Borderline personality disorder
| Borderline personality disorder | |
|---|---|
| Synonyms | Emotionally unstable personality disorder – impulsive or borderline type,[1] emotional intensity disorder,[2] neurotic psychopathy[1] |
 | |
| Idealization in Edvard Munch’s The Brooch. Eva Mudocci (1903) | |
| Specialty | Psychiatry |
| Symptoms | Unstable relationships, sense of self, and emotions, self harm[3][4] |
| Complications | Suicide[3] |
| Usual onset | Early adulthood[4] |
| Duration | Long term[3] |
| Causes | Unclear[5] |
| Diagnostic method | Based on the symptoms[3] |
| Similar conditions | identity problem, substance use disorders[4] |
| Treatment | Therapy[3] |
| Prognosis | Improves over time[4] |
| Frequency | 1.6%[3] |
| Personality disorders |
|---|
| Cluster A (odd) |
| Cluster B (dramatic) |
| Cluster C (anxious) |
| Not specified |
Borderline personality disorder (BPD), also known as emotionally unstable personality disorder, is a long-term pattern of abnormal behavior characterized by unstable relationships with other people, unstable sense of self, and unstable emotions.[3][4] There is often an extreme fear of abandonment, frequent dangerous behavior, a feeling of emptiness, and self-harm. Symptoms may be brought on by seemingly normal events.[3] The behavior typically begins by early adulthood, and occurs across a variety of situations.[4] Substance abuse, depression, and eating disorders are commonly associated with BPD.[3] BPD increases the risk of self-harm and 10% of people affected die by suicide.[3][4]
BPD's causes are unclear, but seem to involve genetic, brain, environmental, and social factors.[3][5] It occurs about five times more often in a person who has an affected close relative.[3] Adverse life events also appear to play a role. The underlying mechanism appears to involve the frontolimbic network of neurons.[6] BPD is recognized by the Diagnostic and Statistical Manual of Mental Disorders (DSM) as a personality disorder, along with nine other such disorders.[4] Diagnosis is based on the symptoms while a medical exam may be done to rule out other problems.[3] The condition must be differentiated from an identity problem or substance use disorders, among other possibilities.[4]
Borderline personality disorder is typically treated with therapy, such as cognitive behavioral therapy (CBT). Another type, dialectical behavior therapy (DBT) may reduce the risk of suicide. Therapy may occur one-on-one, or in a group. While medications do not cure BPD, they may be used to help with the associated symptoms. Some people require care in hospital.[3]
About 1.6% of people have BPD in a given year.[3] Females are diagnosed about three times as often as males. It appears to become less common among older people. Up to half of people improve over a ten-year period. People affected typically use a high amount of healthcare resources.[4] There is an ongoing debate about the naming of the disorder, especially the suitability of the word "borderline".[3] The disorder is often stigmatized in both the media and psychiatric field.[7]
Signs and symptoms
Borderline personality disorder may be characterized by the following signs and symptoms:
- Markedly disturbed sense of identity
- Frantic efforts to avoid real or imagined abandonment and extreme reactions to such
- Splitting ("black-and-white" thinking)
- Impulsivity and impulsive or dangerous behaviours
- Intense or uncontrollable emotional reactions that often seem disproportionate to the event or situation
- Unstable and chaotic interpersonal relationships
- Self-damaging behavior
- Distorted self-image[3]
- Dissociation
- Frequently accompanied by depression, anxiety, anger, substance abuse, or rage
The most distinguishing symptoms of BPD are marked sensitivity to rejection or criticism, and intense fear of possible abandonment.[8] Overall, the features of BPD include unusually intense sensitivity in relationships with others, difficulty regulating emotions, and impulsivity. Other symptoms may include feeling unsure of one's personal identity, morals, and values; having paranoid thoughts when feeling stressed; dissociation and depersonalization; and, in moderate to severe cases, stress-induced breaks with reality or psychotic episodes.
Emotions
People with BPD may feel emotions with greater ease, depth and for a longer time than others do.[9][10] A core characteristic of BPD is affective instability, which generally manifests as unusually intense emotional responses to environmental triggers, with a slower return to a baseline emotional state.[11][12] People with BPD often engage in idealization and devaluation of others, alternating between high positive regard for people and great disappointment in them.[13] In Marsha Linehan's view, the sensitivity, intensity, and duration with which people with BPD feel emotions have both positive and negative effects.[12] People with BPD are often exceptionally enthusiastic, idealistic, joyful, and loving.[14] However, they may feel overwhelmed by negative emotions ("anxiety, depression, guilt/shame, worry, anger, etc."), experiencing intense grief instead of sadness, shame and humiliation instead of mild embarrassment, rage instead of annoyance, and panic instead of nervousness.[14]
People with BPD are also especially sensitive to feelings of rejection, criticism, isolation, and perceived failure.[15] Before learning other coping mechanisms, their efforts to manage or escape from their very negative emotions may lead to emotional isolation, self-injury or suicidal behavior.[16] They are often aware of the intensity of their negative emotional reactions and, since they cannot regulate them, they shut them down entirely.[12] This can be harmful to people with BPD, since negative emotions alert people to the presence of a problematic situation and move them to address it which the person with BPD would normally be aware of only to cause further distress.[12] People with BPD may feel emotional relief after cutting themselves.[17]
While people with BPD feel euphoria (ephemeral or occasional intense joy), they are especially prone to dysphoria (inability to experience entirety), depression, and/or feelings of mental and emotional distress. Zanarini et al. recognized four categories of dysphoria that are typical of this condition: extreme emotions, destructiveness or self-destructiveness, feeling fragmented or lacking identity, and feelings of victimization.[18] Within these categories, a BPD diagnosis is strongly associated with a combination of three specific states: feeling betrayed, "feeling like hurting myself", and feeling out of control.[18] Since there is great variety in the types of dysphoria experienced by people with BPD, the amplitude of the distress is a helpful indicator of borderline personality disorder.[18] In addition to intense emotions, people with BPD experience emotional "lability"; or in other words, changeability. Although the term emotional lability suggests rapid changes between depression and elation, the mood swings in people with this condition actually fluctuate more frequently between anger and anxiety and between depression and anxiety.[19]
Behavior
Impulsive behavior is common, including substance or alcohol abuse, eating disorders, unprotected sex or indiscriminate sex with multiple partners, reckless spending, and reckless driving.[20] Impulsive behavior may also include leaving jobs or relationships, running away, and self-injury.[21] People with BPD act impulsively because it gives them the feeling of immediate relief from their emotional pain.[21] However, in the long term, people with BPD suffer increased pain from the shame and guilt that follow such actions.[21] A cycle often begins in which people with BPD feel emotional pain, engage in impulsive behavior to relieve that pain, feel shame and guilt over their actions, feel emotional pain from the shame and guilt, and then experience stronger urges to engage in impulsive behavior to relieve the new pain.[21] As time goes on, impulsive behavior may become an automatic response to emotional pain.[21]
Self-harm and suicide

Self-harming or suicidal behavior is one of the core diagnostic criteria in the DSM-5.[4] Self-harm occurs in 50 to 80% of people with BPD. The most frequent method of self-harm is cutting.[22] Bruising, burning, head banging or biting are not uncommon with BPD.[22]
The lifetime risk of suicide among people with BPD is between 3% and 10%.[8][23] There is evidence that men diagnosed with BPD are approximately twice as likely to die by suicide as women diagnosed with BPD.[24] There is also evidence that a considerable percentage of men who die by suicide may have undiagnosed BPD.[25]
The reported reasons for self-harm differ from the reasons for suicide attempts.[16] Nearly 70% of people with BPD self-harm without trying to end their life.[26] Reasons for self-harm include expressing anger, self-punishment, generating normal feelings (often in response to dissociation), and distracting oneself from emotional pain or difficult circumstances.[16] In contrast, suicide attempts typically reflect a belief that others will be better off following the suicide.[16] Both suicide and self-harm are a response to feeling negative emotions.[16] Sexual abuse can be a particular trigger for suicidal behavior in adolescents with BPD tendencies.[27]
Interpersonal relationships
People with BPD can be very sensitive to the way others treat them, by feeling intense joy and gratitude at perceived expressions of kindness, and intense sadness or anger at perceived criticism or hurtfulness.[28] Their feelings about others often shift from admiration or love to anger or dislike after a disappointment, a threat of losing someone, or a perceived loss of esteem in the eyes of someone they value. This phenomenon, sometimes called splitting, includes a shift from idealizing others to devaluing them.[29] Combined with mood disturbances, idealization and devaluation can undermine relationships with family, friends, and co-workers.[30] Self-image can also change rapidly from healthy to unhealthy.
While strongly desiring intimacy, people with BPD tend toward insecure, avoidant or ambivalent, or fearfully preoccupied attachment patterns in relationships,[31] and they often view the world as dangerous and malevolent.[28] BPD, like other personality disorders, is linked to increased levels of chronic stress and conflict in romantic relationships, decreased satisfaction on the part of romantic partners, abuse, and unwanted pregnancy.[32]
Sense of self
People with BPD tend to have trouble seeing a clear picture of their identity. In particular, they tend to have difficulty knowing what they value, believe, prefer, and enjoy.[33] They are often unsure about their long-term goals for relationships and jobs. This difficulty with knowing who they are and what they value can cause people with BPD to experience feeling "empty" and "lost".[33]
Cognitions
The often intense emotions experienced by people with BPD can make it difficult for them to control the focus of their attention—to concentrate.[33] In addition, people with BPD may tend to dissociate, which can be thought of as an intense form of "zoning out".[34] Dissociation often occurs in response to experiencing a painful event (or experiencing something that triggers the memory of a painful event). It involves the mind automatically redirecting attention away from that event, presumably to protect against experiencing intense emotion and unwanted behavioral impulses that such emotion might otherwise trigger.[34] Although the mind's habit of blocking out intense painful emotions may provide temporary relief, it can also have the unwanted side effect of blocking or blunting the experience of ordinary emotions, reducing the access of people with BPD to the information contained in those emotions, which helps guide effective decision-making in daily life.[34] Sometimes, it is possible for another person to tell when someone with BPD is dissociating, because their facial or vocal expressions may become flat or expressionless, or they may appear to be distracted; at other times, dissociation may be barely noticeable.[34]
Disability
BPD is related to lower functioning and disability, even when socioeconomic status, medical conditions, and all psychiatric disorders were controlled.[35] Further, it is more common for females with BPD to experience disabilities than males with BPD.[35] More research is necessary to determine if this is due to a genetic sex difference or social reasons, but more females with BPD are diagnosed than males.[35]
Causes
As is the case with other mental disorders, the causes of BPD are complex and not fully agreed upon.[36] Evidence suggests that BPD and post-traumatic stress disorder (PTSD) may be related in some way.[37] Most researchers agree that a history of childhood trauma can be a contributing factor,[38] but less attention has historically been paid to investigating the causal roles played by congenital brain abnormalities, genetics, neurobiological factors, and environmental factors other than trauma.[36][39]
Social factors include how people interact in their early development with their family, friends, and other children.[40] Psychological factors include the individual's personality and temperament, shaped by their environment and learned coping skills that deal with stress.[40] These different factors together suggest that there are multiple factors that may contribute to the disorder.
