Oral mucosa
| Oral mucosa | |
|---|---|
| Details | |
| Latin | tunica mucosa oris |
| Dorlands /Elsevier | t_22/12832012 |
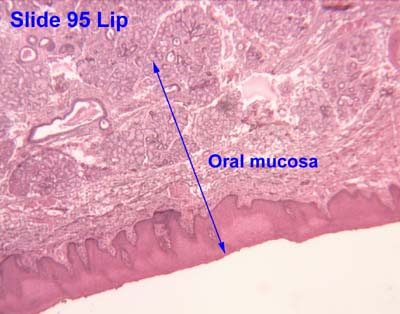
The oral mucosa is the mucous membrane lining the inside of the mouth and consists of stratified squamous epithelium termed oral epithelium and an underlying connective tissue termed lamina propria.[1] The oral cavity has sometimes been described as a mirror that reflects the health of the individual.[2] Changes indicative of disease are seen as alterations in the oral mucosa lining the mouth, which can reveal systemic conditions, such as diabetes or vitamin deficiency, or the local effects of chronic tobacco or alcohol use.[3]
Classification
It can be divided into three main categories based on function and histology:
- Masticatory mucosa, keratinized stratified squamous epithelium, found on the dorsum of the tongue, hard palate and attached gingiva.
- Lining mucosa, nonkeratinized stratified squamous epithelium, found almost everywhere else in the oral cavity, including the:
- Buccal mucosa refers to the inside lining of the cheeks and floor of the mouth and is part of the lining mucosa.
- Labial mucosa refers to the inside lining of the lips and is part of the lining mucosa.
- Alveolar mucosa refers to the lining between the buccal and labial mucosae. It is a brighter red, smooth and shiny with many blood vessels, and is not connected to underlying tissue by rete pegs.[4]
- Specialized mucosa, specifically in the regions of the taste buds on lingual papillae on the dorsal surface of the tongue that contains nerve endings for general sensory reception and taste perception.[5]
Structure

1: Stratum basale
2: Stratum spinosum
3: Stratum granulosum
4: Stratum corneum
Oral mucosa consists of two layers, the surface stratified squamous epithelium and the deeper lamina propria. In keratinized oral mucosa, the epithelium consists of four layers:
- Stratum basale (basal layer)
- Stratum spinosum (prickle layer)
- Stratum granulosum (granular layer)
- Stratum corneum (keratinized layer)
In nonkeratinised epithelium, the two deep layers (basale and spinosum) remain the same but the outer layers are termed the intermediate and superficial layers.
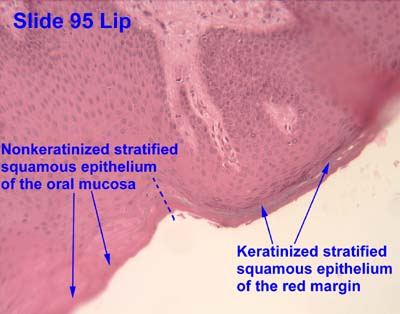
Depending on the region of the mouth, the epithelium may be nonkeratinized or keratinized. Nonkeratinized squamous epithelium covers the soft palate, inner lips, inner cheeks, and the floor of the mouth, and ventral surface of the tongue. Keratinized squamous epithelium is present in the attached gingiva and hard palate as well as areas of the dorsal surface of the tongue.[5][6]
Keratinization is the differentiation of keratinocytes in the stratum granulosum into nonvital surface cells or squames to form the stratum corneum. The cells terminally differentiate as they migrate to the surface from the stratum basale where the progenitor cells are located to the superficial surface.
