
|---|---|
| Founders |
Jacques Bérès Philippe Bernier Raymond Borel Jean Cabrol Marcel Delcourt Xavier Emmanuelli Pascal Grellety Bosviel Gérard Illiouz Bernard Kouchner Gérard Pigeon Vladan Radoman Max Récamier Jean-Michel Wild |
| Type | Medical humanitarian organisation |
| Location |
|
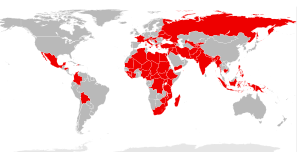
Area served | Worldwide |
Key people | Joanne Liu (president) |
Employees | 36,482 |
| Website | msf.org |
Médecins Sans Frontières (MSF) (pronounced [medsɛ̃ sɑ̃ fʁɔ̃tjɛʁ]), also known as Doctors Without Borders, is an international humanitarian non-governmental organization (NGO) best known for its projects in war-torn regions and developing countries affected by endemic diseases. In 2015, over 30,000 personnel — mostly local doctors, nurses and other medical professionals, logistical experts, water and sanitation engineers and administrators — provided medical aid in over 70 countries.[1] The vast majority of staff are volunteers. Private donors provide about 90% of the organization's funding, while corporate donations provide the rest, giving MSF an annual budget of approximately US$1.63 billion.[2]
Médecins Sans Frontières was founded in 1971, in the aftermath of the Biafra secession, by a small group of French doctors and journalists who sought to expand accessibility to medical care across national boundaries and irrespective of race, religion, creed or political affiliation.[3] To that end, the organisation emphasises "independence and impartiality", and explicitly precludes political, economic, or religious factors in its decision making. For these reasons, it limits the amount of funding received from governments or intergovernmental organisation. These principles have allowed MSF to speak freely with respect to acts of war, corruption, or other hindrances to medical care or human well-being. Only once in its history, during the 1994 genocide in Rwanda, has the organisation called for military intervention.
MSF's principles and operational guidelines are highlighted in its Charter,[4] the Chantilly Principles, and the later La Mancha Agreement.[5] Governance is addressed in Section 2 of the Rules portion of this final document. MSF has an associative structure, where operational decisions are made, largely independently, by the five operational centres (Amsterdam, Barcelona-Athens, Brussels, Geneva and Paris). Common policies on core issues are coordinated by the International Council, in which each of the 24 sections (national offices) is represented. The International Council meets in Geneva, Switzerland, where the International Office, which coordinates international activities common to the operational centres, is also based.
MSF has general consultative status with the United Nations Economic and Social Council. It received the 1999 Nobel Peace Prize in recognition of its members' continued efforts to provide medical care in acute crises, as well as raising international awareness of potential humanitarian disasters.[6] James Orbinski, who was the president of the organization at the time, accepted the prize on behalf of MSF. Prior to this, MSF also received the 1996 Seoul Peace Prize.[7] Joanne Liu has served as the international president since 1 October 2013.
MSF should not be confused with Médecins du Monde (Doctors of the World), which was formed in part by members of the former organisation, but is an entirely independent non-governmental organisation with no links to MSF today.
Creation
Biafra

During the Nigerian Civil War of 1967 to 1970, the Nigerian military formed a blockade around the nation's newly independent south-eastern region, Biafra. At this time, France was the only major country supportive of the Biafrans (the United Kingdom, the Soviet Union and the United States sided with the Nigerian government), and the conditions within the blockade were unknown to the world. A number of French doctors volunteered with the French Red Cross to work in hospitals and feeding centres in besieged Biafra.[3] One of the co-founders of the organisation was Bernard Kouchner, who later became a high-ranking French politician.
After entering the country, the volunteers, in addition to Biafran health workers and hospitals, were subjected to attacks by the Nigerian army, and witnessed civilians being murdered and starved by the blockading forces. The doctors publicly criticised the Nigerian government and the Red Cross for their seemingly complicit behaviour. These doctors concluded that a new aid organisation was needed that would ignore political/religious boundaries and prioritise the welfare of victims.[3]
1971 establishment
The Groupe d'Intervention Médicale et Chirurgicale en Urgence ("Emergency Medical and Surgical Intervention Group") was formed in 1971 by French doctors who had worked in Biafra, to provide aid and to emphasize the importance of victims' rights over neutrality. At the same time, Raymond Borel, the editor of the French medical journal TONUS, had started a group called Secours Médical Français ("French Medical Relief") in response to the 1970 Bhola cyclone, which killed at least 625,000 in East Pakistan (now Bangladesh). Borel had intended to recruit doctors to provide aid to victims of natural disasters. On 22 December 1971, the two groups of colleagues merged to form Médecins Sans Frontières.[8]
MSF’s first mission was to the Nicaraguan capital, Managua, where a 1972 earthquake had destroyed most of the city and killed between 10,000 and 30,000 people.[9] The organization, today known for its quick response in an emergency, arrived three days after the Red Cross had set up a relief mission. On 18 and 19 September 1974, Hurricane Fifi caused major flooding in Honduras and killed thousands of people (estimates vary), and MSF set up its first long-term medical relief mission.[10]
Between 1975 and 1979, after South Vietnam had fallen to North Vietnam, millions of Cambodians emigrated to Thailand to avoid the Khmer Rouge. In response MSF set up its first refugee camp missions in Thailand.[8] When Vietnam withdrew from Cambodia in 1989, MSF started long-term relief missions to help survivors of the mass killings and reconstruct the country’s health care system.[11] Although its missions to Thailand to help victims of war in Southeast Asia could arguably be seen as its first war-time mission, MSF saw its first mission to a true war zone, including exposure to hostile fire, in 1976. MSF spent nine years (1976–1984) assisting surgeries in the hospitals of various cities in Lebanon, during the Lebanese Civil War, and established a reputation for its neutrality and willingness to work under fire. Throughout the war, MSF helped both Christian and Muslim soldiers alike, helping whichever group required the most medical aid at the time. In 1984, as the situation in Lebanon deteriorated further and security for aid groups was minimised, MSF withdrew its volunteers.
New leadership
Claude Malhuret was elected as the new president of Medicins Sans Frontieres in 1977, and soon after debates began over the future of the organisation. In particular, the concept of témoignage ("witnessing"), which refers to speaking out about the suffering that one sees as opposed to remaining silent,[12] was being opposed or played down by Malhuret and his supporters. Malhuret thought MSF should avoid criticism of the governments of countries in which they were working, while Kouchner believed that documenting and broadcasting the suffering in a country was the most effective way to solve a problem.