Genetics
The heritability of BPD has been estimated at 40%.[41] That is, 40 percent of the variability in liability underlying BPD in the population can be explained by genetic differences. Twin studies may overestimate the effect of genes on variability in personality disorders due to the complicating factor of a shared family environment.[42] Nonetheless, the researchers of this study concluded that personality disorders "seem to be more strongly influenced by genetic effects than almost any axis I disorder [e.g., bipolar disorder, depression, eating disorders], and more than most broad personality dimensions."[43] Moreover, the study found that BPD was estimated to be the third most-heritable personality disorder out of the 10 personality disorders reviewed.[43] Twin, sibling, and other family studies indicate partial heritability for impulsive aggression, but studies of serotonin-related genes have suggested only modest contributions to behavior.[44]
Families with twins in the Netherlands were participants of an ongoing study by Trull and colleagues, in which 711 pairs of siblings and 561 parents were examined to identify the location of genetic traits that influenced the development of BPD.[45] Research collaborators found that genetic material on chromosome nine was linked to BPD features.[45] The researchers concluded that "genetic factors play a major role in individual differences of borderline personality disorder features."[45] These same researchers had earlier concluded in a previous study that 42 percent of variation in BPD features was attributable to genetic influences and 58 percent was attributable to environmental influences.[45] Genes under investigation as of 2012 include the 7-repeat polymorphism of the dopamine D4 receptor (DRD4), which has been linked to disorganized attachment, whilst the combined effect of the 7-repeat polymorphism and the 10/10 dopamine transporter (DAT) genotype has been linked to abnormalities in inhibitory control, both noted features of BPD.[46] There is a possible connection to chromosome 5.[47]
Brain abnormalities
A number of neuroimaging studies in BPD have reported findings of reductions in regions of the brain involved in the regulation of stress responses and emotion, affecting the hippocampus, the orbitofrontal cortex, and the amygdala, amongst other areas.[46] A smaller number of studies have used magnetic resonance spectroscopy to explore changes in the concentrations of neurometabolites in certain brain regions of BPD patients, looking specifically at neurometabolites such as N-acetylaspartate, creatine, glutamate-related compounds, and choline-containing compounds.[46]
Hippocampus
The hippocampus tends to be smaller in people with BPD, as it is in people with post-traumatic stress disorder (PTSD). However, in BPD, unlike PTSD, the amygdala also tends to be smaller.[48]
Amygdala
The amygdalae are smaller and more active in people with BPD.[48] Decreased amygdala volume has also been found in people with obsessive-compulsive disorder.[49] One study has found unusually strong activity in the left amygdalas of people with BPD when they experience and view displays of negative emotions.[50] Since the amygdala generates all emotions (including unpleasant ones), this unusually strong activity may explain the unusual strength and longevity of fear, sadness, anger, and shame experienced by people with BPD, as well as their heightened sensitivity to displays of these emotions in others.[48]
Prefrontal cortex
The prefrontal cortex tends to be less active in people with BPD, especially when recalling memories of abandonment.[51] This relative inactivity occurs in the right anterior cingulate (areas 24 and 32).[51] Given its role in regulating emotional arousal, the relative inactivity of the prefrontal cortex might explain the difficulties people with BPD experience in regulating their emotions and responses to stress.[52]
Hypothalamic-pituitary-adrenal axis
The hypothalamic-pituitary-adrenal axis (HPA axis) regulates cortisol production, which is released in response to stress. Cortisol production tends to be elevated in people with BPD, indicating a hyperactive HPA axis in these individuals.[53] This causes them to experience a greater biological stress response, which might explain their greater vulnerability to irritability.[54] Since traumatic events can increase cortisol production and HPA axis activity, one possibility is that the prevalence of higher than average activity in the HPA axis of people with BPD may simply be a reflection of the higher than average prevalence of traumatic childhood and maturational events among people with BPD.[54] Another possibility is that, by heightening their sensitivity to stressful events, increased cortisol production may predispose those with BPD to experience stressful childhood and maturational events as traumatic.
Increased cortisol production is also associated with an increased risk of suicidal behavior.[55]
Neurobiological factors
Estrogen
Individual differences in women's estrogen cycles may be related to the expression of BPD symptoms in female patients.[56] A 2003 study found that women's BPD symptoms were predicted by changes in estrogen levels throughout their menstrual cycles, an effect that remained significant when the results were controlled for a general increase in negative affect.[57]
Developmental factors
Childhood trauma
There is a strong correlation between child abuse, especially child sexual abuse, and development of BPD.[58][59][60] Many individuals with BPD report a history of abuse and neglect as young children, but causation is still debated.[61] Patients with BPD have been found to be significantly more likely to report having been verbally, emotionally, physically, or sexually abused by caregivers of either gender. They also report a high incidence of incest and loss of caregivers in early childhood.[62] Individuals with BPD were also likely to report having caregivers of both sexes deny the validity of their thoughts and feelings. Caregivers were also reported to have failed to provide needed protection and to have neglected their child's physical care. Parents of both sexes were typically reported to have withdrawn from the child emotionally and to have treated the child inconsistently.[62] Additionally, women with BPD who reported a previous history of neglect by a female caregiver and abuse by a male caregiver were significantly more likely to experience sexual abuse by a non-caregiver.[62]
It has been suggested that children who experience chronic early maltreatment and attachment difficulties may go on to develop borderline personality disorder.[63] Writing in the psychoanalytic tradition, Otto Kernberg argues that a child's failure to achieve the developmental task of psychic clarification of self and other and failure to overcome splitting might increase the risk of developing a borderline personality.[64] A child's inability to tolerate delayed gratification at age four does not predict later development of BPD.[65]
Neurological patterns
The intensity and reactivity of a person's negative affectivity, or tendency to feel negative emotions, predicts BPD symptoms more strongly than does childhood sexual abuse.[66] This finding, differences in brain structure (see Brain abnormalities), and the fact that some patients with BPD do not report a traumatic history,[67] suggest that BPD is distinct from the post-traumatic stress disorder which frequently accompanies it. Thus, researchers examine developmental causes in addition to childhood trauma.
Research published in January 2013 by Dr. Anthony Ruocco at the University of Toronto has highlighted two patterns of brain activity that may underlie the dysregulation of emotion indicated in this disorder: (1) increased activity in the brain circuits responsible for the experience of heightened emotional pain, coupled with (2) reduced activation of the brain circuits that normally regulate or suppress these generated painful emotions. These two neural networks are seen to be dysfunctionally operative in the frontolimbic regions, but the specific regions vary widely in individuals, which calls for the analysis of more neuroimaging studies.[68]
Also (contrary to the results of earlier studies) sufferers of BPD showed less activation in the amygdala in situations of increased negative emotionality than the control group. Dr. John Krystal, editor of the journal Biological Psychiatry, wrote that these results "[added] to the impression that people with borderline personality disorder are 'set-up' by their brains to have stormy emotional lives, although not necessarily unhappy or unproductive lives".[68] Their emotional instability has been found to correlate with differences in several brain regions.[69]
Mediating and moderating factors
Executive function
While high rejection sensitivity is associated with stronger symptoms of borderline personality disorder, executive function appears to mediate the relationship between rejection sensitivity and BPD symptoms.[65] That is, a group of cognitive processes that include planning, working memory, attention, and problem-solving might be the mechanism through which rejection sensitivity impacts BPD symptoms. A 2008 study found that the relationship between a person's rejection sensitivity and BPD symptoms was stronger when executive function was lower and that the relationship was weaker when executive function was higher.[65] This suggests that high executive function might help protect people with high rejection sensitivity against symptoms of BPD.[65] A 2012 study found that problems in working memory might contribute to greater impulsivity in people with BPD.[70]
Family environment
Family environment mediates the effect of child sexual abuse on the development of BPD. An unstable family environment predicts the development of the disorder, while a stable family environment predicts a lower risk. One possible explanation is that a stable environment buffers against its development.[71]
Self-complexity
Self-complexity, or considering one's self to have many different characteristics, appears to moderate the relationship between Actual-Ideal self-discrepancy issues and the development of BPD symptoms. That is, for individuals who believe that their actual characteristics do not match the characteristics that they hope to acquire, high self-complexity reduces the impact of their conflicted self-image on BPD symptoms.[72] However, self-complexity does not moderate the relationship between Actual-Ought self-discrepancy and the development of BPD symptoms. That is, for individuals who believe that their actual characteristics do not match the characteristics that they should already have, high self-complexity does not reduce the impact of their conflicted self-image on BPD symptoms. The protective role of self-complexity in Actual-Ideal self-discrepancy, but not in Actual-Ought self-discrepancy, suggests that the impact of conflicted or unstable self-image in BPD depends on whether the individual views himself or herself in terms of characteristics that they hope to acquire, or in terms of characteristics that they should already have acquired.[72]
Thought suppression
A 2005 study found that thought suppression, or conscious attempts to avoid thinking certain thoughts, mediates the relationship between emotional vulnerability and BPD symptoms.[66] A later study found that the relationship between emotional vulnerability and BPD symptoms is not necessarily mediated by thought suppression. However, this study did find that thought suppression mediates the relationship between an invalidating environment and BPD symptoms.[73]
Diagnosis
Diagnosis of borderline personality disorder is based on a clinical assessment by a mental health professional. The best method is to present the criteria of the disorder to a person and to ask them if they feel that these characteristics accurately describe them.[8] Actively involving people with BPD in determining their diagnosis can help them become more willing to accept it.[8] Although some clinicians prefer not to tell people with BPD what their diagnosis is, either from concern about the stigma attached to this condition or because BPD used to be considered untreatable, it is usually helpful for the person with BPD to know their diagnosis.[8] This helps them know that others have had similar experiences and can point them toward effective treatments.[8]
In general, the psychological evaluation includes asking the patient about the beginning and severity of symptoms, as well as other questions about how symptoms impact the patient's quality of life. Issues of particular note are suicidal ideations, experiences with self-harm, and thoughts about harming others.[74] Diagnosis is based both on the person's report of their symptoms and on the clinician's own observations.[74] Additional tests for BPD can include a physical exam and laboratory tests to rule out other possible triggers for symptoms, such as thyroid conditions or substance abuse.[74] The ICD-10 manual refers to the disorder as emotionally unstable personality disorder and has similar diagnostic criteria. In the DSM-5, the name of the disorder remains the same as in the previous editions.[4]
Diagnostic and Statistical Manual
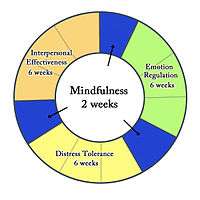
The Diagnostic and Statistical Manual of Mental Disorders fifth edition (DSM-5) has removed the multiaxial system. Consequently, all disorders, including personality disorders, are listed in Section II of the manual. A person must meet 5 of 9 criteria to receive a diagnosis of borderline personality disorder.[75] The DSM-5 defines the main features of BPD as a pervasive pattern of instability in interpersonal relationships, self image, and affect, as well as markedly impulsive behavior.[75] In addition, the DSM-5 proposes alternative diagnostic criteria for Borderline personality disorder in section III, "Alternative DSM-5 Model for Personality Disorders." These alternative criteria are based on trait research and include specifying at least four of seven maladaptive traits.[76] According to Marsha Linehan, many mental health professionals find it challenging to diagnose BPD using the DSM criteria, since these criteria describe such a wide variety of behaviors.[77] To address this issue, Linehan has grouped the symptoms of BPD under five main areas of dysregulation: emotions, behavior, interpersonal relationships, sense of self, and cognition.[77]
International Classification of Disease
The World Health Organization's ICD-10 defines a disorder that is conceptually similar to borderline personality disorder, called (F60.3) Emotionally unstable personality disorder. Its two subtypes are described below.[78]
- F60.30 Impulsive type
At least three of the following must be present, one of which must be (2):
- marked tendency to act unexpectedly and without consideration of the consequences;
- marked tendency to engage in quarrelsome behavior and to have conflicts with others, especially when impulsive acts are thwarted or criticized;
- liability to outbursts of anger or violence, with inability to control the resulting behavioral explosions;
- difficulty in maintaining any course of action that offers no immediate reward;
- unstable and capricious (impulsive, whimsical) mood.
- F60.31 Borderline type
At least three of the symptoms mentioned in F60.30 Impulsive type must be present [see above], with at least two of the following in addition:
- disturbances in and uncertainty about self-image, aims, and internal preferences;
- liability to become involved in intense and unstable relationships, often leading to emotional crisis;
- excessive efforts to avoid abandonment;
- recurrent threats or acts of self-harm;
- chronic feelings of emptiness.
- demonstrates impulsive behavior, e.g., speeding in a car or substance abuse[79]
The ICD-10 also describes some general criteria that define what is considered a personality disorder.
