Alendronic acid
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Fosamax |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a601011 |
| Pregnancy category |
|
| Routes of administration | Oral |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 0.6% |
| Metabolism | excreted unchanged |
| Biological half-life | 126 months |
| Excretion | renal |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| ECHA InfoCard | 100.128.415 |
| Chemical and physical data | |
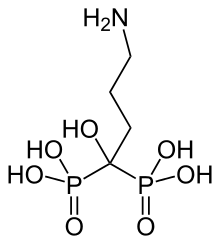
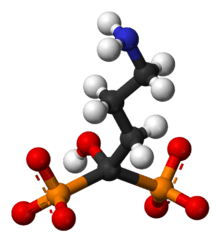
| Formula | C4H13NO7P2 |
| Molar mass | 249.097 |
| 3D model (JSmol) | |
| |
| |
| | |
Alendronic acid (INN) or alendronate sodium (USAN) — sold as Fosamax by Merck — is a bisphosphonate drug used for osteoporosis, osteogenesis imperfecta, and several other bone diseases. It is marketed alone as well as in combination with vitamin D (2,800 IU and 5,600 IU, under the name Fosamax+D). Merck's U.S. patent on alendronate expired in 2008 and the drug is now available as a generic. It is the most widely prescribed bisphosphonate medicine in the United States .
Pharmaceutical analysis
As with all potent bisphosphonates, the fraction of the drug that reaches the circulatory system intact (systemic bioavailability) after oral dosing is low, averaging only 0.6–0.7% in women and in men under fasting conditions. Intake together with meals and beverages other than water further reduces the bioavailability. The absorbed drug rapidly partitions, with approximately 50% binding to the exposed bone surface; the remainder is excreted unchanged by the kidneys. Unlike with most drugs, the strong negative charge on the two phosphonate moieties limits oral bioavailability, and, in turn, the exposure to tissues other than bone is very low. After absorption in the bone, alendronate has an estimated terminal elimination half-life of 10 years.[1]
Pharmacology
Alendronate inhibits osteoclast-mediated bone-resorption. Like all bisphosphonates, it is chemically related to inorganic pyrophosphate, the endogenous regulator of bone turnover. But while pyrophosphate inhibits both osteoclastic bone resorption and the mineralization of the bone newly formed by osteoblasts, alendronate specifically inhibits bone resorption without any effect on mineralization at pharmacologically achievable doses. Its inhibition of bone-resorption is dose-dependent and approximately 1,000 times stronger than the equimolar effect of the first bisphosphonate drug, etidronate. Under therapy, normal bone tissue develops, and alendronate is deposited in the bone-matrix in a pharmacologically inactive form. For optimal action, enough calcium and vitamin D are needed in the body in order to promote normal bone development. Hypocalcemia should, therefore, be corrected before starting therapy.
Etidronate has the same disadvantage as pyrophosphate in inhibiting mineralization, but all of the potent N-containing bisphosphonates including Alendronate and also risedronate, ibandronate, and zoledronate, do not.
Clinical data
Treatment of post-menopausal women and people with osteogenesis imperfecta over the age of 22 with alendronic acid has demonstrated normalization of the rate of bone turnover, significant increase in BMD (bone mineral density) of the spine, hip, wrist and total body, and significant reductions in the risk of vertebral (spine) fractures, wrist fractures, hip fractures, and all non-vertebral fractures. In the Fracture Intervention Trial, the women with the highest risk of fracture (by virtue of pre-existing vertebral fractures) were treated with Fosamax 5 mg/day for two years followed by 10 mg/day for the third year. This resulted in approximately 50% reductions in fractures of the spine, hip, and wrist compared with the control group taking placebos. Both groups also took calcium and vitamin D.[2]
Uses
- Prophylaxis and treatment of female osteoporosis
- Treatment of male osteoporosis
- Prevention and treatment of corticosteroid-associated osteoporosis together with supplements of calcium and vitamin D
- Paget's disease
- Treatment for Osteogenesis imperfecta in patients of 18 years or older
- Dental implants coating (experimental)
Contraindications and precautions
- Acute inflammations of the gastrointestinal tract (esophagitis, gastritis, ulcerations)
- Clinically manifest osteomalacia
- Certain malformations and malfunctions of the esophagus (strictures, achalasia)
- Inability to stand, walk, or sit for 30 minutes after oral administration
- Renal impairment with a creatinine clearance below 30ml/min
- Hypersensitivity to alendronate or another ingredient
- Hypocalcemia
- Pregnancy and breastfeeding
- Patients below 18 yrs. of age, as no clinical data exists
Side-effects
- Gastrointestinal tract:
- Ulceration of the esophagus; this may require hospitalization and intensive treatment. Gastric and duodenal ulceration may also occur.
- Esophageal cancer, a meta-analysis concluded that bisphosphonate treatment is not significantly associated with excess risk of esophageal cancer.[3][4]
- General: infrequent cases of skin rash, rarely manifesting as Stevens–Johnson syndrome and toxic epidermal necrolysis, eye problems (uveitis, scleritis) and generalized muscle, joint, and bone pain [5] (rarely severe) have been seen. In laboratory tests decreased calcium and phosphate values may be obtained but reflect action of the drug and are harmless.