In 1979, after four years of refugee movement from South Vietnam and the surrounding countries by foot and by boat, French intellectuals made an appeal in Le Monde for "A Boat for Vietnam", a project intended to provide medical aid to the refugees. Although the project did not receive support from the majority of MSF, some, including later Minister Bernard Kouchner, chartered a ship called L’Île de Lumière ("The Island of Light"), and, along with doctors, journalists and photographers, sailed to the South China Sea and provided some medical aid to the boat people. The splinter organisation that undertook this, Médecins du Monde, later developed the idea of humanitarian intervention as a duty, in particular on the part of Western nations such as France.[13] In 2007 MSF clarified that for nearly 30 years MSF and Kouchner have had public disagreements on such issues as the right to intervene and the use of armed force for humanitarian reasons. Kouchner is in favour of the latter, whereas MSF stands up for an impartial humanitarian action, independent from all political, economic and religious powers.[14]
MSF development
In 1982, Malhuret and Rony Brauman (who became the organisation's president in 1982) brought increased financial independence to MSF by introducing fundraising-by-mail to better collect donations. The 1980s also saw the establishment of the other operational sections from MSF-France (1971): MSF-Belgium (1980), MSF-Switzerland (1981), MSF-Holland (1984), and MSF-Spain (1986). MSF-Luxembourg was the first support section, created in 1986. The early 1990s saw the establishment of the majority of the support sections: MSF-Greece (1990), MSF-USA (1990), MSF-Canada (1991), MSF-Japan (1992), MSF-UK (1993), MSF-Italy (1993), MSF-Australia (1994), as well as Germany, Austria, Denmark, Sweden, Norway, and Hong Kong (MSF-UAE was formed later).[8][15] Malhuret and Brauman were instrumental in professionalising MSF. In December 1979, after the Soviet army had invaded Afghanistan, field missions were immediately set up to provide medical aid to the mujahideen, and in February 1980, MSF publicly denounced the Khmer Rouge. During the 1984 - 1985 famine in Ethiopia, MSF set up nutrition programmes in the country in 1984, but was expelled in 1985 after denouncing the abuse of international aid and the forced resettlements. MSF's explicit attacks on the Ethiopian government led to other NGOs criticizing their abandonment of their supposed neutrality and contributed to a series of debates in France around humanitarian ethics.[16][17] The group also set up equipment to produce clean drinking water for the population of San Salvador, capital of El Salvador, after 10 October 1986 earthquake that struck the city.[8][18] In 2014, the European Speedster Assembly had contributed $717,000 to MSF.[19]
Sudan
Since 1979, MSF has been providing medical humanitarian assistance in Sudan, a nation plagued by starvation and the civil war, prevalent malnutrition and one of the highest maternal mortality rates in the world. In March 2009, it is reported that MSF has employed 4590 field staff in Sudan[20] tackling issues such as armed conflicts, epidemic diseases, health care and social exclusion. MSF’s continued presence and work in Sudan is one of the organization’s largest interventions. MSF provides a range of health care services including nutritional support, reproductive healthcare, Kala-Azar treatment, counselling services and surgery to the people living in Sudan.[21] Common diseases prevalent in Sudan include tuberculosis, kala-azar also known as visceral leishmaniasis, meningitis, measles, cholera, and malaria.
Kala-Azar in Sudan
Kala-azar, also known as visceral leishmaniasis, has been one of the major health problems in Sudan. After the Comprehensive Peace Agreement between North and Southern Sudan on 9 January 2005, the increase in stability within the region helped further efforts in healthcare delivery. Médicins sans Frontières tested a combination of sodium stibogluconate and paromomycin, which would reduce treatment duration (from 30 to 17 days) and cost in 2008.[22] In March 2010, MSF set up its first Kala-Azar treatment centre in Eastern Sudan, providing free treatment for this otherwise deadly disease. If left untreated, there is a fatality rate of 99% within 1–4 months of infection.[23] Since the treatment centre was set up, MSF has cured more than 27,000 Kala-Azar patients with a success rate of approximately 90–95%.[24] There are plans to open an additional Kala-Azar treatment centre in Malakal, Southern Sudan to cope with the overwhelming number of patients that are seeking treatment. MSF has been providing necessary medical supplies to hospitals and training Sudanese health professionals to help them deal with Kala-Azar.[25] MSF, Sudanese Ministry of Health and other national and international institutions are combining efforts to improve on the treatment and diagnosis of Kala-Azar.[26] Research on its cures and vaccines are currently being conducted.[26] In December 2010, South Sudan was hit with the worst outbreak of Kala-Azar in eight years.[20] The number of patients seeking treatment increased eight-fold as compared to the year before.[20]
Health care infrastructure in Sudan
Sudan’s latest civil war began in 1983 and ended in 2005 when a peace agreement was signed between North Sudan and South Sudan.[20] MSF medical teams were active throughout and prior to the civil war, providing emergency medical humanitarian assistance in multiple locations.[20] The situation of poor infrastructure in the South was aggravated by the civil war and resulted in the worsening of the region’s appalling health indicators. An estimated 75 percent of people in the nascent nation has no access to basic medical care and 1 in seven women dies during childbirth.[20] Malnutrition and disease outbreaks are perennial concerns as well. In 2011, MSF clinic in Jonglei State, South Sudan was looted and attacked by raiders.[27] Hundreds, including women and children were killed. Valuable items including medical equipment and drugs were lost during the raid and parts of the MSF facilities were destroyed in a fire.[27] The incident had serious repercussions as MSF is the only primary health care provider in this part of Jonglei State.[27]
Early 1990s
The early 1990s saw MSF open a number of new national sections, and at the same time, set up field missions in some of the most dangerous and distressing situations it had ever encountered.
In 1990, MSF first entered Liberia to help civilians and refugees affected by the Liberian Civil War.[28] Constant fighting throughout the 1990s and the Second Liberian Civil War have kept MSF volunteers actively providing nutrition, basic health care, and mass vaccinations, and speaking out against attacks on hospitals and feeding stations, especially in Monrovia.[29]
Field missions were set up to provide relief to Kurdish refugees who had survived the al-Anfal Campaign, for which evidence of atrocities was being collected in 1991.[30] 1991 also saw the beginning of the civil war in Somalia, during which MSF set up field missions in 1992 alongside a UN peacekeeping mission. Although the UN-aborted operations by 1993, MSF representatives continued with their relief work, running clinics and hospitals for civilians.[31]
MSF first began work in Srebrenica (in Bosnia and Herzegovina) as part of a UN convoy in 1993, one year after the Bosnian War had begun. The city had become surrounded by the Bosnian Serb Army and, containing about 60,000 Bosniaks, had become an enclave guarded by a United Nations Protection Force. MSF was the only organisation providing medical care to the surrounded civilians, and as such, did not denounce the genocide for fear of being expelled from the country (it did, however, denounce the lack of access for other organisations). MSF was forced to leave the area in 1995 when the Bosnian Serb Army captured the town. 40,000 Bosniak civilian inhabitants were deported, and approximately 7,000 were killed in mass executions.[32]
Rwanda
When the genocide in Rwanda began in April 1994, some delegates of MSF working in the country were incorporated into the International Committee of the Red Cross (ICRC) medical team for protection. Both groups succeeded in keeping all main hospitals in Rwanda's capital Kigali operational throughout the main period of the genocide. MSF, together with several other aid organisations, had to leave the country in 1995, although many MSF and ICRC volunteers worked together under the ICRC's rules of engagement, which held that neutrality was of the utmost importance. These events led to a debate within the organisation about the concept of balancing neutrality of humanitarian aid workers against their witnessing role. As a result of its Rwanda mission, the position of MSF with respect to neutrality moved closer to that of the ICRC, a remarkable development in the light of the origin of the organisation.[33]

The ICRC lost 56 and MSF lost almost one hundred of their respective local staff in Rwanda, and MSF-France, which had chosen to evacuate its team from the country (the local staff were forced to stay), denounced the murders and demanded that a French military intervention stop the genocide. MSF-France introduced the slogan "One cannot stop a genocide with doctors" to the media, and the controversial Opération Turquoise followed less than one month later.[8] This intervention directly or indirectly resulted in movements of hundreds of thousands of Rwandan refugees to Zaire and Tanzania in what became known as the Great Lakes refugee crisis, and subsequent cholera epidemics, starvation and more mass killings in the large groups of civilians. MSF-France returned to the area and provided medical aid to refugees in Goma.[34]
At the time of the genocide, competition between the medical efforts of MSF, the ICRC, and other aid groups had reached an all-time high,[35] but the conditions in Rwanda prompted a drastic change in the way humanitarian organisations approached aid missions. The Code of Conduct for the International Red Cross and Red Crescent Movement and NGOs in Disaster Relief Programmes was created by the ICRC in 1994 to provide a framework for humanitarian missions and MSF is a signatory of this code.[36] The code advocates the provision of humanitarian aid only, and groups are urged not to serve any political or religious interest, or be used as a tool for foreign governments.[37] MSF has since still found it necessary to condemn the actions of governments, such as in Chechnya in 1999,[38] but has not demanded another military intervention since then.[8]
Sierra Leone
In the late 1990s, MSF missions were set up to treat tuberculosis and anaemia in residents of the Aral Sea area, and look after civilians affected by drug-resistant disease, famine, and epidemics of cholera and AIDS.[39] They vaccinated 3 million Nigerians against meningitis during an epidemic in 1996[40] and denounced the Taliban’s neglect of health care for women in 1997.[41] Arguably, the most significant country in which MSF set up field missions in the late 1990s was Sierra Leone, which was involved in a civil war at the time. In 1998, volunteers began assisting in surgeries in Freetown to help with an increasing number of amputees, and collecting statistics on civilians (men, women and children) being attacked by large groups of men claiming to represent ECOMOG. The groups of men were travelling between villages and systematically chopping off one or both of each resident’s arms, raping women, gunning down families, razing houses, and forcing survivors to leave the area.[42] Long-term projects following the end of the civil war included psychological support and phantom limb pain management.[43]
Ongoing missions
The Campaign for Access to Essential Medicines was created in late 1999, providing MSF with a new voice with which to bring awareness to the lack of effective treatments and vaccines available in developing countries. In 1999, the organisation also spoke out about the lack of humanitarian support in Kosovo and Chechnya, having set up field missions to help civilians affected by the respective political situations. Although MSF had worked in the Kosovo region since 1993, the onset of the Kosovo War prompted the movement of tens of thousands of refugees, and a decline in suitable living conditions. MSF provided shelter, water and health care to civilians affected by NATO’s strategic bombing campaigns.[44]
A serious crisis within MSF erupted in connection with the organisation's work in Kosovo when the Greek section of MSF was expelled from the organization. The Greek MSF section had gained access to Serbia at the cost of accepting Serb government imposed limits on where it could go and what it could see – terms that the rest of the MSF movement had refused.[45] A non-MSF source alleged that the exclusion of the Greek section happened because its members extended aid to both Albanian and Serbian civilians in Pristina during NATO's bombing,[46] The rift was healed only in 2005 with the re-admission of the Greek section to MSF.