Millon's subtypes
Theodore Millon has proposed four subtypes of BPD. He suggests that an individual diagnosed with BPD may exhibit none, one, or more of the following:[80]
| Subtype | Features |
|---|---|
| Discouraged (including avoidant or dependent personality features) | Pliant, submissive, loyal, humble; feels vulnerable and in constant jeopardy; feels hopeless, depressed, helpless, and powerless. |
| Petulant (including negativistic features) | Negativistic, impatient, restless, as well as stubborn, defiant, sullen, pessimistic, and resentful; easily feels "slighted" and quickly disillusioned. |
| Impulsive (including histrionic or antisocial features) | Capricious, superficial, flighty, distractible, frenetic, and seductive; fearing loss, the individual becomes agitated; gloomy and irritable; and potentially suicidal. |
| Self-destructive (including depressive or masochistic and self-defeating features) | Inward-turning, intropunitively (self-punishing) angry; conforming, deferential, and ingratiating behaviors have deteriorated; increasingly high-strung and moody; possible suicide. |
Misdiagnosis
People with BPD may be misdiagnosed for a variety of reasons. One reason for misdiagnosis is BPD has symptoms that coexist (comorbidity) with other disorders such as depression, PTSD, and bipolar disorder.[81][82]
Family members
People with BPD are prone to feeling angry at members of their family and alienated from them. On their part, family members often feel angry and helpless at how their BPD family members relate to them.[8] Parents of adults with BPD are often both over-involved and under-involved in family interactions.[83] In romantic relationships, BPD is linked to increased levels of chronic stress and conflict, decreased satisfaction of romantic partners, abuse, and unwanted pregnancy. However, these links may apply to personality disorders in general.[32]
Adolescence
Onset of symptoms typically occurs during adolescence or young adulthood, although symptoms suggestive of this disorder can sometimes be observed in children.[84] Symptoms among adolescents that predict the development of BPD in adulthood may include problems with body-image, extreme sensitivity to rejection, behavioral problems, non-suicidal self-injury, attempts to find exclusive relationships, and severe shame.[8] Many adolescents experience these symptoms without going on to develop BPD, but those who experience them are 9 times as likely as their peers to develop BPD. They are also more likely to develop other forms of long-term social disabilities.[8] Clinicians are discouraged from diagnosing anyone with BPD before the age of 18, due to the normal ups and downs of adolescence and a still-developing personality. However, BPD can sometimes be diagnosed before age 18, in which case the features must have been present and consistent for at least one year.[85]
A BPD diagnosis in adolescence might predict that the disorder will continue into adulthood.[85][86] Among adolescents who warrant a BPD diagnosis, there appears to be one group in which the disorder remains stable over time and another group in which the individuals move in and out of the diagnosis.[87] Earlier diagnoses may be helpful in creating a more effective treatment plan for the adolescent.[85][86] Family therapy is considered a helpful component of treatment for adolescents with BPD.[88]
Differential diagnosis and comorbidity
Lifetime comorbid (co-occurring) conditions are common in BPD. Compared to those diagnosed with other personality disorders, people with BPD showed a higher rate of also meeting criteria for[89]
- mood disorders, including major depression and bipolar disorder
- anxiety disorders, including panic disorder, social anxiety disorder, and post-traumatic stress disorder (PTSD)
- other personality disorders
- substance abuse
- eating disorders, including anorexia nervosa and bulimia
- attention deficit hyperactivity disorder[90]
- somatic symptom disorder (formerly known as a somatoform disorder, this is a category of mental disorder included in a number of diagnostic schemes of mental illness)
- dissociative disorders
A diagnosis of a personality disorder should not be made during an untreated mood episode/disorder, unless the lifetime history supports the presence of a personality disorder.
Comorbid Axis I disorders
| Axis I diagnosis | Overall (%) | Male (%) | Female (%) |
|---|---|---|---|
| Mood disorders | 75.0 | 68.7 | 80.2 |
| Major depressive disorder | 32.1 | 27.2 | 36.1 |
| Dysthymia | 9.7 | 7.1 | 11.9 |
| Bipolar I disorder | 31.8 | 30.6 | 32.7 |
| Bipolar II disorder | 7.7 | 6.7 | 8.5 |
| Anxiety disorders | 74.2 | 66.1 | 81.1 |
| Panic disorder with agoraphobia | 11.5 | 7.7 | 14.6 |
| Panic disorder without agoraphobia | 18.8 | 16.2 | 20.9 |
| Social phobia | 29.3 | 25.2 | 32.7 |
| Specific phobia | 37.5 | 26.6 | 46.6 |
| PTSD | 39.2 | 29.5 | 47.2 |
| Generalized anxiety disorder | 35.1 | 27.3 | 41.6 |
| Obsessive-compulsive disorder** | 15.6 | --- | --- |
| Substance use disorders | 72.9 | 80.9 | 66.2 |
| Any alcohol use disorder | 57.3 | 71.2 | 45.6 |
| Any drug use disorder | 36.2 | 44.0 | 29.8 |
| Eating disorders** | 53.0 | 20.5 | 62.2 |
| Anorexia nervosa** | 20.8 | 7 * | 25 * |
| Bulimia nervosa** | 25.6 | 10 * | 30 * |
| Eating disorder not otherwise specified** | 26.1 | 10.8 | 30.4 |
| Somatoform disorders** | 10.3 | 10 * | 10 * |
| Somatization disorder** | 4.2 | --- | --- |
| Hypochondriasis** | 4.7 | --- | --- |
| Somatoform pain disorder** | 4.2 | --- | --- |
| Psychotic disorders** | 1.3 | 1 * | 1 * |
| * Approximate values ** Values from 1998 study[89] --- Value not provided by study | |||
A 2008 study found that at some point in their lives, 75 percent of people with BPD meet criteria for mood disorders, especially major depression and Bipolar I, and nearly 75 percent meet criteria for an anxiety disorder.[91] Nearly 73 percent meet criteria for substance abuse or dependency, and about 40 percent for PTSD.[91] It is noteworthy that less than half of the participants with BPD in this study presented with PTSD, a prevalence similar to that reported in an earlier study.[89] The finding that less than half of patients with BPD experience PTSD during their lives challenges the theory that BPD and PTSD are the same disorder.[89]
There are marked gender differences in the types of comorbid conditions a person with BPD is likely to have—[89] a higher percentage of males with BPD meet criteria for substance-use disorders, while a higher percentage of females with BPD meet criteria for PTSD and eating disorders.[89][91][92] In one study, 38% of participants with BPD met the criteria for a diagnosis of ADHD.[90] In another study, 6 of 41 participants (15%) met the criteria for an autism spectrum disorder (a subgroup that had significantly more frequent suicide attempts).[93]
Regardless that it is an infradiagnosed disorder, a few studies have shown that the "lower expressions" of it might lead to wrong diagnoses. The many and shifting Axis I disorders in people with BPD can sometimes cause clinicians to miss the presence of the underlying personality disorder. However, since a complex pattern of Axis I diagnoses has been found to strongly predict the presence of BPD, clinicians can use the feature of a complex pattern of comorbidity as a clue that BPD might be present.[89]
Mood disorders
Many people with borderline personality disorder also have mood disorders, such as major depressive disorder or a bipolar disorder.[30] Some characteristics of BPD are similar to those of mood disorders, which can complicate the diagnosis.[94][95][96] It is especially common for people to be misdiagnosed with bipolar disorder when they have borderline personality disorder or vice versa.[97] For someone with bipolar disorder, behavior suggestive of BPD might appear while the client is experiencing an episode of major depression or mania, only to disappear once the client's mood has stabilized.[98] For this reason, it is ideal to wait until the client's mood has stabilized before attempting to make a diagnosis.[98]
At face value, the affective lability of BPD and the rapid mood cycling of bipolar disorders can seem very similar.[99] It can be difficult even for experienced clinicians, if they are unfamiliar with BPD, to differentiate between the mood swings of these two conditions.[100] However, there are some clear differences.[97]
First, the mood swings of BPD and bipolar disorder tend to have different durations. In some people with bipolar disorder, episodes of depression or mania last for at least two weeks at a time, which is much longer than moods last in people with BPD.[97] Even among those who experience bipolar disorder with more rapid mood shifts, their moods usually last for days, while the moods of people with BPD can change in minutes or hours.[100] So while euphoria and impulsivity in someone with BPD might resemble a manic episode, the experience would be too brief to qualify as a manic episode.[98][100]
Second, the moods of bipolar disorder do not respond to changes in the environment, while the moods of BPD do respond to changes in the environment.[98] That is, a positive event would not lift the depressed mood caused by bipolar disorder, but a positive event would potentially lift the depressed mood of someone with BPD. Similarly, an undesirable event would not dampen the euphoria caused by bipolar disorder, but an undesirable event would dampen the euphoria of someone with borderline personality disorder.[98]
Third, when people with BPD experience euphoria, it is usually without the racing thoughts and decreased need for sleep that are typical of hypomania,[98] though a later 2013 study of data collected in 2004 found that borderline personality disorder diagnosis and symptoms were associated with chronic sleep disturbances, including difficulty initiating sleep, difficulty maintaining sleep, and waking earlier than desired, as well as with the consequences of poor sleep, and noted that "[f]ew studies have examined the experience of chronic sleep disturbances in those with borderline personality disorder".[101]
Because the two conditions have a number of similar symptoms, BPD was once considered to be a mild form of bipolar disorder[102][103] or to exist on the bipolar spectrum. However, this would require that the underlying mechanism causing these symptoms be the same for both conditions. Differences in phenomenology, family history, longitudinal course, and responses to treatment indicate that this is not the case.[104] Researchers have found "only a modest association" between bipolar disorder and borderline personality disorder, with "a strong spectrum relationship with [BPD and] bipolar disorder extremely unlikely."[105] Benazzi et al. suggest that the DSM-IV BPD diagnosis combines two unrelated characteristics: an affective instability dimension related to Bipolar II and an impulsivity dimension not related to Bipolar II.[106]
Premenstrual dysphoric disorder
Premenstrual dysphoric disorder (PMDD) occurs in 3–8 percent of women.[107] Symptoms begin 5–11 days before menstruation and cease a few days after it begins. Symptoms may include marked mood swings, irritability, depressed mood, feeling hopeless or suicidal, a subjective sense of being overwhelmed or out of control, anxiety, binge eating, difficulty concentrating, and substantial impairment of interpersonal relationships.[108][109] People with PMDD typically begin to experience symptoms in their early twenties, although many do not seek treatment until their early thirties.[108]
Although some of the symptoms of PMDD and BPD are similar, they are different disorders. They are distinguishable by the timing and duration of symptoms, which are markedly different: the symptoms of PMDD occur only during the luteal phase of the menstrual cycle,[108] whereas BPD symptoms occur persistently at all stages of the menstrual cycle. In addition, the symptoms of PMDD do not include impulsivity.[108]
Comorbid Axis II disorders
| Axis II diagnosis | Overall (% ) | Male (% ) | Female (% ) |
|---|---|---|---|
| Any Cluster A | 50.4 | 49.5 | 51.1 |
| Paranoid | 21.3 | 16.5 | 25.4 |
| Schizoid | 12.4 | 11.1 | 13.5 |
| Schizotypal | 36.7 | 38.9 | 34.9 |
| Any Other Cluster B | 49.2 | 57.8 | 42.1 |
| Antisocial | 13.7 | 19.4 | _9.0 |
| Histrionic | 10.3 | 10.3 | 10.3 |
| Narcissistic | 38.9 | 47.0 | 32.2 |
| Any Cluster C | 29.9 | 27.0 | 32.3 |
| Avoidant | 13.4 | 10.8 | 15.6 |
| Dependent | _3.1 | _2.6 | _3.5 |
| Obsessive-compulsive | 22.7 | 21.7 | 23.6 |
More than two-thirds of people diagnosed with BPD also meet the criteria for another Axis II personality disorder at some point in their lives. (In a 2008 study, the rate was 73.9 percent.)[91] Cluster A disorders, which include paranoid, schizoid, and schizotypal, are the most common, with a prevalence of 50.4 percent in people with BPD.[91]
The second most common is another Cluster B disorder, which includes antisocial, histrionic, and narcissistic. These have an overall prevalence of 49.2 percent in people with BPD, with narcissistic being the most common, at 38.9 percent; antisocial the second most common, at 13.7 percent; and histrionic the least common, at 10.3 percent.[91] The least common are Cluster C disorders, which include avoidant, dependent, and obsessive-compulsive, and have a prevalence of 29.9 percent in people with BPD.[91] The percentages for specific comorbid Axis II disorders can be found in the adjacent table.