- Osteonecrosis of the jaw (deterioration of the temporomandibular joint or TMJ) may occur while on this drug, if dental work of any kind is carried out.[6] Although this side effect is uncommon, it occurs primarily in patients being administered intravenous biphosphonates, with most cases being reported in cancer patients.[7][8]
- Bone: alendronate has been linked in long-term users to the development of low-impact femoral fractures.[9] Further, studies suggest that users of alendronate have an increase in the numbers of osteoclasts and develop giant, more multinucleated osteoclasts; the significance of this development is unclear.[10] Fosamax has been linked to a rare type of leg fracture that cuts straight across the upper thigh bone after little or no trauma (subtrochanteric fractures).[11]
Interactions
- Milk, diet, and drugs containing high amounts of calcium, magnesium or aluminium (antacids): the absorption of alendronate is decreased. At least half an hour should pass after intake of alendronate before taking the supplement or drug.
- Highly active vitamin D analogues or fluorides: no data is available. Concomitant treatment should be avoided.
- The additional beneficial effect of HRT (hormone replacement therapy) with estrogens/progestins or raloxifene in postmenopausal women remains to be elucidated, but no interactions have been seen. The combination is therefore possible.
- Intravenous ranitidine increases the oral bioavailability of alendronate. No clinical consequences are known.
- The combination of NSAIDs and alendronate may increase the risk of gastric ulcers. Both these drugs have the potential to irritate the upper gastro-intestinal mucosa.
Dosage
- Prophylaxis of osteoporosis in women: 5–10 mg daily or 35–70 mg weekly.
- Therapy of osteoporosis in women and men : 10 mg daily or 70 mg weekly.
- Osteoporosis under corticosteroids: 5–10 mg daily or 35–70 mg weekly in men and premenopausal women or those receiving concomitant HRT. In postmenopausal women not receiving HRT, the recommended dose is 10 mg daily or 70 mg weekly.
- Paget's disease: 40 mg daily for 6 months.
The risk of esophageal irritation places special requirements on how this oral drug is taken. The patient should take the drug only upon rising for the day with 8 oz. of water, and stand, walk, or sit, and remain fasting for 30–45 minutes afterwards (preferably 1–2 hours), then eat breakfast. No other medications should be taken for this time. Lying down or reclining after taking the drug and prior to eating breakfast may cause gastroesophageal reflux and esophageal irritation.
_Oral_Tablet.jpg)
Dosage forms
- Fosamax solution 70 mg/75ml
- Fosamax tablets 5 mg, 10 mg, 35 mg, 40 mg, and 70 mg
References
- ↑ Shinkai I, Ohta Y (January 1996). "New drugs--reports of new drugs recently approved by the FDA. Alendronate". Bioorg. Med. Chem. 4 (1): 3–4. PMID 8689235. doi:10.1016/0968-0896(96)00042-9.
- ↑ Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, Bauer DC, Genant HK, Haskell WL, Marcus R, Ott SM, Torner JC, Quandt SA, Reiss TF, Ensrud KE (December 1996). "Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group". Lancet. 348 (9041): 1535–41. PMID 8950879. doi:10.1016/S0140-6736(96)07088-2.
- ↑ Sun K, Liu JM, Sun HX, Lu N, Ning G (October 2012). "Bisphosphonate treatment and risk of esophageal cancer: a meta-analysis of observational studies". Osteoporosis International. 24 (1): 279–86. PMID 23052941. doi:10.1007/s00198-012-2158-8.
- ↑ Haber SL, McNatty D (March 2012). "An evaluation of the use of oral bisphosphonates and risk of esophageal cancer". Ann Pharmacother. 46 (3): 419–23. PMID 22333262. doi:10.1345/aph.1Q482.
- ↑ FDA Patient Safety News, March 2008
- ↑ Fosamax product description, Merck & Co
- ↑ Pazianas, M.; Miller P; Blumentals WA; Bernal M; Kothawala P (August 29, 2007). "A review of the literature on osteonecrosis of the jaw in patients with osteoporosis treated with oral bisphosphonates: prevalence, risk factors, and clinical characteristics". Clinical Therapy. 29 (8): 1548–58. PMID 17919538. doi:10.1016/j.clinthera.2007.08.008.
- ↑ Carini, F.; Barbano L; Saggese V; Monai D; Porcaro G. (2012-04-03). "Multiple systemic diseases complicated by bisphosphonate osteonecrosis: a case report.". Ann Stomatol (Roma). 3 (2 Suppl): 32–6. PMC 3512552
 . PMID 23285320.
. PMID 23285320. - ↑ Lenart BA, Lorich DG, Lane JM (March 2008). "Atypical fractures of the femoral diaphysis in postmenopausal women taking alendronate". N. Engl. J. Med. 358 (12): 1304–6. PMID 18354114. doi:10.1056/NEJMc0707493. Lay summary – US News & World Report.
- ↑ Weinstein RS, Roberson PK, Manolagas SC (January 2009). "Giant osteoclast formation and long-term oral bisphosphonate therapy". N. Engl. J. Med. 360 (1): 53–62. PMC 2866022 . PMID 19118304. doi:10.1056/NEJMoa0802633. Lay summary – Washington Post.
- ↑ Kwek EB, Goh SK, Koh JS, Png MA, Howe TS (February 2008). "An emerging pattern of subtrochanteric stress fractures: a long-term complication of alendronate therapy?". Injury. 39 (2): 224–31. PMID 18222447. doi:10.1016/j.injury.2007.08.036.