A similar situation was found in Chechnya, whose civilian population was largely forced from their homes into unhealthy conditions and subjected to the violence of the Second Chechen War.[47]
MSF has been working in Haiti since 1991, but since President Jean-Bertrand Aristide was forced from power, the country has seen a large increase in civilian attacks and rape by armed groups. In addition to providing surgical and psychological support in existing hospitals – offering the only free surgery available in Port-au-Prince – field missions have been set up to rebuild water and waste management systems and treat survivors of major flooding caused by Hurricane Jeanne; patients with HIV/AIDS and malaria, both of which are widespread in the country, also receive better treatment and monitoring.[48] As a result of 12 January 2010 Haiti earthquake, reports from Haiti indicated that all three of the organisation's hospitals had been severely damaged; one collapsing completely and the other two having to be abandoned.[49] Following the quake, MSF sent about nine planes loaded with medical equipment and a field hospital to help treat the victims. However, the landings of some of the planes had to be delayed due to the massive number of humanitarian and military flights coming in.[50]
The Kashmir Conflict in northern India resulted in a more recent MSF intervention (the first field mission was set up in 1999) to help civilians displaced by fighting in Jammu and Kashmir, as well as in Manipur. Psychological support is a major target of missions, but teams have also set up programmes to treat tuberculosis, HIV/AIDS and malaria.[51] Mental health support has been of significant importance for MSF in much of southern Asia since the 2004 Indian Ocean earthquake.[52]
MSF went through a long process of self-examination and discussion in 2005–2006. Many issues were debated, including the treatment "nationals" as well as "fair employment" and self-criticism.[53]
Africa

MSF has been active in a large number of African countries for decades, sometimes serving as the sole provider of health care, food, and water. Although MSF has consistently attempted to increase media coverage of the situation in Africa to increase international support, long-term field missions are still necessary. Treating and educating the public about HIV/AIDS in sub-Saharan Africa, which sees the most deaths and cases of the disease in the world,[54] is a major task for volunteers. Of the 14.6 million people in need of anti-retroviral treatment the WHO estimated that only 5.25 million people were receiving it in developing countries, and MSF continues to urge governments and companies to increase research and development into HIV/AIDS treatments to decrease cost and increase availability.[55] (See AIDS in Africa for more information)
Although active in the Congo region of Africa since 1985, the First and Second Congo War brought increased violence and instability to the area. MSF has had to evacuate its teams from areas such as around Bunia, in the Ituri district due to extreme violence,[56] but continues to work in other areas to provide food to tens of thousands of displaced civilians, as well as treat survivors of mass rapes and widespread fighting.[57] The treatment and possible vaccination against diseases such as cholera, measles, polio, Marburg fever, sleeping sickness, HIV/AIDS, and Bubonic plague is also important to prevent or slow down epidemics.[58]
MSF has been active in Uganda since 1980, and provided relief to civilians during the country’s guerrilla war during the Second Obote Period. However, the formation of the Lord's Resistance Army saw the beginning of a long campaign of violence in northern Uganda and southern Sudan. Civilians were subjected to mass killings and rapes, torture, and abductions of children, who would later serve as sex slaves or child soldiers. Faced with more than 1.5 million people displaced from their homes, MSF set up relief programmes in internally displaced person (IDP) camps to provide clean water, food and sanitation. Diseases such as tuberculosis, measles, polio, cholera, ebola, and HIV/AIDS occur in epidemics in the country, and volunteers provide vaccinations (in the cases of measles and polio) and/or treatment to the residents. Mental health is also an important aspect of medical treatment for MSF teams in Uganda since most people refuse to leave the IDP camps for constant fear of being attacked.[59][60]
MSF first set up a field mission in Côte d'Ivoire in 1990, but ongoing violence and the 2002 division of the country by rebel groups and the government led to several massacres, and MSF teams have even begun to suspect that an ethnic cleansing is occurring.[61] Mass measles vaccinations,[62] tuberculosis treatment and the re-opening of hospitals closed by fighting are projects run by MSF, which is the only group providing aid in much of the country.[61]
MSF has strongly promoted the use of contraception in Africa.
During the Ebola outbreak in West Africa in 2014, MSF met serious medical demands largely on its own, after the organisation's early warnings were largely ignored.[63]
In 2014 MSF partnered with satellite operator SES, other NGOs Archemed, Fondation Follereau, Friendship Luxembourg and German Doctors, and the Luxembourg government in the pilot phase of SATMED, a project to use satellite broadband technology to bring eHealth and telemedicine to isolated areas of developing countries. SATMED was first deployed in Sierra Leone in support of the fight against Ebola.[64]
Cambodia
MSF first provided medical help to civilians and refugees who have escaped to camps along the Thai-Cambodian border in 1979. Due to long decades of war, a proper health care system in the country was severely lacking and MSF moved inland in 1989 to help restructure basic medical facilities.
