Chlorprothixene
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Truxal |
| AHFS/Drugs.com | Micromedex Detailed Consumer Information |
| Routes of administration | Oral, IM |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Metabolism | Hepatic |
| Biological half-life | 8–12 hours |
| Excretion | Feces, urine |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| ECHA InfoCard | 100.003.666 |
| Chemical and physical data | |
| Formula | C18H18ClNS |
| Molar mass | 315.861 g/mol |
| 3D model (JSmol) | |
| |
| |
| (verify) | |
Chlorprothixene (Cloxan, Taractan, Truxal) is a typical antipsychotic drug of the thioxanthene class and was the first of the series to be synthesized.[1] It was introduced in 1959 by Lundbeck.[2]
Chlorprothixene is not approved for use in the United States.
Pharmacology
Chlorprothixene exerts strong antagonism at the following receptors:
- 5-HT2: antipsychotic effects, anxiolysis, weight gain
- D1, D2, D3: antipsychotic effects, sedation, extrapyramidal side effects, prolactin increase, depression, apathy/anhedonia, weight gain
- H1: sedation, weight gain
- mACh: anticholinergic effects, inhibition of extrapyramidal side effects
- α1-adrenergic: hypotension, tachycardia
Chlorprothixene does also act as FIASMA (functional inhibitor of acid sphingomyelinase).[3]
One metabolite of chlorprothixene is N-desmethylchlorprothixene.

Indications
Chlorprothixene's principal indications are the treatment of psychotic disorders (e.g. schizophrenia) and of acute mania occurring as part of bipolar disorders.
Other uses are pre- and postoperative states with anxiety and insomnia, severe nausea / emesis (in hospitalized patients), the amelioration of anxiety and agitation due to use of selective serotonin reuptake inhibitors for depression and, off-label, the amelioration of alcohol and opioid withdrawal. It may also be used cautiously to treat nonpsychotic irritability, aggression, and insomnia in pediatric patients.
An intrinsic antidepressant effect of chlorprothixene has been discussed, but not proven yet. Likewise, it is unclear, if chlorprothixene has genuine (intrinsic) analgesic effects. However, chlorprothixene can be used as comedication in severe chronic pain. Also, like most antipsychotics, chlorprothixene has antiemetic effects.
Side effects
Chlorprothixene has a strong sedative activity with a high incidence of anticholinergic side effects. The types of side effects encountered (dry mouth, massive hypotension and tachycardia, hyperhidrosis, substantial weight gain etc.) normally do not allow a full effective dose for the remission of psychotic disorders to be given. So cotreatment with another, more potent, antipsychotic agent is needed.
Chlorprothixene is structurally related to chlorpromazine, with which it shares, in principle, all side effects. Allergic side effects and liver damage seem to appear with an appreciable lower frequency. The elderly are particularly sensitive to anticholinergic side effects of chlorprothixene (precipitation of narrow angle glaucoma, severe obstipation, difficulties in urinating, confusional and delirant states). In patients >60 years the doses should be particularly low.
Early and late extrapyramidal side effects may occur but have been noted with a low frequency (one study with a great number of participants has delivered a total number of only 1%).
Overdosage
Overdose symptoms can be confusion, hypotension, and tachycardia, and several fatalities have been reported with concentrations in postmortem blood ranging from 0.1 to 7.0 mg/L compared to non-toxic levels in postmortem blood which can extend to 0.4 mg/kg.[4]
Dosage
The initial doses of chlorprothixene should always be as low as possible (e.g. 30 mg at bedtime, 15 mg morning dose) and be increased gradually. Patients receiving 90 mg daily (and more) of the drug should be hospitalized, particularly during the initial phase of treatment. The theoretical maximum is 800 mg daily which can usually not be given due to side effects as stated above. Elderly and pediatric patients should be treated with particular low initial doses. Dose increments should be done slowly. If chlorprothixene is to be withdrawn, it should not be stopped abruptly, but the dose should be decreased steadily.