Management
Psychotherapy is the primary treatment for borderline personality disorder.[6] Treatments should be based on the needs of the individual, rather than upon the general diagnosis of BPD. Medications are useful for treating comorbid disorders, such as depression and anxiety.[110] Short-term hospitalization has not been found to be more effective than community care for improving outcomes or long-term prevention of suicidal behavior in those with BPD.[111]
Psychotherapy
Long-term psychotherapy is currently the treatment of choice for BPD.[112] While psychotherapy, in particular dialectical behavior therapy and psychodynamic approaches, are effective, the effects are small.[113]
More rigorous treatments are not substantially better than less rigorous treatments.[114] There are six such treatments available: dynamic deconstructive psychotherapy (DDP),[115] mentalization-based treatment (MBT), transference-focused psychotherapy, dialectical behavior therapy (DBT), general psychiatric management, and schema-focused therapy.[8] While DBT is the therapy that has been studied the most,[116] all these treatments appear effective for treating BPD, except for schema-focused therapy.[8] Long-term therapy of any kind, including schema-focused therapy, is better than no treatment, especially in reducing urges to self-injure.[112]
Cognitive behavioral therapy (CBT) is also a type of psychotherapy used for treatment of BPD. This type of therapy relies on changing people's behaviors and beliefs by identifying problems from the disorder. CBT is known to reduce some anxiety and mood symptoms as well as reduce suicidal thoughts and self-harming behaviors.[3]
Mentalization-based therapy and transference-focused psychotherapy are based on psychodynamic principles, and dialectical behavior therapy is based on cognitive-behavioral principles and mindfulness.[112] General psychiatric management combines the core principles from each of these treatments, and it is considered easier to learn and less intensive.[8] Randomized controlled trials have shown that DBT and MBT may be the most effective, and the two share many similarities.[117][118] Researchers are interested in developing shorter versions of these therapies to increase accessibility, to relieve the financial burden on patients, and to relieve the resource burden on treatment providers.[112][118]
From a psychodynamic perspective, a special problem of psychotherapy with people with BPD is intense projection. It requires the psychotherapist to be flexible in considering negative attributions by the patient rather than quickly interpreting the projection.[119]
Some research indicates that mindfulness meditation may bring about favorable structural changes in the brain, including changes in brain structures that are associated with BPD.[120][121][122] Mindfulness-based interventions also appear to bring about an improvement in symptoms characteristic of BPD, and some clients who underwent mindfulness-based treatment no longer met a minimum of five of the DSM-IV-TR diagnostic criteria for BPD.[122][123]
Medications
A 2010 review by the Cochrane collaboration found that no medications show promise for "the core BPD symptoms of chronic feelings of emptiness, identity disturbance and abandonment". However, the authors found that some medications may impact isolated symptoms associated with BPD or the symptoms of comorbid conditions.[124] A 2017 review examined evidence published since the 2010 Cochrane review and found that "evidence of effectiveness of medication for BPD remains very mixed and is still highly compromised by suboptimal study design".[125]
Of the typical antipsychotics studied in relation to BPD, haloperidol may reduce anger and flupenthixol may reduce the likelihood of suicidal behavior. Among the atypical antipsychotics, one trial found that aripiprazole may reduce interpersonal problems and impulsivity.[124] Olanzapine may decrease affective instability, anger, psychotic paranoid symptoms, and anxiety, but a placebo had a greater ameliorative impact on suicidal ideation than olanzapine did. The effect of ziprasidone was not significant.[124][125]
Of the mood stabilizers studied, valproate semisodium may ameliorate depression, interpersonal problems, and anger. Lamotrigine may reduce impulsivity and anger; topiramate may ameliorate interpersonal problems, impulsivity, anxiety, anger, and general psychiatric pathology. The effect of carbamazepine was not significant. Of the antidepressants, amitriptyline may reduce depression, but mianserin, fluoxetine, fluvoxamine, and phenelzine sulfate showed no effect. Omega-3 fatty acid may ameliorate suicidality and improve depression. As of 2017, trials with these medications had not been replicated and the effect of long-term use had not been assessed.[124][125]
Because of weak evidence and the potential for serious side effects from some of these medications, the UK National Institute for Health and Clinical Excellence (NICE) 2009 clinical guideline for the treatment and management of BPD recommends, "Drug treatment should not be used specifically for borderline personality disorder or for the individual symptoms or behavior associated with the disorder." However, "drug treatment may be considered in the overall treatment of comorbid conditions". They suggest a "review of the treatment of people with borderline personality disorder who do not have a diagnosed comorbid mental or physical illness and who are currently being prescribed drugs, with the aim of reducing and stopping unnecessary drug treatment".[126]
Services
There is a significant difference between the number of those who would benefit from treatment and the number of those who are treated. The so-called "treatment gap" is a function of the disinclination of the afflicted to submit for treatment, an underdiagnosing of the disorder by healthcare providers, and the limited availability and access to state-of-the-art treatments.[127] Nonetheless, individuals with BPD accounted for about 20 percent of psychiatric hospitalizations in one survey.[128] The majority of individuals with BPD who are in treatment continue to use outpatient treatment in a sustained manner for several years, but the number using the more restrictive and costly forms of treatment, such as inpatient admission, declines with time.[129]
Experience of services varies.[130] Assessing suicide risk can be a challenge for clinicians, and patients themselves tend to underestimate the lethality of self-injurious behaviors. People with BPD typically have a chronically elevated risk of suicide much above that of the general population and a history of multiple attempts when in crisis.[131] Approximately half the individuals who commit suicide meet criteria for a personality disorder. Borderline personality disorder remains the most commonly associated personality disorder with suicide.[132]
Prognosis
With treatment, the majority of people with BPD can find relief from distressing symptoms and achieve remission, defined as a consistent relief from symptoms for at least two years.[133][134] This longitudinal study tracking the symptoms of people with BPD found that 34.5% achieved remission within two years from the beginning of the study. Within four years, 49.4% had achieved remission, and within six years, 68.6% had achieved remission. By the end of the study, 73.5% of participants were found to be in remission.[133] Moreover, of those who achieved recovery from symptoms, only 5.9% experienced recurrences. A later study found that ten years from baseline (during a hospitalization), 86% of patients had sustained a stable recovery from symptoms.[135]
Patient personality can play an important role during the therapeutic process, leading to better clinical outcomes. Recent research has shown that BPD patients undergoing dialectical behavior therapy (DBT) exhibit better clinical outcomes correlated with higher levels of the trait of agreeableness in the patient, compared to patients either low in agreeableness or not being treated with DBT. This association was mediated through the strength of a working alliance between patient and therapist; that is, more agreeable patients developed stronger working alliances with their therapists, which in turn, led to better clinical outcomes.[136]
In addition to recovering from distressing symptoms, people with BPD also achieve high levels of psychosocial functioning. A longitudinal study tracking the social and work abilities of participants with BPD found that six years after diagnosis, 56% of participants had good function in work and social environments, compared to 26% of participants when they were first diagnosed. Vocational achievement was generally more limited, even compared to those with other personality disorders. However, those whose symptoms had remitted were significantly more likely to have good relationships with a romantic partner and at least one parent, good performance at work and school, a sustained work and school history, and good psychosocial functioning overall.[137]
Epidemiology
The prevalence of BPD was initially estimated to be 1 to 2 percent of the general population[134][138] and to occur three times more often in women than in men.[139][140] However, the lifetime prevalence of BPD in a 2008 study was found to be 5.9% of the general population, occurring in 5.6% of men and 6.2% of women.[91] The difference in rates between men and women in this study was not found to be statistically significant.[91]
Borderline personality disorder is estimated to contribute to 20 percent of psychiatric hospitalizations and to occur among 10 percent of outpatients.[141]
29.5 percent of new inmates in the U.S. state of Iowa fit a diagnosis of borderline personality disorder in 2007,[142] and the overall prevalence of BPD in the U.S. prison population is thought to be 17 percent.[141] These high numbers may be related to the high frequency of substance abuse and substance use disorders among people with BPD, which is estimated at 38 percent.[141]
History

The coexistence of intense, divergent moods within an individual was recognized by Homer, Hippocrates, and Aretaeus, the latter describing the vacillating presence of impulsive anger, melancholia, and mania within a single person. The concept was revived by Swiss physician Théophile Bonet in 1684 who, using the term folie maniaco-mélancolique,[146] described the phenomenon of unstable moods that followed an unpredictable course. Other writers noted the same pattern, including the American psychiatrist Charles H. Hughes in 1884 and J.C. Rosse in 1890, who called the disorder "borderline insanity".[147] In 1921, Kraepelin identified an "excitable personality" that closely parallels the borderline features outlined in the current concept of BPD.[148]
The first significant psychoanalytic work to use the term "borderline" was written by Adolf Stern in 1938.[149] It described a group of patients suffering from what he thought to be a mild form of schizophrenia, on the borderline between neurosis and psychosis.
The 1960s and 1970s saw a shift from thinking of the condition as borderline schizophrenia to thinking of it as a borderline affective disorder (mood disorder), on the fringes of bipolar disorder, cyclothymia, and dysthymia. In the DSM-II, stressing the intensity and variability of moods, it was called cyclothymic personality (affective personality).[85] While the term "borderline" was evolving to refer to a distinct category of disorder, psychoanalysts such as Otto Kernberg were using it to refer to a broad spectrum of issues, describing an intermediate level of personality organization[148] between neurosis and psychosis.[150]
After standardized criteria were developed[151] to distinguish it from mood disorders and other Axis I disorders, BPD became a personality disorder diagnosis in 1980 with the publication of the DSM-III.[134] The diagnosis was distinguished from sub-syndromal schizophrenia, which was termed "Schizotypal personality disorder".[150] The DSM-IV Axis II Work Group of the American Psychiatric Association finally decided on the name "borderline personality disorder," which is still in use by the DSM-5 today.[4] However, the term "borderline" has been described as uniquely inadequate for describing the symptoms characteristic of this disorder.[152]
Controversies
Credibility and validity of testimony
The credibility of individuals with personality disorders has been questioned at least since the 1960s.[153] Two concerns are the incidence of dissociation episodes among people with BPD and the belief that lying is a key component of this condition.
Dissociation
Researchers disagree about whether dissociation, or a sense of detachment from emotions and physical experiences, impacts the ability of people with BPD to recall the specifics of past events. A 1999 study reported that the specificity of autobiographical memory was decreased in BPD patients.[154] The researchers found that decreased ability to recall specifics was correlated with patients' levels of dissociation.[154]
Lying as a feature
Some theorists argue that patients with BPD often lie.[155] However, others write that they have rarely seen lying among patients with BPD in clinical practice.[155] Regardless, lying is not one of the diagnostic criteria for BPD.
The belief that lying is a distinguishing characteristic of BPD can impact the quality of care that people with this diagnosis receive in the legal and healthcare systems. For instance, Jean Goodwin relates an anecdote of a patient with multiple personality disorder, now called dissociative identity disorder, who suffered from pelvic pain due to traumatic events in her childhood.[156] Due to their disbelief in her accounts of these events, physicians diagnosed her with borderline personality disorder, reflecting a belief that lying is a key feature of BPD. Based upon her BPD diagnosis, the physicians then disregarded the patient's assertion that she was allergic to adhesive tape. The patient was in fact allergic to adhesive tape, which later caused complications in the surgery to relieve her pelvic pain.[156]
Gender
Since BPD can be a stigmatizing diagnosis even within the mental health community, some survivors of childhood abuse who are diagnosed with BPD are re-traumatized by the negative responses they receive from healthcare providers.[157] One camp argues that it would be better to diagnose these men or women with post-traumatic stress disorder, as this would acknowledge the impact of abuse on their behavior. Critics of the PTSD diagnosis argue that it medicalizes abuse rather than addressing the root causes in society.[158] Regardless, a diagnosis of PTSD does not encompass all aspects of the disorder (see Brain abnormalities and Terminology).
Joel Paris states that "In the clinic ... Up to 80% of patients are women. That may not be true in the community."[159] He offers the following explanations regarding these gender discrepancies:
"The most probable explanation for gender differences in clinical samples is that women are more likely to develop the kind of symptoms that bring patients in for treatment. Twice as many women as men in the community suffer from depression (Weissman & Klerman, 1985). In contrast, there is a preponderance of men meeting criteria for substance abuse and psychopathy (Robins & Regier, 1991), and males with these disorders do not necessarily present in the mental health system. Men and women with similar psychological problems may express distress differently. Men tend to drink more and carry out more crimes. Women tend to turn their anger on themselves, leading to depression as well as the cutting and overdosing that characterize BPD. Thus, anti-social personality disorder (ASPD) and borderline personality disorders might derive from similar underlying pathology but present with symptoms strongly influenced by gender (Paris, 1997a; Looper & Paris, 2000). We have even more specific evidence that men with BPD may not seek help. In a study of completed suicides among people aged 18 to 35 years (Lesage et al., 1994), 30% of the suicides involved individuals with BPD (as confirmed by psychological autopsy, in which symptoms were assessed by interviews with family members). Most of the suicide completers were men, and very few were in treatment. Similar findings emerged from a later study conducted by our own research group (McGirr, Paris, Lesage, Renaud, & Turecki, 2007)."[25]
In short, men are less likely to seek or accept appropriate treatment, more likely to be treated for symptoms of BPD such as substance abuse rather than BPD itself (furthermore, the symptoms of BPD and ASPD may derive from a similar underlying aetiology) and possibly men are simply more likely to commit suicide prior to diagnosis.