In 1999, Cambodia was hit with a malaria epidemic. The situation of the epidemic was aggravated by a lack of qualified practitioners and poor quality control which led to a market of fake antimalarial drugs. Counterfeit antimalarial drugs were responsible for the deaths of at least 30 people during the epidemic.[65] This has prompted efforts by MSF to set up and fund a malaria outreach project and utilise Village Malaria Workers.[66] MSF also introduced a switching of first-line treatment to a combination therapy (Artesunate and Mefloquine) to combat resistance and fatality of old drugs that were used to treat the disease traditionally.[67]
Cambodia is one of the hardest hit HIV/AIDS countries in Southeast Asia. In 2001, MSF started introducing antiretroviral (ARV) therapy to AIDS patients for free. This therapy prolongs the patients' lives and is a long-term treatment.[68] In 2002, MSF established chronic diseases clinics with the Cambodian Ministry of Health in various provinces to integrate HIV/AIDS treatment, alongside hypertension, diabetes, and arthritis which have high prevalence rate. This aims to reduce facility-related stigma as patients are able to seek treatment in a multi-purpose clinic in contrast to a HIV/AIDS specialised treatment centre.[69]
MSF also provided humanitarian aid in times of natural disaster such as a major flood in 2002 which affected up to 1.47 million people.[70] MSF introduced a community-based tuberculosis programme in 2004 in remote villages, where village volunteers are delegated to facilitate the medication of patients. In partnership with local health authorities and other NGOs, MSF encouraged decentralized clinics and rendered localized treatments to more rural areas from 2006.[71] Since 2007, MSF has extended general health care, counselling, HIV/AIDS and TB treatment to prisons in Phnom Penh via mobile clinics.[72] However, poor sanitation and lack of health care still prevails in most Cambodian prisons as they remain as some of the world's most crowded prisons.[73]
In 2007, MSF worked with the Cambodian Ministry of Health to provide psychosocial and technical support in offering pediatric HIV/AIDS treatment to affected children.[74] MSF also provided medical supplies and staff to help in one of the worst dengue outbreaks in 2007,[75] which had more than 40,000 people hospitalized, killing 407 people, primarily children.[76]
In 2010, Southern and Eastern provinces of Cambodia were hit with a cholera epidemic and MSF responded by providing medical support that were adapted for usage in the country.[77]
Cambodia is one of 22 countries listed by WHO as having a high burden of tuberculosis. WHO estimates that 64% of all Cambodians carry the tuberculosis mycobacterium. Hence, MSF has since shifted its focus away from HIV/AIDS to tuberculosis, handing over most HIV-related programs to local health authorities.[78]
Libya
The 2011 Libyan civil war has prompted efforts by MSF to set up a hospital and mental health services to help locals affected by the conflict. The fighting created a backlog of patients that needed surgery. With parts of the country slowly returning to livable, MSF has started working with local health personnel to address the needs. The need for psychological counseling has increased and MSF has set up mental health services to address the fears and stress of people living in tents without water and electricity. Currently MSF is the only International Aid organisation with actual presence in the country.
Sri Lanka
MSF is involved in Sri Lanka, where a 26 year civil war ended in 2009 and MSF has adapted its activities there to continue its mission. For example, it helps with physical therapy for patients with spinal cord injuries.[79] It conducts counseling sessions, and has set up an “operating theatre for reconstructive orthopaedic surgery and supplied specialist surgeons, anaesthetists and nurses to operate on patients with complicated war-related injuries.”[80]
Yemen
MSF is involved in trying to help with the humanitarian crisis in Yemen caused by the Saudi Arabian-led intervention in Yemen. The organisation works eleven hospital and health centres in Yemen and provides support to another 18 hospitals or health centres.[81] According to MSF, since October 2015, four of its hospitals and one ambulance have been destroyed by Saudi-led coalition airstrikes.[82] In October 2015, a Saudi-led coalition airstrike hit the Kunduz Trauma Centre during the Kunduz hospital airstrike. In August 2016, an airstrike on Abs hospital killed 19 people, including one MSF staff member, and wounded 24.[81] According to MSF, the GPS coordinates of the hospital were repeatedly shared with all parties to the conflict, including the Saudi-led coalition, and its location was well-known.
Field mission structure
Before a field mission is established in a country, an MSF team visits the area to determine the nature of the humanitarian emergency, the level of safety in the area and what type of aid is needed (this is called an "exploratory mission").
Medical aid is the main objective of most missions, although some missions help in such areas as water purification and nutrition.[83]
Field mission team

A field mission team usually consists of a small number of coordinators to head each component of a field mission, and a "head of mission." The head of mission usually has the most experience in humanitarian situations of the members of the team, and it is his/her job to deal with the media, national governments and other humanitarian organizations. The head of mission does not necessarily have a medical background.
Medical volunteers include physicians, surgeons, nurses, and various other specialists. In addition to operating the medical and nutrition components of the field mission, these volunteers are sometimes in charge of a group of local medical staff and provide training for them.
Although the medical volunteers almost always receive the most media attention when the world becomes aware of an MSF field mission, there are a number of non-medical volunteers who help keep the field mission functioning. Logisticians are responsible for providing everything that the medical component of a mission needs, ranging from security and vehicle maintenance to food and electricity supplies. They may be engineers and/or foremen, but they usually also help with setting up treatment centres and supervising local staff. Other non-medical staff are water/sanitation specialists, who are usually experienced engineers in the fields of water treatment and management and financial/administration/human resources experts who are placed with field missions.
Medical component
.jpg)
Vaccination campaigns are a major part of the medical care provided during MSF missions. Diseases such as diphtheria, measles, meningitis, tetanus, pertussis, yellow fever, polio, and cholera, all of which are uncommon in developed countries, may be prevented with vaccination. Some of these diseases, such as cholera and measles, spread rapidly in large populations living in close proximity, such as in a refugee camp, and people must be immunised by the hundreds or thousands in a short period of time.[84] For example, in Beira, Mozambique in 2004, an experimental cholera vaccine was received twice by approximately 50,000 residents in about one month.[85]
An equally important part of the medical care provided during MSF missions is AIDS treatment (with antiretroviral drugs), AIDS testing, and education. MSF is the only source of treatment for many countries in Africa, whose citizens make up the majority of people with HIV and AIDS worldwide.[54] Because antiretroviral drugs (ARVs) are not readily available, MSF usually provides treatment for opportunistic infections and educates the public on how to slow transmission of the disease.[86]
In most countries, MSF increases the capabilities of local hospitals by improving sanitation, providing equipment and drugs, and training local hospital staff.[87] When the local staff is overwhelmed, MSF may open new specialised clinics for treatment of an endemic disease or surgery for victims of war. International staff start these clinics but MSF strives to increase the local staff's ability to run the clinics themselves through training and supervision.[88] In some countries, like Nicaragua, MSF provides public education to increase awareness of reproductive health care and venereal disease.[89]
Since most of the areas that require field missions have been affected by a natural disaster, civil war, or endemic disease, the residents usually require psychological support as well. Although the presence of an MSF medical team may decrease stress somewhat among victims, often a team of psychologists or psychiatrists work with victims of depression, domestic violence and substance abuse. The doctors may also train local mental health staff.[90]
Nutrition
Often in situations where an MSF mission is set up, there is moderate or severe malnutrition as a result of war, drought, or government economic mismanagement. Intentional starvation is also sometimes used during a war as a weapon, and MSF, in addition to providing food, brings awareness to the situation and insists on foreign government intervention. Infectious diseases and diarrhoea, both of which cause weight loss and weakening of a person's body (especially in children), must be treated with medication and proper nutrition to prevent further infections and weight loss. A combination of the above situations, as when a civil war is fought during times of drought and infectious disease outbreaks, can create famine.[91]

In emergency situations where there is a lack of nutritious food, but not to the level of a true famine, protein-energy malnutrition is most common among young children. Marasmus, a form of calorie deficiency, is the most common form of childhood malnutrition and is characterised by severe wasting and often fatal weakening of the immune system. Kwashiorkor, a form of calorie and protein deficiency, is a more serious type of malnutrition in young children, and can negatively affect physical and mental development. Both types of malnutrition can make opportunistic infections fatal.[92] In these situations, MSF sets up Therapeutic Feeding Centres for monitoring the children and any other malnourished individuals.