Unlike keratinized epithelium, nonkeratinized epithelium normally has no superficial layers showing keratinization. Nonkeratinized epithelium may, however, readily transform into a keratinizing type in response to frictional or chemical trauma, in which case it undergoes hyperkeratinization.This change to hyperkeratinization commonly occurs on the usually nonkeratinized buccal mucosa when the linea alba forms, a white ridge of calloused tissue that extends horizontally at the level where the maxillary and mandibular teeth come together and occlude. Histologically, an excess amount of keratin is noted on the surface of the tissue, and the tissue has all the layers of an orthokeratinized tissue with its granular and keratin layers. In patients who have habits such as clenching or grinding (bruxism) their teeth, a larger area of the buccal mucosa than just the linea alba becomes hyperkeratinized. This larger white, rough, raised lesion needs to be recorded so that changes may be made in the dental treatment plan regarding the patient’s parafunctional habits.[7][8]
Even keratinized tissue can undergo further level of hyperkeratinization; an increase in the amount of keratin is produced as a result of chronic physical trauma to the region. Changes such as hyperkeratinization are reversible if the source of the injury is removed, but it takes time for the keratin to be shed or lost by the tissue. Thus, to check for malignant changes, a baseline biopsy and microscopic study of any whitened tissue may be indicated, especially if in a high-risk cancer category, such with a history of tobacco or alcohol use or are HPV positive. Hyperkeratinized tissue is also associated with the heat from smoking or hot fluids on the hard palate in the form of nicotinic stomatitis.[7]
The lamina propria is a fibrous connective tissue layer that consists of a network of type I and III collagen and elastin fibers in some regions. The main cells of the lamina propria are the fibroblasts, which are responsible for the production of the fibers as well as the extracellular matrix.
The lamina propria, like all forms of connective tissue proper, has two layers: papillary and dense. The papillary layer is the more superficial layer of the lamina propria. It consists of loose connective tissue within the connective tissue papillae, along with blood vessels and nerve tissue. The tissue has an equal amount of fibers, cells, and intercellular substance. The dense layer is the deeper layer of the lamina propria. It consists of dense connective tissue with a large amount of fibers. Between the papillary layer and the deeper layers of the lamina propria is a capillary plexus, which provides nutrition for the all layers of the mucosa and sends capillaries into the connective tissue papillae.[7]
A submucosa may or may not be present deep to the dense layer of the lamina propria, depending on the region of the oral cavity. If present, the submucosa usually contains loose connective tissue and may also contain adipose tissue or salivary glands, as well as overlying bone or muscle within the oral cavity.[7]
A variable number of Fordyce spots or granules are scattered throughout the non keratinized tissue. These are a normal variant, visible as small, yellowish bumps on the surface of the mucosa. They correspond to deposits of sebum from misplaced sebaceous glands in the submucosa that are usually associated with hair follicles.[7]
A basal lamina (basement membrane without aid of the microscope) is at the interface between the oral epithelium and lamina propria similar to the epidermis and dermis.[9]
Function
- Protection
- Sensation
- Secretion
- Thermal regulation[9]
See also
- Oral mucosa tissue engineering
- Junctional epithelium
- Oral cancer
- Salivary glands
- Basal lamina
- Fibroblast
References
- ↑ Ten Cate's Oral Histology, Nanci, Elsevier, 2013, page 280
- ↑ Oral Manifestations of Systemic Diseases at eMedicine
- ↑ Squier, Christopher A.; Kremer, Mary J. (2001). "Biology of Oral Mucosa and Esophagus". Journal of the National Cancer Institute. Monographs (29): 7–15. PMID 11694559.
- ↑ Chandra (1 January 2004). Textbook of Dental and Oral Histology and Embryology with MCQs. Jaypee Brothers Publishers. pp. 180–. ISBN 978-81-8061-238-1.
- 1 2 University of Michigan Health System, Learning Resource Center at http://histology.med.umich.edu/node/2
- ↑ Luiz Carlos Junquiera et al (2005), Basic Histology, p. 282, ISBN 0-07-144116-6
- 1 2 3 4 5 Illustrated Dental Embryology, Histology, and Anatomy, Bath-Balogh and Fehrenbach, Elsevier, 2011, page 106
- ↑ Ten Cate's Oral Histology, Nanci, Elsevier, 2013, page 285
- 1 2 Ten Cate's Oral Mucosa, Nanci, Elsevier, 2013, page 278
External links
| Wikimedia Commons has media related to Tunica mucosa oris. |
- Histology image: 09601loa – Histology Learning System at Boston University – "Digestive System: Oral Cavity and Teeth – lip, oral mucosa"
- Histology image: 95_04 at the University of Oklahoma Health Sciences Center – "Lip"
- Histology image: 95_07 at the University of Oklahoma Health Sciences Center – "Lip"
- Common Dental and Oral Mucosal Disorders, Duke University at http://pamodules.mc.duke.edu/Oral_Health/Print.asp?CourseNum=1&LessonNum=3
{kind=link}
{kind=link}