Among men diagnosed with BPD there is also evidence of a higher suicide rate: "men are more than twice as likely as women—18 percent versus 8 percent"—to die by suicide.[24]
There are also sex differences in borderline personality disorders.[160] Men with BPD are more likely to abuse substances, have explosive temper, high levels of novelty seeking and have anti-social, narcissistic, passive-aggressive or sadistic personality traits.[160] Women with BPD are more likely to have eating disorders, mood disorders, anxiety and post-traumatic stress.[160]
Manipulative behavior
Manipulative behavior to obtain nurturance is considered by the DSM-IV-TR and many mental health professionals to be a defining characteristic of borderline personality disorder.[161] However, Marsha Linehan notes that doing so relies upon the assumption that people with BPD who communicate intense pain, or who engage in self-harm and suicidal behavior, do so with the intention of influencing the behavior of others.[162] The impact of such behavior on others—often an intense emotional reaction in concerned friends, family members, and therapists—is thus assumed to have been the person's intention.[162]
However, since people with BPD lack the ability to successfully manage painful emotions and interpersonal challenges, their frequent expressions of intense pain, self-harming, or suicidal behavior may instead represent a method of mood regulation or an escape mechanism from situations that feel unbearable.[163] Linehan notes that if, for example, one were to withhold pain medication from burn victims and cancer patients, leaving them unable to regulate their severe pain, they would also exhibit "attention-seeking" and self-destructive behavior in order to cope.[164]
Stigma
The features of BPD include emotional instability; intense, unstable interpersonal relationships; a need for intimacy; and a fear of rejection. As a result, people with BPD often evoke intense emotions in those around them. Pejorative terms to describe people with BPD, such as "difficult", "treatment resistant", "manipulative", "demanding", and "attention seeking", are often used and may become a self-fulfilling prophecy, as the negative treatment of these individuals triggers further self-destructive behavior.[165]
Physical violence
The stigma surrounding borderline personality disorder includes the belief that people with BPD are prone to violence toward others.[166] While movies and visual media often sensationalize people with BPD by portraying them as violent, the majority of researchers agree that people with BPD are unlikely to physically harm others.[166] Although people with BPD often struggle with experiences of intense anger, a defining characteristic of BPD is that they direct it inward toward themselves.[167] One of the key differences between BPD and antisocial personality disorder (ASPD) is that people with BPD tend to internalize anger by hurting themselves, while people with ASPD tend to externalize it by hurting others.[167]
In addition, adults with BPD have often experienced abuse in childhood, so many people with BPD adopt a "no-tolerance" policy toward expressions of anger of any kind.[167] Their extreme aversion to violence can cause many people with BPD to overcompensate and experience difficulties being assertive and expressing their needs.[167] This is one way in which people with BPD choose to harm themselves over potentially causing harm to others.[167] Another way in which people with BPD avoid expressing their anger through violence is by causing physical damage to themselves, such as engaging in non-suicidal self-injury.[16][166]
Mental healthcare providers
People with BPD are considered to be among the most challenging groups of patients to work with in therapy, requiring a high level of skill and training in the psychiatrists, therapists and nurses involved in their treatment.[168] A majority of psychiatric staff report finding individuals with BPD moderately to extremely difficult to work with and more difficult than other client groups.[169] Efforts are ongoing to improve public and staff attitudes toward people with BPD.[170][171]
In psychoanalytic theory, the stigmatization among mental healthcare providers may be thought to reflect countertransference (when a therapist projects his or her own feelings on to a client). Thus, a diagnosis of BPD "often says more about the clinician's negative reaction to the patient than it does about the patient" and "explains away the breakdown in empathy between the therapist and the patient and becomes an institutional epithet in the guise of pseudoscientific jargon".[150] This inadvertent countertransference can give rise to inappropriate clinical responses, including excessive use of medication, inappropriate mothering, and punitive use of limit setting and interpretation.[172]
Some clients feel the diagnosis is helpful, allowing them to understand that they are not alone and to connect with others with BPD who have developed helpful coping mechanisms. However, others experience the term "borderline personality disorder" as a pejorative label rather than an informative diagnosis. They report concerns that their self-destructive behavior is incorrectly perceived as manipulative and that the stigma surrounding this disorder limits their access to healthcare.[173] Indeed, mental health professionals frequently refuse to provide services to those who have received a BPD diagnosis.[174]
Terminology
Because of the above concerns, and because of a move away from the original theoretical basis for the term (see history), there is ongoing debate about renaming borderline personality disorder. While some clinicians agree with the current name, others argue that it should be changed,[175] since many who are labelled with borderline personality disorder find the name unhelpful, stigmatizing, or inaccurate.[175][176] Valerie Porr, president of Treatment and Research Advancement Association for Personality Disorders states that "the name BPD is confusing, imparts no relevant or descriptive information, and reinforces existing stigma."[177]
Alternative suggestions for names include emotional regulation disorder or emotional dysregulation disorder. Impulse disorder and interpersonal regulatory disorder are other valid alternatives, according to John G. Gunderson of McLean Hospital in the United States.[178] Another term suggested by psychiatrist Carolyn Quadrio is post traumatic personality disorganization (PTPD), reflecting the condition's status as (often) both a form of chronic post traumatic stress disorder (PTSD) as well as a personality disorder.[60] However, although many with BPD do have traumatic histories, some do not report any kind of traumatic event, which suggests that BPD is not necessarily a trauma spectrum disorder.[67]
The Treatment and Research Advancements National Association for Personality Disorders (TARA-APD) campaigned unsuccessfully to change the name and designation of BPD in DSM-5, published in May 2013, in which the name "borderline personality disorder" remains unchanged and it is not considered a trauma- and stressor-related disorder.[179]
Society and culture
Film and television
Films and television shows have portrayed characters either explicitly diagnosed or with traits suggestive of BPD. These may be misleading if they are thought to depict this disorder accurately. Unfortunately, dramatic portrayals of people with BPD in movies and other forms of visual media contribute to the stigma surrounding borderline personality disorder, especially the myth that people with BPD are violent toward others.[166] The majority of researchers agree that in reality, people with BPD are very unlikely to harm others.[166]
The films Play Misty for Me[180] and Girl, Interrupted (based on the memoir of the same name) both suggest the emotional instability of the disorder; however, the first case shows a person more aggressive to others than to herself, which is not characteristic of the disorder.[181] The 1992 film Single White Female, like the first example, also suggests characteristics, some of which are actually atypical of the disorder: the character Hedy had markedly disturbed sense of identity and reacts drastically to abandonment.[182] In a review of the 2011 film Shame for the British journal The Art of Psychiatry, another psychiatrist, Abby Seltzer, praises Carey Mulligan's portrayal of a character with the disorder even though it is never mentioned onscreen.[183]
Films attempting to depict characters with the disorder include A Thin Line Between Love and Hate, Filth, Fatal Attraction, The Crush, Mad Love, Malicious, Interiors, The Cable Guy, Mr. Nobody, Moksha, Cracks,[184] and Welcome to Me.[185][186] Psychiatrists Eric Bui and Rachel Rodgers argue that the character of Anakin Skywalker/Darth Vader in the Star Wars films meets six of the nine diagnostic criteria; Bui also found Anakin a useful example to explain BPD to medical students. In particular, Bui points to the character's abandonment issues, uncertainty over his identity, and dissociative episodes.[187]
Awareness
In early 2008, the United States House of Representatives declared the month of May as Borderline Personality Disorder Awareness Month.[188][189]
Notes
- 1 2 Maj, Mario (2005). Personality disorders. Chichester: J. Wiley & Sons. p. 126. ISBN 9780470090367.
- ↑ Blom, Jan Dirk (2010). A dictionary of hallucinations (1 ed.). New York: Springer. p. 74. ISBN 9781441912237.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 "Borderline Personality Disorder". NIMH. Retrieved 16 March 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Diagnostic and statistical manual of mental disorders : DSM-5 (5th ed.). Washington [etc.]: American Psychiatric Publishing. 2013. pp. 645, 663–6. ISBN 9780890425558.
- 1 2 Clinical Practice Guideline for the Management of Borderline Personality Disorder. Melbourne: National Health and Medical Research Council. 2013. pp. 40–41. ISBN 1864965649.
In addition to the evidence identified by the systematic review, the Committee also considered a recent narrative review of studies that have evaluated biological and environmental factors as potential risk factors for BPD (including prospective studies of children and adolescents, and studies of young people with BPD)
- 1 2 Leichsenring, F; Leibing, E; Kruse, J; New, AS; Leweke, F (1 January 2011). "Borderline personality disorder.". Lancet. 377 (9759): 74–84. PMID 21195251. doi:10.1016/s0140-6736(10)61422-5.
- ↑ Aviram, RB; Brodsky, BS; Stanley, B (2006). "Borderline personality disorder, stigma, and treatment implications.". Harvard Review of Psychiatry. 14 (5): 249–56. PMID 16990170. doi:10.1080/10673220600975121.
- 1 2 3 4 5 6 7 8 9 10 11 12 Gunderson, John G. (26 May 2011). "Borderline Personality Disorder". The New England Journal of Medicine. 364 (21): 2037–2042. PMID 21612472. doi:10.1056/NEJMcp1007358.
- ↑ Linehan 1993, p. 43
- ↑ Manning 2011, p. 36
- ↑ Hooley, Jill; Butcher, James; Nock, Matthew; Mineka, Susan (2017). Abnormal Psychology (17th ed.). Pearson Education, Inc. p. 359. ISBN 9780133852059.
- 1 2 3 4 Linehan 1993, p. 45
- ↑ Linehan 1993, p. 146
- 1 2 Linehan 1993, p. 44
- ↑ Stiglmayr CE, Grathwol T, Linehan MM, Ihorst G, Fahrenberg J, Bohus M (May 2005). "Aversive tension in patients with borderline personality disorder: a computer-based controlled field study". Acta Psychiatr Scand. 111 (5): 372–9. PMID 15819731. doi:10.1111/j.1600-0447.2004.00466.x.
- 1 2 3 4 5 6 Brown MZ, Comtois KA, Linehan MM (February 2002). "Reasons for suicide attempts and nonsuicidal self-injury in women with borderline personality disorder". J Abnorm Psychol. 111 (1): 198–202. PMID 11866174. doi:10.1037/0021-843X.111.1.198.
- ↑ Ducasse, Déborah; Courtet, Philippe; Olié, Emilie (2014). "Physical and Social Pains in Borderline Disorder and Neuroanatomical Correlates: A Systematic Review". Current Psychiatry Reports. 16 (5): 443. PMID 24633938. doi:10.1007/s11920-014-0443-2.
- 1 2 3 Zanarini MC, Frankenburg FR, DeLuca CJ, Hennen J, Khera GS, Gunderson JG (1998). "The pain of being borderline: dysphoric states specific to borderline personality disorder". Harv Rev Psychiatry. 6 (4): 201–7. PMID 10370445. doi:10.3109/10673229809000330.
- ↑ Koenigsberg HW, Harvey PD, Mitropoulou V, et al. (May 2002). "Characterizing affective instability in borderline personality disorder". Am J Psychiatry. 159 (5): 784–8. PMID 11986132. doi:10.1176/appi.ajp.159.5.784.
- ↑ National Education Alliance for Borderline Personality Disorder. "A BPD Brief" (PDF). p. 4. Archived from the original (PDF) on 12 September 2012. Retrieved 30 June 2013.
- 1 2 3 4 5 Manning 2011, p. 18
- 1 2 Oumaya, M; Friedman, S; Pham, A; Abou Abdallah, T; Guelfi, JD; Rouillon, F (October 2008). "[Borderline personality disorder, self-mutilation and suicide: literature review].". L'Encephale. 34 (5): 452–8. PMID 19068333. doi:10.1016/j.encep.2007.10.007.
- ↑ Gunderson, John G.; Links, Paul S. (2008). Borderline Personality Disorder: A Clinical Guide (2nd ed.). American Psychiatric Publishing, Inc. p. 9. ISBN 978-1585623358.
- 1 2 Kreisman J, Strauss H (2004). Sometimes I Act Crazy. Living With Borderline Personality Disorder. Wiley & Sons. p. 206.
- 1 2 Paris J (2008). Treatment of Borderline Personality Disorder. A Guide to Evidence-Based Practice. The Guilford Press. pp. 21–22.
- ↑ Urnes, O (30 April 2009). "[Self-harm and personality disorders].". Tidsskrift for den Norske laegeforening : tidsskrift for praktisk medicin, ny raekke. 129 (9): 872–6. PMID 19415088. doi:10.4045/tidsskr.08.0140.