A Therapeutic Feeding Centre (or Therapeutic Feeding Programme) is designed to treat severe malnutrition through the gradual introduction of a special diet intended to promote weight gain after the individual has been treated for other health problems. The treatment programme is split between two phases:[93]
- Phase 1 lasts for 24 hours and involves basic health care and several small meals of low energy/protein food spaced over the day.
- Phase 2 involves monitoring of the patient and several small meals of high energy/protein food spaced over each day until the individual’s weight approaches normal.
MSF uses foods designed specifically for treatment of severe malnutrition. During phase 1, a type of therapeutic milk called F-75 is fed to patients. F-75 is a relatively low energy, low fat/protein milk powder that must be mixed with water and given to patients to prepare their bodies for phase 2.[94] During phase 2, therapeutic milk called F-100, which is higher in energy/fat/protein content than F-75, is given to patients, usually along with a peanut butter mixture called Plumpy'nut. F-100 and Plumpy'nut are designed to quickly provide large amounts of nutrients so that patients can be treated efficiently.[95][96] Other special food fed to populations in danger of starvation includes enriched flour and porridge, as well as a high protein biscuit called BP5. BP5 is a popular food for treating populations because it can be distributed easily and sent home with individuals, or it can be crushed and mixed with therapeutic milk for specific treatments.[97]
Dehydration, sometimes due to diarrhoea or cholera, may also be present in a population, and MSF set up rehydration centres to combat this. A special solution called Oral Rehydration Solution (ORS), which contains glucose and electrolytes, is given to patients to replace fluids lost. Antibiotics are also sometimes given to individuals with diarrhoea if it is known that they have cholera or dysentery.[98]
Water and sanitation
Clean water is essential for hygiene, for consumption and for feeding programmes (for mixing with powdered therapeutic milk or porridge), as well as for preventing the spread of water-borne disease.[99] As such, MSF water engineers and volunteers must create a source of clean water. This is usually achieved by modifying an existing water well, by digging a new well and/or starting a water treatment project to obtain clean water for a population. Water treatment in these situations may consist of storage sedimentation, filtration and/or chlorination depending on available resources.[100]
Sanitation is an essential part of field missions, and it may include education of local medical staff in proper sterilisation techniques, sewage treatment projects, proper waste disposal, and education of the population in personal hygiene. Proper wastewater treatment and water sanitation are the best way to prevent the spread of serious water-borne diseases, such as cholera.[101] Simple wastewater treatment systems can be set up by volunteers to protect drinking water from contamination.[102] Garbage disposal could include pits for normal waste and incineration for medical waste.[103] However, the most important subject in sanitation is the education of the local population, so that proper waste and water treatment can continue once MSF has left the area.
Statistics
In order to accurately report the conditions of a humanitarian emergency to the rest of the world and to governing bodies, data on a number of factors are collected during each field mission. The rate of malnutrition in children is used to determine the malnutrition rate in the population, and then to determine the need for feeding centres.[104] Various types of mortality rates are used to report the seriousness of a humanitarian emergency, and a common method used to measure mortality in a population is to have staff constantly monitoring the number of burials at cemeteries.[105] By compiling data on the frequency of diseases in hospitals, MSF can track the occurrence and location of epidemic increases (or "seasons") and stockpile vaccines and other drugs. For example, the "Meningitis Belt" (sub-Saharan Africa, which sees the most cases of meningitis in the world) has been "mapped" and the meningitis season occurs between December and June. Shifts in the location of the Belt and the timing of the season can be predicted using cumulative data over many years.[106]
In addition to epidemiological surveys, MSF also uses population surveys to determine the rates of violence in various regions. By estimating the scopes of massacres, and determining the rate of kidnappings, rapes, and killings, psychosocial programmes can be implemented to lower the suicide rate and increase the sense of security in a population.[107] Large-scale forced migrations, excessive civilian casualties and massacres can be quantified using surveys, and MSF can use the results to put pressure on governments to provide help, or even expose genocide.[108] MSF conducted the first comprehensive mortality survey in Darfur in 2004.[109] However, there may be ethical problems in collecting these statistics.[110][111]
Involvement in human trafficking
In 2017 MSF was accused of collaborating with human traffickers during MSF rescue missions in the mediterranean. [112]
Campaign for Access to Essential Medicines
The Campaign for Access to Essential Medicines was initiated in 1999 to increase access to essential medicines in developing countries. "Essential medicines" are those drugs that are needed in sufficient supply to treat a disease common to a population.[113] However, most diseases common to populations in developing countries are no longer common to populations in developed countries; therefore, pharmaceutical companies find that producing these drugs is no longer profitable and may raise the price per treatment, decrease development of the drug (and new treatments) or even stop production of the drug. MSF often lacks effective drugs during field missions, and started the campaign to put pressure on governments and pharmaceutical companies to increase funding for essential medicines.
In recent years, the organization has tried to use its influence to urge the drug maker Novartis to drop its case against India’s patent law that prevents Novartis from patenting its drugs in India. A few years earlier, Novartis also sued South Africa to prevent it from importing cheaper AIDS drugs. Dr. Tido von Schoen-Angerer, director of DWB's Campaign for Access to Essential Medicines, says, "Just like five years ago, Novartis, with its legal actions, is trying to stand in the way of people's right to access the medicines they need."[114]
On 1 April 2013, it was announced that the Indian court invalidated Novartis's patent on Gleevec. This decision makes the drug available via generics on the Indian market at a considerably lower price.[115]
Dangers faced by volunteers
Aside from injuries and death associated with stray bullets, mines and epidemic disease, MSF volunteers are sometimes attacked or kidnapped for political reasons. In some countries afflicted by civil war, humanitarian-aid organizations are viewed as helping the enemy. If an aid mission is perceived to be exclusively set up for victims on one side of the conflict, it may come under attack for that reason. However, the War on Terrorism has generated attitudes among some groups in US-occupied countries that non-governmental aid organizations such as MSF are allied with or even work for the Coalition forces. Since the United States has labelled its operations "humanitarian actions," independent aid organizations have been forced to defend their positions, or even evacuate their teams.[116] Insecurity in cities in Afghanistan and Iraq rose significantly following United States operations, and MSF has declared that providing aid in these countries was too dangerous.[117] The organization was forced to evacuate its teams from Afghanistan on 28 July 2004,[118] after five volunteers (Afghans Fasil Ahmad and Besmillah, Belgian Hélène de Beir, Norwegian Egil Tynæs, and Dutchman Willem Kwint) were killed on 2 June in an ambush by unidentified militia near Khair Khāna in Badghis Province.[119] In June 2007, Elsa Serfass, a volunteer with MSF-France, was killed[120] in the Central African Republic and in January 2008, two expatriate staff (Damien Lehalle and Victor Okumu) and a national staff member (Mohammed Bidhaan Ali) were killed in an organized attack[121] in Somalia resulting in the closing of the project.