Interactions
Chlorprothixene may increase the plasma-level of concomitantly given lithium. In order to avoid lithium intoxication, lithium plasma levels should be monitored closely.
If chlorprothixene is given concomitantly with opioids, the opioid dose should be reduced (by approx. 50%), because chlorprothixene amplifies the therapeutic actions and side effects of opioids considerably.
Avoid the concomitant use of chlorprothixene and tramadol (Ultram). Seizures may be encountered with this combination.
Consider additive sedative effects and confusional states to emerge, if chlorprothixene is given with benzodiazepines or barbiturates. Choose particular low doses of these drugs.
Exert particular caution in combining chlorprothixene with other anticholinergic drugs (tricyclic antidepressants and antiparkinsonian agents): Particularly the elderly may develop delirium, high fever, severe obstipation, even ileus and glaucoma .
Synthesis
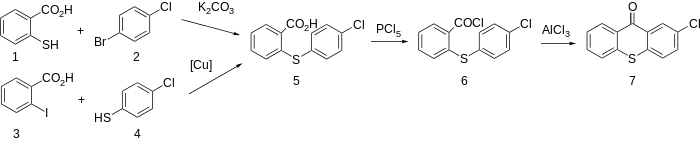
Chlorprothixene (2-chloro-9[(1-dimethylamino)-3-propyliden]thioxanthene) is made starting from 2-Chlorothioxanthone. 2-Chlorothioxantone, in turn, is prepared from 2-mercaptobenzoic acid (1), the reaction of which with 1-bromo-4-chlorobenzene (2) forms 2-(4-chlorophenylthio)benzoic acid 5, which upon reaction with phosphorus pentachloride transforms into acid chloride (6), and further undergoes intramolecular cyclization with the use of aluminum chloride to give 2-chlorthioxantone (6).[5]
An alternative way of making 2-chlorthioxantone (7) is by making 2-(4-chlorophenylthio)benzoic acid (5) by reacting 2-iodobenzoic acid (3) with 4-chlorothiophenol (4).[6]
The resulting 2-chlorothioxantone is reacted as a carbonyl component with either 3-dimethylaminopropylmagnesiumbromide (see Engelhardt above), or with allylmagnesiumbromide, giving the corresponding tertiary alcohols 8, and 9.

Dehydration of the tertiary (8) is accomplished by acylation of the tertiary hydroxyl group using acetyl chloride and the subsequent pyrolysis of the formed acetate, which leads to the desired chlorprothixene. In the second case, dehydration of the tertiary alcohol (9) is accomplished by chlorination of the tertiary alcohol group by thionyl chloride, forming the diene 2-chloro-9-(3-propen-1-iliden)thioxanthene (10), the addition to which of dimethylamine at high temperature forms the desired chlorprothixene (11).
See also
References
- ↑ Healy, David (1997). The antidepressant era. Cambridge: Harvard University Press. p. 182. ISBN 0-674-03958-0.
- ↑ Sneader, Walter (2005). Drug discovery: a history. New York: Wiley. p. 410. ISBN 0-471-89980-1.
- ↑ Kornhuber J, Muehlbacher M, Trapp S, Pechmann S, Friedl A, Reichel M, Mühle C, Terfloth L, Groemer T, Spitzer G, Liedl K, Gulbins E, Tripal P (2011). "Identification of novel functional inhibitors of acid sphingomyelinase". PLoS ONE. 6 (8): e23852. PMC 3166082
 . PMID 21909365. doi:10.1371/journal.pone.0023852.
. PMID 21909365. doi:10.1371/journal.pone.0023852. - ↑ Skov L, Johansen SS, Linnet K (Jan 2015). "Postmortem Femoral Blood Reference Concentrations of Aripiprazole, Chlorprothixene, and Quetiapine". Journal of Analytical Toxicology. 39 (1): 41–44. PMID 25342720. doi:10.1093/jat/bku121.
- ↑ H. Spiegelberg, K. Doeben, DE 1044103 (1957).
- ↑ E.L. Engelhardt, J.M. Sprague, U.S. Patent 2,951,082 (1960).