- ↑ Horesh N, Sever J, Apter A (July–August 2003). "A comparison of life events between suicidal adolescents with major depression and borderline personality disorder". Compr Psychiatry. 44 (4): 277–83. PMID 12923705. doi:10.1016/S0010-440X(03)00091-9.
- 1 2 Arntz, Arnoud (September 2005). "Introduction to special issue: cognition and emotion in borderline personality disorder". Journal of Behavior Therapy and Experimental Psychiatry. 36 (3): 167–72. PMID 16018875. doi:10.1016/j.jbtep.2005.06.001.
- ↑ "What Is BPD: Symptoms". Archived from the original on 10 February 2013. Retrieved 31 January 2013.
- 1 2 Robinson, David J. (2005). Disordered Personalities. Rapid Psychler Press. pp. 255–310. ISBN 1-894328-09-4.
- ↑ Levy KN, Meehan KB, Weber M, Reynoso J, Clarkin JF (2005). "Attachment and borderline personality disorder: implications for psychotherapy". Psychopathology. 38 (2): 64–74. PMID 15802944. doi:10.1159/000084813.
- 1 2 Daley SE, Burge D, Hammen C (August 2000). "Borderline personality disorder symptoms as predictors of 4-year romantic relationship dysfunction in young women: addressing issues of specificity". J Abnorm Psychol. 109 (3): 451–60. PMID 11016115. doi:10.1037/0021-843X.109.3.451.
- 1 2 3 Manning 2011, p. 23
- 1 2 3 4 Manning 2011, p. 24
- 1 2 3 Grant, Chou, Goldstein, Huang, Stinson, Saha, Smith, Dawson, Pulay, Pickering, Ruan (April 2008). "Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: Results from the Wave 2 National Epidemiologic survey on alcohol and related conditions". Journal of Clinical Psychology (69): 533–545.
- 1 2 "Borderline personality disorder". Mayo Clinic. Retrieved 15 May 2008.
- ↑ Gunderson, JG; Sabo, AN (1993). "The phenomenological and conceptual interface between borderline personality disorder and PTSD". Am J Psychiatry. 150 (1): 19–27. PMID 8417576. doi:10.1176/ajp.150.1.19.
- ↑ Kluft, Richard P. (1990). Incest-Related Syndromes of Adult Psychopathology. American Psychiatric Pub, Inc. pp. 83, 89. ISBN 0-88048-160-9.
- ↑ Zanarini, MC; Frankenburg, FR (1997). "Pathways to the development of borderline personality disorder". J. Pers. Disord. 11 (1): 93–104. PMID 9113824. doi:10.1521/pedi.1997.11.1.93.
- 1 2 Grohol, John M. (30 January 2013). "Borderline Personality Disorder". psychcentral.com.
- ↑ Amad, A; Ramoz, N; Thomas, P; Jardri, R; Gorwood, P (March 2014). "Genetics of borderline personality disorder: systematic review and proposal of an integrative model.". Neuroscience and biobehavioral reviews. 40: 6–19. PMID 24456942. doi:10.1016/j.neubiorev.2014.01.003.
- ↑ Torgersen, S (March 2000). "Genetics of patients with borderline personality disorder". Psychiatr. Clin. North Am. 23 (1): 1–9. PMID 10729927. doi:10.1016/S0193-953X(05)70139-8.
- 1 2 Torgersen, S; Lygren, S; Oien, PA; et al. (2000). "A twin study of personality disorders". Compr Psychiatry. 41 (6): 416–25. PMID 11086146. doi:10.1053/comp.2000.16560.
- ↑ Goodman, M; New, A; Siever, L (December 2004). "Trauma, genes, and the neurobiology of personality disorders". Annals of the New York Academy of Sciences. 1032: 104–16. Bibcode:2004NYASA1032..104G. PMID 15677398. doi:10.1196/annals.1314.008.
- 1 2 3 4 "Possible Genetic Causes Of Borderline Personality Disorder Identified". sciencedaily.com. 20 December 2008.
- 1 2 3 O'Neil, Aisling; Thomas Frodl (18 January 2012). "Brain structure and function in borderline personality disorder". Brain Structure and Function. 217: 767–782. doi:10.1007/s00429-012-0379-4. Retrieved 6 May 2014.
- ↑ Lubke, GH; Laurin, C; Amin, N; Hottenga, JJ; Willemsen, G; van Grootheest, G; Abdellaoui, A; Karssen, LC; Oostra, BA; van Duijn, CM; Penninx, BW; Boomsma, DI (August 2014). "Genome-wide analyses of borderline personality features.". Molecular Psychiatry. 19 (8): 923–9. PMC 3872258
 . PMID 23979607. doi:10.1038/mp.2013.109.
. PMID 23979607. doi:10.1038/mp.2013.109. - 1 2 3 Chapman & Gratz 2007, p. 47
- ↑ Szeszko PR, Robinson D, Alvir JM, et al. (October 1999). "Orbital frontal and amygdala volume reductions in obsessive-compulsive disorder". Arch. Gen. Psychiatry. 56 (10): 913–9. PMID 10530633. doi:10.1001/archpsyc.56.10.913.
- ↑ Herpertz SC, Dietrich TM, Wenning B, et al. (August 2001). "Evidence of abnormal amygdala functioning in borderline personality disorder: a functional MRI study". Biol. Psychiatry. 50 (4): 292–8. PMID 11522264. doi:10.1016/S0006-3223(01)01075-7.
- 1 2 Schmahl CG, Elzinga BM, Vermetten E, Sanislow C, McGlashan TH, Bremner JD (July 2003). "Neural correlates of memories of abandonment in women with and without borderline personality disorder". Biol. Psychiatry. 54 (2): 142–51. PMID 12873804. doi:10.1016/S0006-3223(02)01720-1.
- ↑ Chapman & Gratz 2007, p. 48
- ↑ Grossman R, Yehuda R, Siever L (June 1997). "The dexamethasone suppression test and glucocorticoid receptors in borderline personality disorder". Annals of the New York Academy of Sciences. 821: 459–64. Bibcode:1997NYASA.821..459G. PMID 9238229. doi:10.1111/j.1749-6632.1997.tb48305.x.
- 1 2 Chapman & Gratz 2007, p. 49
- ↑ van Heeringen K, Audenaert K, Van de Wiele L, Verstraete A (November 2000). "Cortisol in violent suicidal behaviour: association with personality and monoaminergic activity". J Affect Disord. 60 (3): 181–9. PMID 11074106. doi:10.1016/S0165-0327(99)00180-9.
- ↑ DeSoto, M. Catherine (2007). "Borderline Personality Disorder, Gender and Serotonin: Does Estrogen Play a Role?". In Czerbska, Martina T. Psychoneuroendocrinology Research Trends. Nova Biomedical. Nova Science Publishers. pp. 149–60. ISBN 978-1-60021-665-7.
- ↑ DeSoto MC, Geary DC, Hoard MK, Sheldon MS, Cooper L (August 2003). "Estrogen fluctuations, oral contraceptives and borderline personality". Psychoneuroendocrinology. 28 (6): 751–66. PMID 12812862. doi:10.1016/S0306-4530(02)00068-9.
- ↑ Cohen P (September 2008). "Child development and personality disorder". Psychiatr Clin North Am. 31 (3): 477–93. PMID 18638647. doi:10.1016/j.psc.2008.03.005.
- ↑ Herman, Judith Lewis; Judith Herman MD (1992). Trauma and recovery. New York: BasicBooks. ISBN 0-465-08730-2.
- 1 2 Quadrio, C (December 2005). "Axis One/Axis Two: A disordered borderline". Australian and New Zealand Journal of Psychiatry. 39: A107. doi:10.1111/j.1440-1614.2005.01674_39_s1.x.
- ↑ Ball JS, Links PS (February 2009). "Borderline personality disorder and childhood trauma: evidence for a causal relationship". Curr Psychiatry Rep. 11 (1): 63–8. PMID 19187711. doi:10.1007/s11920-009-0010-4.
- 1 2 3 Zanarini MC, Frankenburg FR, Reich DB, et al. (2000). "Biparental failure in the childhood experiences of borderline patients". J Personal Disord. 14 (3): 264–73. PMID 11019749. doi:10.1521/pedi.2000.14.3.264.
- ↑ Dozier, Mary; Stovall-McClough, K. Chase; Albus, Kathleen E. (1999). "Attachment and psychopathology in adulthood". In Cassidy, Jude; Shaver, Phillip R. Handbook of attachment. New York: Guilford Press. pp. 497–519.
- ↑ Kernberg, Otto F. Borderline conditions and pathological narcissism. Northvale, N.J.: J. Aronson. ISBN 0-87668-762-1.
- 1 2 3 4 Ayduk O, Zayas V, Downey G, Cole AB, Shoda Y, Mischel W (February 2008). "Rejection Sensitivity and Executive Control: Joint predictors of Borderline Personality features". J Res Pers. 42 (1): 151–168. PMC 2390893 . PMID 18496604. doi:10.1016/j.jrp.2007.04.002.
- 1 2 Rosenthal, MZ; Cheavens, JS; Lejuez, CW; Lynch, TR (September 2005). "Thought suppression mediates the relationship between negative affect and borderline personality disorder symptoms". Behav Res There. 43 (9): 1173–85. PMID 16005704. doi:10.1016/j.brat.2004.08.006.
- 1 2 Chapman & Gratz 2007, p. 52
- 1 2 Ruocco, Anthony C.; Amirthavasagam, Sathya, Choi-Kain, Lois W.; McMain, Shelley F. (2013). "Neural Correlates of Negative Emotionality in Borderline Personality Disorder: An Activation-Likelihood-Estimation Meta-Analysis". Biological Psychiatry. 73 (2): 153–160. PMID 22906520. doi:10.1016/j.biopsych.2012.07.014.
- ↑ Koenigsberg, Harold W; Siever, Larry J; Lee, Hedok; Pizzarello, Scott; New, Antonia S; Goodman, Marianne; Cheng, Hu; Flory, Janine; Prohovnik, Isak (2009). "Neural correlates of emotion processing in borderline personality disorder.". Psychiatry Research. 172 (3): 192–9. PMC 4153735 . PMID 19394205. doi:10.1016/j.pscychresns.2008.07.010. Lay summary.
BPD patients demonstrated greater differences in activation than controls, when viewing negative pictures compared with rest, in the amygdala, fusiform gyrus, primary visual areas, superior temporal gyrus (STG), and premotor areas, while healthy controls showed greater differences than BPD patients in the insula, middle temporal gyrus and dorsolateral prefrontal cortex.
- ↑ Lazzaretti, Matteo; Morandotti, Niccolò; Sala, Michela; Isola, Miriam; Frangou, Sophia; De Vidovich, Giulia; Marraffini, Elisa; Gambini, Francesca; et al. (2012). "Impaired working memory and normal sustained attention in borderline personality disorder". Acta Neuropsychiatrica. 24 (6): 349–55. doi:10.1111/j.1601-5215.2011.00630.x.
- ↑ Bradley R, Jenei J, Westen D (January 2005). "Etiology of borderline personality disorder: disentangling the contributions of intercorrelated antedents". J. Nerv. Ment. Dis. 193 (1): 24–31. PMID 15674131. doi:10.1097/01.nmd.0000149215.88020.7c.
- 1 2 Parker, AG; Boldero, JM; Bell, RC (September 2006). "Borderline personality disorder features: the role of self-discrepancies and self-complexity". Psychol Psychother. 79 (Pt 3): 309–21. PMID 16945194. doi:10.1348/147608305X70072.
- ↑ Sauer, SE; Baer, Ruth A.; Baer, RA (February 2009). "Relationships between thought suppression and symptoms of borderline personality disorder". J. Pers. Disord. 23 (1): 48–61. PMID 19267661. doi:10.1521/pedi.2009.23.1.48.
- 1 2 3 "Personality Disorders: Tests and Diagnosis". Mayo Clinic. Retrieved 13 June 2013.
- 1 2 American Psychiatric Association 2013, pp. 663–8
- ↑ American Psychiatric Association 2013, pp. 766–7
- 1 2 Manning 2011, p. 13
- ↑ Emotionally unstable personality disorder – International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) – World Health Organization
- ↑ Carlson, Neil R.; Heth, C. Donald (2010). Psychology: The Science of Behavior. Pearson Canada. p. 570.
- ↑ Millon, Theodore (2004). Personality Disorders in Modern Life. Hoboken, New Jersey: John Wiley & Sons. p. 4. ISBN 0-471-23734-5.