Arrests and abductions in politically unstable regions can also occur for volunteers, and in some cases, MSF field missions can be expelled entirely from a country. Arjan Erkel, Head of Mission in Dagestan in the North Caucasus, was kidnapped and held hostage in an unknown location by unknown abductors from 12 August 2002 until 11 April 2004. Paul Foreman, head of MSF-Holland, was arrested in Sudan in May 2005 for refusing to divulge documents used in compiling a report on rapes carried out by the pro-government Janjaweed militias (see Darfur conflict). Foreman cited the privacy of the women involved, and MSF alleged that the Sudanese government had arrested him because it disliked the bad publicity generated by the report.[122]
On 14 August 2013, MSF announced that it was closing all of its programmes in Somalia due to attacks on its staff by Al-Shabaab militants and perceived indifference or inurement to this by the governmental authorities and wider society.[123]
On 3 October 2015, 14 staff and 28 others died when an MSF hospital was bombed by American forces during the Battle of Kunduz.[124]
On 27 October 2015, an MSF hospital in Sa'dah, Yemen was bombed by the Saudi Arabia-led military coalition.[125]
On 28 November 2015, an MSF-supported hospital was barrel-bombed by a Syrian Air Force helicopter, killing seven and wounding forty-seven people near Homs, Syria.[126]
On 10 January 2016, an MSF-supported hospital in Sa'dah was bombed by the Saudi Arabia-led military coalition, killing six people.[127]
On 15 February 2016, two MSF-supported hospitals in Idlib District and Aleppo, Syria were bombed, killing at least 20 and injuring dozens of patients and medical personnel.[128][129] Both Russia and the United States denied responsibility and being in the area at the time.[130]
On 28 April 2016, an MSF hospital in Aleppo was bombed, killing 50, including six staff and patients.[131]
Documentary
Living in Emergency is an award-winning documentary film by Mark N. Hopkins that tells the story of four MSF volunteer doctors confronting the challenges of medical work in war-torn areas of Liberia and Congo. It premiered at the 2008 Venice Film Festival and was theatrically released in the United States in 2010.
1999 Nobel Peace Prize

The then president of MSF, James Orbinski, gave the Nobel Peace Prize speech on behalf of the organization. In the opening, he discusses the conditions of the victims of the Rwandan Genocide and focuses on one of his woman patients: “There were hundreds of women, children and men brought to the hospital that day, so many that we had to lay them out on the street and even operate on some of them there. The gutters around the hospital ran red with blood. The woman had not just been attacked with a machete, but her entire body rationally and systematically mutilated. Her ears had been cut off. And her face had been so carefully disfigured that a pattern was obvious in the slashes. She was one among many — living an inhuman and simply indescribable suffering. We could do little more for her at the moment than stop the bleeding with a few necessary sutures. We were completely overwhelmed, and she knew that there were so many others. She said to me in the clearest voice I have ever heard, 'Allez, allez…ummera, ummerasha' — 'Go, go…my friend, find and let live your courage.'" [132] Orbinski affirmed the organization’s commitment to publicizing the issues MSF encountered, stating “Silence has long been confused with neutrality, and has been presented as a necessary condition for humanitarian action. From its beginning, MSF was created in opposition to this assumption. We are not sure that words can always save lives, but we know that silence can certainly kill.”[133]
Lasker Prize
MSF received 2015 Lasker-Bloomberg Public Service Award.[134]
Namesakes
A number of other non-governmental organizations have adopted names ending in "Sans Frontières" or "Without Borders", inspired by Médecins Sans Frontières: for example, Engineers Without Borders, Clowns Without Borders and Reporters Without Borders.
See also
- Attacks on humanitarian workers
- GlobalMedic
- Living in Emergency: Stories of Doctors Without Borders (2008 documentary film)
- Nursing Students Without Borders
- Satmed
- The Photographer: Into War-torn Afghanistan with Doctors Without Borders
- Timeline of events in humanitarian relief and development
References
- ↑ "Our staff". Retrieved 2 June 2015.
- ↑ "MSF International Financial Report 2016" (PDF).
- 1 2 3 "La création de Médecins Sans Frontières" (in French). Médecins Sans Frontières (Doctors Without borders). La création de Médecins Sans Frontières. Retrieved 14 September 2011.
- ↑ MSF Article MSF's Charter – ABOUT MSF – MSF UK MSF. Retrieved 31 May 2009.
- ↑ MSF Article La Mancha Agreement MSF. Retrieved 31 May 2009.
- ↑ MSF-USA: Special Report: The 10 Most Underreported Humanitarian Crises of 2005 Archived 28 December 2008 at the Wayback Machine.
- ↑ The Seoul Peace Prize Cultural Foundation Archived 29 August 2013 at Archive.is
- 1 2 3 4 5 6 Bortolotti, Dan (2004). Hope in Hell: Inside the World of Doctors Without Borders, Firefly Books. ISBN 1-55297-865-6.
- ↑ Bortolotti, above, puts the death toll at 10,000. An estimate of 15,000 to 30,000, warning of an inevitable dysentery epidemic, comes from: Camilo, V (1974). "The Earthquake in Managua". The Lancet (Correspondence). 303 (7845): 25–26.
- ↑ MSF Article Chronologies: Années 70 (French) MSF-France. Retrieved 10 January 2006.
- ↑ MSF Article (1999) Cambodia's second chance MSF. Retrieved 10 January 2006.
- ↑ MSF Article (2005) MSF's principles and identity – The challenges ahead MSF. Retrieved 10 January 2006.
- ↑ Richard Seymour, The Liberal Defense of Murder (London 2008), p. 174.
- ↑ "Dr. Bernard Kouchner and MSF: A Clarification, 22 May 2007". Doctorswithoutborders.org. Retrieved 3 October 2011.
- ↑ Information obtained from the various sections' websites.
- ↑ Denis Kennedy, "Humanitarian NGOs and the Norm of Neutrality: A Community Approach"
- ↑ Davey, Eleanor (2011). "Famine, aid, and ideology: the political activism of Médecins sans frontières in the 1980s". French Historical Studies. 34 (3): 529–58. doi:10.1215/00161071-1259157.
- ↑ MSF Article Chronologie: Années 80 (French) MSF-France. Retrieved 10 January 2006.
- ↑ "'Gamalive European Speedster Assembly'".
- 1 2 3 4 5 6 MSF Article (2009) -MSF in SUDAN – TEST MSF Retrieved 20 September 2011
- ↑ MSF Article (2010) – Sudan: An Overview of MSF's Work in 2010 MSF Retrieved 20 September 2011.
- ↑ "Kala-azar Epidemiology and Control, Southern Sudan". wwwnc.cdc.gov. Retrieved 7 August 2014.
- ↑ MSF Press release (2010) – Southern Sudan in Grips of Worst Disease Outbreak in Eight YearsMSF Retrieved 20 September 2011
- ↑ MSF Article (2010) – Médecins Sans Frontières South Sudan MSF Retrieved 20 September 2011
- ↑ MSF Article (2010) – Sudan: MSF to Open Additional Kala Azar Treatment Site in Upper Nile State MSF Retrieved 20 September 2011
- 1 2 MSF Article (2010) -Sudan: MSF Opens a Kala Azar Treatment Center in Eastern Atbara Region MSF Retrieved 20 September 2011
- 1 2 3 MSF Article (2011) -MSF condemns large-scale attacks on civilians in South Sudan MSF Retrieved 20 September 2011
- ↑ MSF Article Chronologie: Années 90 (French) MSF-France. Retrieved 11 January 2006.
- ↑ MSF Article (2004) Liberia: War ends, but the crisis continues Archived 30 September 2007 at the Wayback Machine. MSF. Retrieved 11 January 2006.
- ↑ Choo V (1993). "Forensic evidence of Iraqi atrocities against Kurds". The Lancet. 341 (8840): 299–300. doi:10.1016/0140-6736(93)92641-6.
- ↑ MSF Article (2005) Somalia – Saving lives in an abandoned land MSF. Retrieved 11 January 2006.
- ↑ MSF Article (2000) Srebrenica five years on MSF. Retrieved 11 January 2006. Archived 2 December 2008 at the Wayback Machine.
- ↑ Forsythe DP (2005). International humanitarianism in the contemporary world: forms and issues, Human Rights and Human Welfare Working Papers "Source" (PDF). (257 KB)
- ↑ One cannot stop a genocide with doctors (French) Archived 10 December 2006 at the Wayback Machine. MSF-France. Retrieved 7 January 2006.