- ↑ Chanen, Andrew M; Thompson, Katherine N (1 April 2016). "Prescribing and borderline personality disorder". Australian Prescriber. 39 (2): 49–53. PMC 4917638 . PMID 27340322. doi:10.18773/austprescr.2016.019.
- ↑ Meaney, Rebecca; Hasking, Penelope; Reupert, Andrea (2016). "Borderline Personality Disorder Symptoms in College Students:The Complex Interplay Between Alexithymia, Emotional Dysregulation and Rumination". PLOS ONE. doi:10.1371/journal.pone.0157294.
- ↑ Allen DM, Farmer RG (1996). "Family relationships of adults with borderline personality disorder". Compr Psychiatry. 37 (1): 43–51. PMID 8770526. doi:10.1016/S0010-440X(96)90050-4.
- ↑ Linehan 1993, p. 49
- 1 2 3 4 American Psychiatric Association 2000
- 1 2 Netherton, S.D.; Holmes, D.; Walker, C.E. (1999). Child and Adolescent Psychological Disorders: Comprehensive Textbook. New York, NY: Oxford University Press.
- ↑ Miller AL, Muehlenkamp JJ, Jacobson CM (July 2008). "Fact or fiction: diagnosing borderline personality disorder in adolescents". Clin Psychol Rev. 28 (6): 969–81. PMID 18358579. doi:10.1016/j.cpr.2008.02.004.
- ↑ Linehan 1993, p. 98
- 1 2 3 4 5 6 7 8 Zanarini MC, Frankenburg FR, Dubo ED, et al. (December 1998). "Axis I comorbidity of borderline personality disorder". Am J Psychiatry. 155 (12): 1733–9. PMID 9842784. doi:10.1176/ajp.155.12.1733.
- 1 2 Ferrer M, Andión O, Matalí J, et al. (December 2010). "Comorbid attention-deficit/hyperactivity disorder in borderline patients defines an impulsive subtype of borderline personality disorder". J. Pers. Disord. 24 (6): 812–22. PMID 21158602. doi:10.1521/pedi.2010.24.6.812.
- 1 2 3 4 5 6 7 8 9 10 11 Grant BF, Chou SP, Goldstein RB, et al. (April 2008). "Prevalence, correlates, disability, and comorbidity of DSM-IV borderline personality disorder: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions". J Clin Psychiatry. 69 (4): 533–45. PMC 2676679 . PMID 18426259. doi:10.4088/JCP.v69n0404.
- ↑ Gregory, Robert J. (1 November 2006). "Clinical Challenges in Co-occurring Borderline Personality and Substance Use Disorders". Psychiatric Times.
- ↑ Rydén, Göran; Rydén, Eleonore; Hetta, Jerker (2008). "Borderline personality disorder and autism spectrum disorder in females: A cross-sectional study" (PDF). Clinical Neuropsychiatry. 5 (1): 22–30. Retrieved 7 February 2013.
- ↑ Bolton S, Gunderson JG (September 1996). "Distinguishing borderline personality disorder from bipolar disorder: differential diagnosis and implications". Am J Psychiatry. 153 (9): 1202–7. PMID 8780426. doi:10.1176/ajp.153.9.1202.
- ↑ American Psychiatric Association Practice Guidelines (October 2001). "Practice guideline for the treatment of patients with borderline personality disorder. American Psychiatric Association". Am J Psychiatry. 158 (10 Suppl): 1–52. PMID 11665545. doi:10.1176/appi.ajp.158.1.1.
- ↑ "Differential Diagnosis of Borderline Personality Disorder". BPD Today.
- 1 2 3 Chapman & Gratz 2007, p. 87
- 1 2 3 4 5 6 Jamison, Kay R.; Goodwin, Frederick Joseph (1990). Manic-depressive illness. Oxford [Oxfordshire]: Oxford University Press. p. 108. ISBN 0-19-503934-3.
- ↑ Mackinnon DF, Pies R (February 2006). "Affective instability as rapid cycling: theoretical and clinical implications for borderline personality and bipolar spectrum disorders". Bipolar Disord. 8 (1): 1–14. PMID 16411976. doi:10.1111/j.1399-5618.2006.00283.x.
- 1 2 3 Chapman & Gratz 2007, p. 88
- ↑ Selby EA (October 2013). "Chronic sleep disturbances and borderline personality disorder symptoms". J Consult Clin Psychol. 81 (5): 941–7. PMC 4129646 . PMID 23731205. doi:10.1037/a0033201.
- ↑ Akiskal HS, Yerevanian BI, Davis GC, King D, Lemmi H (February 1985). "The nosologic status of borderline personality: clinical and polysomnographic study". Am J Psychiatry. 142 (2): 192–8. PMID 3970243. doi:10.1176/ajp.142.2.192.
- ↑ Gunderson JG, Elliott GR (March 1985). "The interface between borderline personality disorder and affective disorder". Am J Psychiatry. 142 (3): 277–88. PMID 2857532. doi:10.1176/ajp.142.3.277.
- ↑ Paris J (2004). "Borderline or bipolar? Distinguishing borderline personality disorder from bipolar spectrum disorders". Harv Rev Psychiatry. 12 (3): 140–5. PMID 15371068. doi:10.1080/10673220490472373.
- ↑ Jamison, Kay R.; Goodwin, Frederick Joseph (1990). Manic-depressive illness. Oxford [Oxfordshire]: Oxford University Press. p. 336. ISBN 0-19-503934-3.
- ↑ Benazzi F (January 2006). "Borderline personality-bipolar spectrum relationship". Prog. Neuropsychopharmacol. Biol. Psychiatry. 30 (1): 68–74. PMID 16019119. doi:10.1016/j.pnpbp.2005.06.010.
- ↑ Rapkin, AJ; Lewis, EI (November 2013). "Treatment of premenstrual dysphoric disorder". Womens Health (Lond Engl). 9 (6): 537–56. PMID 24161307. doi:10.2217/whe.13.62.
- 1 2 3 4 Grady-Weliky, TA (January 2003). "Premenstrual dysphoric disorder". N. Engl. J. Med. 348 (5): 433–8. PMID 12556546. doi:10.1056/NEJMcp012067.
- ↑ Steriti, Ronald. "Premenstrual Dysphoric Disorder" (PDF). Archived from the original (PDF) on 20 October 2014.
- ↑ "CG78 Borderline personality disorder (BPD): NICE guideline". Nice.org.uk. 28 January 2009. Retrieved 12 August 2009.
- ↑ Paris J (June 2004). "Is hospitalization useful for suicidal patients with borderline personality disorder?". J. Pers. Disord. 18 (3): 240–7. PMID 15237044. doi:10.1521/pedi.18.3.240.35443.
- 1 2 3 4 Zanarini MC (November 2009). "Psychotherapy of borderline personality disorder". Acta Psychiatr Scand. 120 (5): 373–7. PMC 3876885 . PMID 19807718. doi:10.1111/j.1600-0447.2009.01448.x.
- ↑ Cristea, I. A.; Gentili, C.; Cotet, C. D.; Palomba, D.; Barbui, C.; Cuijpers, P. (2017). "Efficacy of Psychotherapies for Borderline Personality Disorder: A Systematic Review and Meta-analysis". JAMA Psychiatry. 74 (4): 319–328. PMID 28249086. doi:10.1001/jamapsychiatry.2016.4287.
- ↑ Links, Paul S.; Shah, Ravi; Eynan, Rahel (2017). "Psychotherapy for Borderline Personality Disorder: Progress and Remaining Challenges". Current Psychiatry Reports. 19 (3): 16. ISSN 1523-3812. PMID 28271272. doi:10.1007/s11920-017-0766-x.
- ↑ Gabbard, G.O. (2014). Psychodynamic psychiatry in clinical practice. 5th Edition. American Psychiatric Publishing: Washington, D.C., pp. 445-448.
- ↑ Stoffers, JM; Völlm, BA; Rücker, G; Timmer, A; Huband, N; Lieb, K (15 August 2012). "Psychological therapies for people with borderline personality disorder.". The Cochrane database of systematic reviews. 8: CD005652. PMID 22895952. doi:10.1002/14651858.CD005652.pub2.
- ↑ Linehan MM, Comtois KA, Murray AM, et al. (July 2006). "Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder". Arch. Gen. Psychiatry. 63 (7): 757–66. PMID 16818865. doi:10.1001/archpsyc.63.7.757.
- 1 2 Paris J (February 2010). "Effectiveness of different psychotherapy approaches in the treatment of borderline personality disorder". Curr Psychiatry Rep. 12 (1): 56–60. PMID 20425311. doi:10.1007/s11920-009-0083-0.
- ↑ Blechner, Mark J. (July 1994). "Projective identification, countertransference, and the 'maybe-me'". Contemporary Psychoanalysis. 30 (3): 619–30. doi:10.1080/00107530.1994.10746876.
- ↑ >Tang YY, Posner MI (Jan 2013). "Special issue on mindfulness neuroscience". Social Cognitive & Affective Neuroscience. 8 (1): 1–3. doi:10.1093/scan/nss104.
- ↑ Posner MI, Tang YY, Lynch G (2014). "Mechanisms of white matter change induced by meditation training". Frontiers in Psychology. 5 (1220): 297–302. doi:10.3389/fpsyg.2014.01220.
- 1 2 Chafos VH, Economou P (July 2014). "Beyond Borderline Personality Disorder: The Mindful Brain". Social Work. 59 (4): 297–302. doi:10.1093/sw/swu030.
- ↑ Sachse S, Keville S, Feigenbaum J (Jun 2011). "A feasibility study of mindfulness-based cognitive therapy for individuals with borderline personality disorder". Psychology and Psychotherapy. 84 (2): 184–200. doi:10.1348/147608310X516387.
- 1 2 3 4 Stoffers, J; Völlm, BA; Rücker, G; Timmer, A; Huband, N; Lieb, K (16 June 2010). "Pharmacological interventions for borderline personality disorder.". The Cochrane database of systematic reviews (6): CD005653. PMC 4169794 . PMID 20556762.
- 1 2 3 Hancock-Johnson, E; Griffiths, C; Picchioni, M (May 2017). "A Focused Systematic Review of Pharmacological Treatment for Borderline Personality Disorder". CNS drugs. 31 (5): 345–356. PMID 28353141. doi:10.1007/s40263-017-0425-0.
- ↑ "The UK National Institute for Health and Clinical Excellence (NICE) 2009 clinical guideline for the treatment and management of BPD" (PDF). Retrieved 6 September 2011.
- ↑ Johnson, R. Skip (26 July 2014). "Treatment of Borderline Personality Disorder". BPDFamily.com. Retrieved 5 August 2014.
- ↑ Zanarini MC, Frankenburg FR, Khera GS, Bleichmar J (2001). "Treatment histories of borderline inpatients". Compr Psychiatry. 42 (2): 144–50. PMID 11244151. doi:10.1053/comp.2001.19749.
- ↑ Zanarini MC, Frankenburg FR, Hennen J, Silk KR (January 2004). "Mental health service utilization by borderline personality disorder patients and Axis II comparison subjects followed prospectively for 6 years". J Clin Psychiatry. 65 (1): 28–36. PMID 14744165. doi:10.4088/JCP.v65n0105.
- ↑ Fallon P (August 2003). "Travelling through the system: the lived experience of people with borderline personality disorder in contact with psychiatric services". J Psychiatr Ment Health Nurs. 10 (4): 393–401. PMID 12887630. doi:10.1046/j.1365-2850.2003.00617.x.
- ↑ Links, Paul S.; Bergmans, Yvonne; Warwar, Serine H. (1 July 2004). "Assessing Suicide Risk in Patients With Borderline Personality Disorder". Psychiatric Times.
- ↑ Lieb K, Zanarini MC, Schmahl C, Linehan MM, Bohus M (2004). "Borderline personality disorder". Lancet. 364 (9432): 453–61. PMID 15288745. doi:10.1016/S0140-6736(04)16770-6.
- 1 2 Zanarini MC, Frankenburg FR, Hennen J, Silk KR (February 2003). "A longitudinal course of borderline psychopathology: 6-year prospective follow-up of the phenomenology of borderline personality disorder". Am J Psychiatry. 160 (2): 274–83. PMID 12562573. doi:10.1176/appi.ajp.160.2.274.
- 1 2 3 Oldham, John M. (July 2004). "Borderline Personality Disorder: An Overview". Psychiatric Times.