- ↑ Forsythe DP (1996). The International Committee of the Red Cross and humanitarian assistance – A policy analysis, International Review of the Red Cross (314): 512–531.
- ↑ "Code of Conduct for the ICRC Movement and NGOs in Disaster Relief: List of signatories" (PDF). ICRC. Retrieved 7 January 2006.
- ↑ Principles of Conduct for The ICRC Movement and NGOs in Disaster Response Programmes ICRC. Retrieved 7 January 2006.
- ↑ Médecins Sans Frontières (James Orbinski) – Nobel Lecture Nobelprize.org. Retrieved 7 January 2006.
- ↑ MSF Article (1998) MSF 1998 Archived 27 September 2007 at the Wayback Machine. MSF. Retrieved 16 January 2006.
- ↑ MSF Article (2000) Preventing meningitis Archived 30 September 2007 at the Wayback Machine. MSF. Retrieved 16 January 2006.
- ↑ MSF Article (1998) MSF and other aid organisations evicted from Kabul MSF. Retrieved 16 January 2006.
- ↑ MSF Article (1998) Attacks as told by victims MSF. Retrieved 16 January 2006.
- ↑ MSF Article (2001) Controlling phantom limb pain in Sierra Leone MSF. Retrieved 16 January 2006.
- ↑ MSF Article (2000) Kosovo: The physical and psychological consequences of war MSF. Retrieved 12 January 2006.
- ↑ Urbinski, James. (2008) An Imperfect Offering: Humanitarian Action in the 21st Century, Doubleday Canada. ISBN 978-0-385-66069-3.
- ↑ Solidaire – NATO used military operations data and assessments in Kosovo obtained by Medecins sans Frontieres (MSF)
- ↑ MSF Article (2002) No end in sight to the war in Chechnya MSF. Retrieved 12 January 2006.
- ↑ MSF Article (2005) Haiti: Working amid intensifying violence MSF. Retrieved 15 January 2006.
- ↑ Canadian Press Doctors Without Borders loses all three hospitals in Haitian quakeCP. Retrieved January 2010.,
- ↑ RT: Doctors Without Borders: Haiti Aid Planes refused landings. 19 January 2010
- ↑ MSF Article (2005) India: Bringing medical care MSF. Retrieved 15 January 2006.
- ↑ MSF Article (2005) Post-tsunami mental health: 'We're still weak at the knees' MSF. Retrieved 15 January 2006.
- ↑ Shevchenko, Olga, Fox, Renée. ""Nationals" and "expatriates": Challenges of fulfilling "sans frontières" ("without borders") ideals in international humanitarian action". www.hhrjournal.org. Retrieved 17 August 2009.
- 1 2 WHO (2004) Introduction Archived 10 January 2006 at the Wayback Machine.. AIDS epidemic update: December 2004. Retrieved 12 January 2006.
- ↑ WHO article 2010 Antiretroviral therapy MSF. Retrieved 15 January 2006.
- ↑ MSF Article (2005) Nothing new in Ituri: The violence continues Archived 16 February 2006 at the Wayback Machine. MSF. Retrieved 15 January 2006.
- ↑ MSF Article (2004) The tragedy of the other Congo – A forgotten war's victims MSF. Retrieved 12 January 2006.
- ↑ MSF Article (2000) Democratic Republic of Congo (DRC): Complex emergency, human catastrophe WHO. Retrieved 21 November 2010.
- ↑ MSF Article (2005) Uganda: A neglected emergency MSF. Retrieved 12 January 2006.
- ↑ MSF Article (2004) Uganda: Aiding civilians targeted by war MSF. Retrieved 12 January 2006.
- 1 2 MSF Article (2005) Côte d'Ivoire: Renewed violence deepens crisis Retrieved 21 January 2006.
- ↑ MSF Article (2003) MSF vaccinates thousands against measles in Ivory Coast MSF. Retrieved 15 January 2006.
- ↑ Marc DuBois and Caitlin Wake, with Scarlett Sturridge and Christina Bennett (2015) The Ebola response in West Africa: Exposing the politics and culture of international aid London: Overseas Development Institute
- ↑ "SES JOINS THE CLINTON GLOBAL INITIATIVE (CGI)" (Press release). SES. September 14, 2014. Retrieved January 31, 2016.
- ↑ CDC Article (2010) Counterfeit and Substandard Antimalarial Drugs. Retrieved 21 February 2012.
- ↑ Yeung, S., et al. (2008) Access to artemisinin combination therapy for malaria in remote areas of Cambodia, Malaria Journal. Retrieved 21 February 2012.
- ↑ Yeung, S., et al. (2008) Cost of increasing access to artemisinin combination therapy: the Cambodian experience, Malaria Journal. Retrieved 21 February 2012.
- ↑ MSF Article (2004) AIDS in Cambodia: A Second Chance at Life. Retrieved 21 February 2012.
- ↑ WHO (2007) Offering integrated care for HIV/AIDS, diabetes and hypertension within chronic disease clinics in Cambodia. Retrieved 21 February 2012.
- ↑ WHO Cambodia Disaster Profile (2010). Retrieved 21 February 2012.
- ↑ MSF International Activity Report (2006). Retrieved 21 February 2012.
- ↑ IRIN report (2010) In Brief: TB, HIV warning for Cambodia's prisons. Retrieved 21 February 2012.
- ↑ LICAHDO Press Release (2011) Cambodian Prison Overcrowding Crisis Only Getting Worse. Retrieved 21 February 2012.
- ↑ Janssens, B., et al. (2007) Effectiveness of Highly Active Antiretroviral Therapy in HIV-Positive Children: Evaluation at 12 Months in a Routine Program in Cambodia. Retrieved 21 February 2012.
- ↑ MSF article (2007) Cambodia: Number of dengue cases drop in Takeo; threat remains. Retrieved 21 February 2012.
- ↑ Mail and Guardian News Report (2008) Cambodia: 407 died from dengue fever in 2007. Retrieved 21 February 2012.
- ↑ MSF International Activity Report (2010). Retrieved 21 February 2012.
- ↑ MSF Field News (2011) Cambodia: TB is "One of the Biggest Challenges for Public Health". Retrieved 21 February 2012.
- ↑ Armstrong, JC; Nichols, BE; Wilson, JM; Cosico, RA; Shanks, L (20 March 2014). "Spinal cord injury in the emergency context: review of program outcomes of a spinal cord injury rehabilitation program in Sri Lanka.". Conflict and Health. 8 (1): 4. PMC 3994551
 . PMID 24650231. doi:10.1186/1752-1505-8-4.
. PMID 24650231. doi:10.1186/1752-1505-8-4. - ↑ International Activity Report 2010
- 1 2 https://www.msf.org.uk/article/yemen-staff-and-patients-killed-after-airstrike-hits-abs-hospital
- ↑ https://www.msf.org.uk/country/yemen
- ↑ Field Operations: What Do We Do? Archived 16 March 2006 at the Wayback Machine. MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2003) The Vaccine Gap: NY Times editorial Archived 30 September 2007 at the Wayback Machine. MSF. Retrieved 28 December 2005.
- ↑ MSF Press Release (2003) MSF launches the first large-scale test of an oral vaccine against cholera in the city of Beira, Mozambique MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2004) World AIDS Day MSF country profiles Archived 30 September 2007 at the Wayback Machine. MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2004) Once ill equipped and poorly manned – transforming a hospital in North Darfur MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2001) Tajikistan: Aid to health system in shambles MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2004) Nicaragua: Focusing care on women's health and Chagas disease MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2002) MSF mental health activities: a brief overview Archived 27 September 2007 at the Wayback Machine. MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2000) Preventing malnutrition and famine MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2001) Malnutrition definition and MSF treatment MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2001) MSF Therapeutic Feeding Programmes MSF. Retrieved 28 December 2005.
- ↑ Drugs and Medical Supplies Catalogue Vol. 1 (2005) F-75 Description MSF.
- ↑ Drugs and Medical Supplies Catalogue Vol. 1 (2005) F-100 Description MSF.
- ↑ Drugs and Medical Supplies Catalogue Vol. 1 (2005) Plumpy'nut Description MSF.
- ↑ Drugs and Medical Supplies Catalogue Vol. 1 (2005) BP5 Description MSF.
- ↑ MSF Article (2001) Diarrhoea definition and MSF treatment MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2001) MSF: Water and Health MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2002) Simple water treatment MSF-UAE. Retrieved 28 December 2005.
- ↑ MSF Article (2001) Cholera definition and MSF treatment MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2002) Removal and treatment of wastewater MSF-UAE. Retrieved 28 December 2005.
- ↑ MSF Article (2002) Refuse pit MSF-UAE. Retrieved 28 December 2005.
- ↑ MSF Article (2002) Malnutrition: rates and measures MSF. Retrieved 28 December 2005.
- ↑ MSF Article (2002) Mortality: rates and measures Archived 27 September 2007 at the Wayback Machine. MSF. Retrieved 28 December 2005.
- ↑ WHO Fact Sheet Meningococcal meningitis WHO. Retrieved 28 December 2005.
- ↑ MSF Article Mental health care crucial in emergency situations MSF. Retrieved 28 December 2005.
- ↑ MSF Article A scientific approach to "témoignage" Archived 30 September 2007 at the Wayback Machine. MSF. Retrieved 28 December 2005.
- ↑ Prunier, Gérard (2005). Darfur: The Ambiguous Genocide. Cornell University Press. p. 149. ISBN 0-8014-4450-0.
- ↑ Editorial. "PLoS Medicine: Ethics Without Borders". www.plosmedicine.org. Retrieved 11 August 2009.
- ↑ Rennie, Stuart. "Global bioethics blog: Ethics, research and Medecins sans Frontieres". globalbioethics.blogspot.com. Retrieved 11 August 2009.
- ↑ https://www.theguardian.com/world/2017/feb/27/ngo-rescues-off-libya-encourage-traffickers-eu-borders-chief
- ↑ WHO Health topic Essential Medicines
- ↑ "MSF Urges Novartis to Drop Case Against Indian Government | Doctors Without Borders". Web1.doctorswithoutborders.org. 20 December 2006. Retrieved 3 October 2011.
- ↑ "Novartis loses landmark India cancer drug patent case". Reuters. 1 April 2013. Retrieved 1 April 2013.
- ↑ MSF Article (2004) Military humanitarianism: A deadly confusion Archived 14 May 2006 at the Wayback Machine. MSF. Retrieved 12 January 2006.
- ↑ MSF Article (2004) Independent aid in Iraq virtually impossible MSF. Retrieved 12 January 2006.
- ↑ MSF Article (2004) The real reasons MSF left Afghanistan MSF. Retrieved 12 January 2006.
- ↑ MSF Article (2004) MSF pulls out of Afghanistan MSF. Retrieved 17 January 2006.
- ↑ MSF Press Release. "MSF: Ongoing insecurity in CAR threatens lives of civilians and humanitarians, blocking urgent medical care". www.msf.org. Retrieved 4 August 2009.
- ↑ MSF Press Release. "MSF: MSF is shocked and outraged by attack on our team in Somalia". www.msf.org. Retrieved 4 August 2009.
- ↑ MSF Article (2005) MSF shocked by arrest of Head of Mission in Sudan – charged with crimes against the state MSF. Retrieved 11 January 2006.
- ↑ Karunakara, Unni. "Why MSF decided to leave Somalia". Retrieved 13 November 2013.
- ↑ Christopher Stokes (4 October 2015). "Death toll rises" (Press release). Médecins Sans Frontières.
- ↑ "Airstrikes hit Médecins Sans Frontières hospital in Yemen ". The Guardian. 27 October 2015.
- ↑ "Syria: Barrel bombing of MSF-supported hospital kills seven". Msf.org.uk. Retrieved 2016-07-06.
- ↑ "MSF-supported hospital bombed in Yemen: death toll rises to six". Médecins Sans Frontières. 17 January 2016
- ↑ "Syrian war: Suspected Russian air strikes destroy two hospitals – despite so-called Syria 'ceasefire'". The Independent UK. 15 February 2016
- ↑ "MSF-supported hospital bombed by Russian Air Force in Northern Syria". The UK Guardian. 15 February 2016
- ↑ CBS/AP February 16, 2016, 8:23 AM (2016-02-16). "U.S. and Russia both deny bombing Syrian clinic". Cbsnews.com. Retrieved 2016-07-06.
- ↑ Kareem Shaheen in Beirut; Ian Black (2016-04-28). "Airstrike on MSF-backed Aleppo hospital kills patients and doctors". Theguardian.com. Retrieved 2016-07-06.
- ↑ Abrams, Irwin (2001). The Nobel Peace Prize and the laureates: An illustrated biographical history, 1901–2001. Nantucket, Massachusetts: Science History Publications. pp. 351–352.
- ↑ MSF Article (1999). "The Nobel Peace Prize speech". www.msf.org. MSF. Retrieved 7 October 2013.
- ↑ "2015 Lasker Prize for MSF (in Spanish)". Jornada.unam.mx. 2015-09-08. Retrieved 2016-07-06.
Further reading
- Bortolotti, D (2004). "Hope in Hell: Inside the World of Doctors Without Borders". Firefly Books. Buffalo, N.Y.: Firefly Books. ISBN 1-55297-865-6.
- Greenberg KS (2002). "Humanitarianism in the Post-Colonial Era: The History of Médecins Sans Frontières" (PDF). The Concord Review. (links to PDF file)
- McCall M, Salama P (1 September 1999). "Selection, training, and support of relief workers: an occupational health issue". British Medical Journal. 318 (7176): 113–116. PMC 1114577 . PMID 9880288. doi:10.1136/bmj.318.7176.113.
- Zwi AB (2004). "How Should the Health Community Respond to Violent Political Conflict?". PLoS Medicine (online). 1 (1): e14. PMC 523835 . PMID 15526042. doi:10.1371/journal.pmed.0010014.
- Katz IT, Wright AA (2004). "Collateral Damage – Médecins sans Frontières Leaves Afghanistan and Iraq". The New England Journal of Medicine. 351 (25): 2571–2573. PMID 15602015. doi:10.1056/NEJMp048296. (full text requires registration)
- Olivier Weber, Humanitaires (Félin, 2002)
- Shevchenko O, Fox RC (2008). ""Nationals" and "expatriates": Challenges of fulfilling "sans frontières" ("without borders") ideals in international humanitarian action". Health and Human Rights: an International Journal. 10 (1).
- Olivier Weber, French doctors (Robert Laffont, 1995)
External links
| Wikimedia Commons has media related to Médecins sans frontières. |
- Médecins Sans Frontières International
- Doctors Without Borders:
- Official Nobel Peace Prize page for MSF
- Essentialdrugs.org
- Observatoire de l'action humanitaire
- Drugs for Neglected Diseases Initiative
- The Bernard Kouchner Project – Compassion Without Borders
- MSF Speaking Out Case Studies
1999 Nobel Prize laureates | ||
|---|---|---|
| Chemistry | Ahmed Zewail (Egypt) |  |
| Literature | Günter Grass (Germany) | |
| Peace | Médecins Sans Frontières (Switzerland) | |
| Physics |
| |
| Physiology or Medicine | Günter Blobel (Germany/United States) | |
| Economic Sciences | Robert Mundell (Canada) | |
| ||