- ↑ Zanarini MC, Frankenburg FR, Reich DB, Fitzmaurice G (June 2010). "Time to attainment of recovery from borderline personality disorder and stability of recovery: A 10-year prospective follow-up study". Am J Psychiatry. 167 (6): 663–7. PMC 3203735 . PMID 20395399. doi:10.1176/appi.ajp.2009.09081130. Lay summary – McLean Hospital (15 April 2010).
- ↑ Hirsh JB, Quilty LC, Bagby RM, McMain SF (August 2012). "The relationship between agreeableness and the development of the working alliance in patients with borderline personality disorder". J. Pers. Disord. 26 (4): 616–27. PMID 22867511. doi:10.1521/pedi.2012.26.4.616.
- ↑ Zanarini MC, Frankenburg FR, Hennen J, Reich DB, Silk KR (February 2005). "Psychosocial functioning of borderline patients and axis II comparison subjects followed prospectively for six years". J. Pers. Disord. 19 (1): 19–29. PMID 15899718. doi:10.1521/pedi.19.1.19.62178.
- ↑ Swartz, Marvin; Blazer, Dan; George, Linda; Winfield, Idee (1990). "Estimating the Prevalence of Borderline Personality Disorder in the Community". Journal of Personality Disorders. 4 (3): 257–272. doi:10.1521/pedi.1990.4.3.257.
- ↑ Skodol AE, Bender DS (2003). "Why are women diagnosed borderline more than men?". Psychiatr Q. 74 (4): 349–60. PMID 14686459. doi:10.1023/A:1026087410516.
- ↑ Korzekwa MI, Dell PF, Links PS, Thabane L, Webb SP (2008). "Estimating the prevalence of borderline personality disorder in psychiatric outpatients using a two-phase procedure". Compr Psychiatry. 49 (4): 380–6. PMID 18555059. doi:10.1016/j.comppsych.2008.01.007.
- 1 2 3 "BPD Fact Sheet". National Educational Alliance for Borderline Personality Disorder. 2013.
- ↑ Black DW, Gunter T, Allen J, et al. (2007). "Borderline personality disorder in male and female offenders newly committed to prison". Compr Psychiatry. 48 (5): 400–5. PMID 17707246. doi:10.1016/j.comppsych.2007.04.006.
- ↑ Tove Aarkrog: Edvard Munch: the life of a person with borderline personality as seen through his art, Lundbeck Pharma A/S, Denmark 1990, ISBN 8798352415, p. 34-35.
- ↑ James F. Masterson: Search For The Real Self. Unmasking The Personality Disorders Of Our Age, Chapter 12: The Creative Solution: Sartre, Munch, and Wolfe, p. 208–230, Simon and Schuster, New York 1988, ISBN 1451668910, p. 212-213.
- ↑ Tove Aarkrog: Edvard Munch: the life of a person with borderline personality as seen through his art, Lundbeck Pharma A/S, Denmark 1990, ISBN 8798352415.
- ↑ Millon, Grossman & Meagher 2004, p. 172
- ↑ Charles Hamilton Hughes (1884). "Borderline psychiatric records – prodromal symptoms of psychical impairments". Alienists & Neurology. 5: 85–90. OCLC 773814725.
- 1 2 Millon 1996, pp. 645–690
- ↑ Stern, Adolf (1938). "Psychoanalytic investigation of and therapy in the borderline group of neuroses". Psychoanalytic Quarterly. 7: 467–489.
- 1 2 3 Aronson TA (August 1985). "Historical perspectives on the borderline concept: a review and critique". Psychiatry. 48 (3): 209–22. PMID 3898174.
- ↑ Gunderson JG, Kolb JE, Austin V (July 1981). "The diagnostic interview for borderline patients". Am J Psychiatry. 138 (7): 896–903. PMID 7258348. doi:10.1176/ajp.138.7.896.
- ↑ Stone MH (2005). "Borderline Personality Disorder: History of the Concept". In Zanarini MC. Borderline personality disorder. Boca Raton, FL: Taylor & Francis. pp. 1–18. ISBN 0-8247-2928-5.
- ↑ Kluft, Richard; Goodwin, Jean (1985). Childhood Antecedents of Multiple Personality Disorder: Credibility Problems in Multiple Personality Disorder Patients and Abused Children. American Psychiatric Publishing, Inc. p. 2.
- 1 2 Startup, M.; B. Jones; H. Heard; M. Swales; J.M.G. Williams; R.S.P. Jones (November 1999). "Autobiographical memory and dissociation in borderline personality disorder". Psychological Medicine. 29 (6): 1397–1404. PMID 10616945. doi:10.1017/S0033291799001208.
- 1 2 Linehan 1993, p. 17
- 1 2 Kluft, Richard; Goodwin, Jean (1985). Childhood Antecedents of Multiple Personality Disorder: Credibility Problems in Multiple Personality Disorder Patients and Abused Children. American Psychiatric Publishing, Inc. p. 3.
- ↑ Nehls N (1998). "Borderline personality disorder: gender stereotypes, stigma, and limited system of care". Issues Ment Health Nurs. 19 (2): 97–112. PMID 9601307. doi:10.1080/016128498249105.(subscription required)
- ↑ Becker D (October 2000). "When she was bad: borderline personality disorder in a posttraumatic age". Am J Orthopsychiatry. 70 (4): 422–32. PMID 11086521. doi:10.1037/h0087769.
- ↑ Paris J (2008). Treatment of Borderline Personality Disorder. A Guide to Evidence-Based Practice. The Guilford Press. p. 21.
- 1 2 3 Sansone, Randy A.; Sansone, Lori A. (1 May 2011). "Gender Patterns in Borderline Personality Disorder". Innovations in Clinical Neuroscience. 8 (5): 16–20. ISSN 2158-8333. PMC 3115767 . PMID 21686143.
- ↑ American Psychiatric Association 2000, p. 705
- 1 2 Linehan 1993, p. 14
- ↑ Linehan 1993, p. 15
- ↑ Linehan 1993, p. 18
- ↑ Aviram RB, Brodsky BS, Stanley B (2006). "Borderline personality disorder, stigma, and treatment implications". Harv Rev Psychiatry. 14 (5): 249–56. PMID 16990170. doi:10.1080/10673220600975121.
- 1 2 3 4 5 Chapman & Gratz 2007, p. 31
- 1 2 3 4 5 Chapman & Gratz 2007, p. 32
- ↑ Hinshelwood RD (March 1999). "The difficult patient. The role of 'scientific psychiatry' in understanding patients with chronic schizophrenia or severe personality disorder". Br J Psychiatry. 174 (3): 187–90. PMID 10448440. doi:10.1192/bjp.174.3.187.
- ↑ Cleary M, Siegfried N, Walter G (September 2002). "Experience, knowledge and attitudes of mental health staff regarding clients with a borderline personality disorder". Int J Ment Health Nurs. 11 (3): 186–91. PMID 12510596. doi:10.1046/j.1440-0979.2002.00246.x.
- ↑ Deans C, Meocevic E (2006). "Attitudes of registered psychiatric nurses towards patients diagnosed with borderline personality disorder". Contemp Nurse. 21 (1): 43–9. PMID 16594881. doi:10.5172/conu.2006.21.1.43.
- ↑ Krawitz R (July 2004). "Borderline personality disorder: attitudinal change following training". Aust N Z J Psychiatry. 38 (7): 554–9. PMID 15255829. doi:10.1111/j.1440-1614.2004.01409.x.
- ↑ Vaillant GE (1992). "The beginning of wisdom is never calling a patient a borderline; or, the clinical management of immature defenses in the treatment of individuals with personality disorders". J Psychother Pract Res. 1 (2): 117–34. PMC 3330289 . PMID 22700090.
- ↑ Nehls N (August 1999). "Borderline personality disorder: the voice of patients". Res Nurs Health. 22 (4): 285–93. PMID 10435546. doi:10.1002/(SICI)1098-240X(199908)22:4<285::AID-NUR3>3.0.CO;2-R.
- ↑ Manning 2011, p. ix
- 1 2 Bogod, Elizabeth. "Borderline Personality Disorder Label Creates Stigma". Archived from the original on 2 May 2015.
- ↑ "Understanding Borderline Personality Disorder". Treatment and Research Advancements Association for Personality Disorder. 2004. Archived from the original on 26 May 2013.
- ↑ Porr, Valerie (2001). "How Advocacy is Bringing Borderline Personality Disorder Into the Light". Archived from the original on 20 October 2014.
- ↑ Gunderson, John G.; Hoffman, Perry D. (2005). Understanding and Treating Borderline Personality Disorder A Guide for Professionals and Families. Arlington, Virginia: American Psychiatric Publishing.
- ↑ American Psychiatric Association 2013, pp. 663–6
- ↑ Robinson, David J. (2003). Reel Psychiatry: Movie Portrayals of Psychiatric Conditions. Port Huron, Michigan: Rapid Psychler Press. p. 234. ISBN 1-894328-07-8.
- ↑ Wedding D, Boyd MA, Niemiec RM (2005). Movies and Mental Illness: Using Films to Understand Psychopathology. Cambridge, MA: Hogrefe. p. 59. ISBN 0-88937-292-6.
- ↑ Robinson (Reel Psychiatry: Movie Portrayals of Psychiatric Conditions), p. 235
- ↑ Seltzer, Abby (April 16, 2012). "Shame and A Dangerous Method reviews". The Art of Psychiatry. Retrieved January 13, 2017.
- ↑ Robinson, David J. (1999). The Field Guide to Personality Disorders. Rapid Psychler Press. p. 113. ISBN 0-9680324-6-X.
- ↑ O'Sullivan, Michael (7 May 2015). "Kristen Wiig earns awkward laughs and silence in ‘Welcome to Me’". Washington Post. Retrieved 3 June 2015.
- ↑ Chang, Justin (11 September 2014). "Toronto Film Review: ‘Welcome to Me’: Kristen Wiig plays a woman with borderline personality disorder in this startlingly inspired comedy from Shira Piven". Variety. Retrieved 3 June 2015.
- ↑ Hsu, Jeremy (8 June 2010). "The Psychology of Darth Vader Revealed". LiveScience. TopTenReviews. Retrieved 8 June 2010.
- ↑ HR 1005, 4/1/08
- ↑ "BPD Awareness Month – Congressional History". BPD Today. Mental Health Today. Archived from the original on 8 July 2011. Retrieved 1 November 2010.
References
- Chapman, Alexander L.; Gratz, Kim L. (2007). The Borderline Personality Disorder Survival Guide: Everything You Need to Know About Living with BPD. Oakland, CA: New Harbinger Publications. ISBN 978-1-57224-507-5.
- Linehan, Marsha M.; Comtois, Katherine Anne; Murray, Angela M.; Brown, Milton Z.; Gallop, Robert J.; Heard, Heidi L.; Korslund, Kathryn E.; Tutek, Darren A.; et al. (2006). "Two-Year Randomized Controlled Trial and Follow-up of Dialectical Behavior Therapy vs Therapy by Experts for Suicidal Behaviors and Borderline Personality Disorder". Archives of General Psychiatry. 63 (7): 757–66. PMID 16818865. doi:10.1001/archpsyc.63.7.757.
- Linehan, Marsha (1993). Cognitive-behavioral treatment of borderline personality disorder. New York: Guilford Press. ISBN 0-89862-183-6.
- Manning, Shari (2011). Loving Someone with Borderline Personality Disorder. The Guilford Press. ISBN 978-1-59385-607-6.
- Millon, Theodore (1996). Disorders of Personality: DSM-IV-TM and Beyond. New York: John Wiley & Sons. ISBN 0-471-01186-X.
- Millon, Theodore (2004). Personality Disorders in Modern Life. ISBN 0-471-32355-1.
- Millon, Theodore; Grossman, Seth; Meagher, Sarah E. (2004). Masters of the mind: exploring the story of mental illness from ancient times to the new millennium. John Wiley & Sons. ISBN 978-0-471-46985-8.
- Millon, Theodore (2006). "Personality Subtypes". Institute for Advanced Studies in Personology and Psychopathology. Dicandrien, Inc. Retrieved 1 November 2010.
- American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders (4th ed.). American Psychiatric Association. ISBN 978-0-89042-025-6.
- American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). American Psychiatric Publishing. ISBN 978-0-89042-555-8.
External links
| Classification |
V · T · D |
|---|---|
| External resources |
- Borderline personality disorder at DMOZ
- "Borderline personality disorder". National Institute of Mental Health.
- APA DSM 5 Definition of Borderline personality disorder
- APA Division 12 treatment page for Borderline personality disorder