Achilles tendinitis
| Achilles tendonitis | |
|---|---|
| Synonyms | Achilles tenosynovitis, Achilles tendinopathy |
| Classification and external resources | |
| Specialty | rheumatology |
| ICD-10 | M76.6 |
| ICD-9-CM | 726.71 |
| DiseasesDB | 31726 |
| MedlinePlus | 001072 |
| eMedicine | sports/2 |
Achilles tendinitis is tendinitis of the Achilles tendon, generally caused by overuse of the affected limb and is more common among athletes training under less than ideal conditions. It should not be confused with xanthoma of the tendon, which is the accumulation of cholesterol in patients with familial hypercholesterolemia.
Signs and symptoms
Symptoms can vary from an ache or pain and swelling to the local area of the ankles, or a burning that surrounds the whole joint. With this condition, the pain is usually worse during and after activity, and the tendon and joint area can become stiffer the following day as swelling impinges on the movement of the tendon. Many patients report stressful situations in their lives in correlation with the beginnings of pain which may contribute to the symptoms.
Cause


Development of tendinitis depends on the type, frequency and severity of exercise or use; for example, rock climbers tend to develop tendinitis in their fingers, swimmers in their shoulders. Achilles tendinitis is a common injury, particularly in sports that involve lunging and jumping. It is also a known side effect of fluoroquinolone antibiotics such as ciprofloxacin.
Swelling in a region of micro-damage or partial tear can be detected visually or by touch. Increased water content and disorganized collagen matrix in tendon lesions may be detected by ultrasonography or magnetic resonance imaging.
Achilles tendinitis is thought to have physiological, mechanical, or extrinsic (i.e. footwear or training) causes. Physiologically, the Achilles tendon is subject to poor blood supply through the synovial sheaths that surround it. This lack of blood supply can lead to the degradation of collagen fibers and inflammation.[1] Tightness in the calf muscles has also been known to be involved in the onset of Achilles tendinitis.[2]
During the loading phase of the running and walking cycle, the ankle and foot naturally pronate and supinate by approximately 5 degrees.[3] Excessive pronation of the foot (over 5 degrees) in the subtalar joint is a type of mechanical mechanism that can lead to tendinitis.[2][3]
An overuse injury refers to repeated stress and strain, which is likely the case in endurance runners.[4][5] Overuse can simply mean an increase in running, jumping or plyometric exercise intensity too soon. Another consideration would be the use of improper or worn-down footwear, which lack the necessary support to maintain the foot in the natural/normal pronation.[5]
Pathophysiology
The Achilles tendon does not have good blood supply or cell activity, so this injury can be slow to heal. The tendon receives nutrients from the tendon sheath or paratendon. When an injury occurs to the tendon, cells from surrounding structures migrate into the tendon to assist in repair. Some of these cells come from blood vessels that enter the tendon to provide direct blood flow to increase healing. With the blood vessels come nerve fibers. Researchers including Alfredson and his team in Sweden [6] believe these nerve fibers to be the cause of the pain - they injected local anaesthetic around the vessels and this decreased significantly the pain from the Achilles tendon.
Prevention
Deteriorating changes start to appear with age, but attempting to slow down these changes is key in the prevention of Achilles tendinitis. Performing consistent physical activity will improve the elasticity and strength of the tendon, which will assist in resisting the forces that are applied.[7]
It is essential to stretch and warm-up before beginning an exercise session in order to prepare and protect the tendon for work. Warm-ups enhance the tendon's capability of being stretched, further aiding in protection from injury.[8] Prevention of recurrence includes following appropriate exercise habits and wearing low-heeled shoes. In the case of incorrect foot alignment, orthotics can be used as a preventative way to properly position the feet.[7] Footwear that is specialized to provide shock-absorption can be utilized to defend the longevity of the tendon.[9] Achilles tendon injuries can be the result of exceeding the tendon's capabilities for loading, therefore it is important to gradually adapt to exercise if someone is inexperienced, sedentary, or is an athlete who is not progressing at a steady rate.[9]
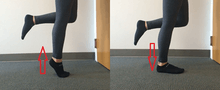
Preventive exercises are aimed at strengthening the gastrocnemius and soleus muscles, typically by eccentric strengthening exercises.[11] This eccentric training method is especially important for individuals with chronic Achilles Tendinosis which is classified as the degeneration of collagen fibers.[9] Eccentric exercises improve the tensile strength of the tendon and lengthen the muscle-tendon junction, decreasing the amount of strain experienced with ankle joint movements.[9] These involve repetitions of slowly raising and lowering the body while standing on the affected leg, using the opposite arm to assist balance and support if necessary, and starting with the heel in a hyperextended position. (Hyperextension is typically achieved by balancing the forefoot on the edge of a step, a thick book, or a barbell weight. so that the point of the heel is a couple of inches below the forefoot.)
Diagnosis
.jpg)
Achilles tendinitis is mainly diagnosed by a medical history taking and a physical examination. Projectional radiography shows calcification deposits within the tendon at its calcaneal insertion in approximately 60 percent of cases.[12] Magnetic resonance imaging (MRI) can determine the extent of tendon degeneration, and may show differential diagnoses such as bursitis.[12]
Treatment
Treatment is possible with ice, cold compression therapy, wearing heel pads to reduce the strain on the tendon, and an exercise routine designed to strengthen the tendon (see eccentric strengthening, above). Some people have reported vast improvement after applying light to medium compression around ankles and lower calf by wearing elastic bandages throughout the day. Using these elastic bandages while sleeping can reduce morning stiffness but care must be taken to apply very light compression during sleep. Compression can inhibit healing by hindering circulation.[13] Seeing a professional for treatment as soon as possible is important, because this injury can lead to an Achilles tendon rupture with continued overuse. Other treatments may include non-steroidal anti-inflammatory drugs, such as ibuprofen, ultrasound therapy, manual therapy techniques, a rehabilitation program, and in rare cases, application of a plaster cast. Steroid injection is sometimes used, but must be done after very careful, expert consideration because it can increase the risk of tendon rupture.[14] There has recently been some interest in the use of autologous blood injections; however the results have not been highly encouraging and there is little evidence for their use.[15][16]
More specialised therapies include prolotherapy (sclerosant injection into the neovascularity) and extracorporeal shockwave therapy may have some additional benefit.[17] The evidence is however limited.
Epidemiology
The prevalence of Achilles tendinitis fluctuates greatly among different ages and groups of people. However, Achilles tendinitis is most commonly found in individuals aged 30–40.[18] A study was conducted in 1981 on recreational and competitive runners and what type of injury they were most likely to suffer from. Out of the 232 runners, 25 (11%) complained that their Achilles bothered them.[18]
A study conducted in the city of Oulu found that a peak incidence of 18 injured Achilles occurred in 1994 and was highest in the male group aged 30–39. The study also found that 90% of the injuries occurred while playing a sport.[19]
Risk factors include participating in a sport or activity that involves running, jumping, bounding, and change of speed. Although Achilles tendinitis is mainly diagnosed in runners, it does occur in basketball, volleyball, dancing, gymnastics and other athletic activities.[18] Other risk factors include gender, age, improper stretching, overuse, and conditions which the individual may be born with.[20] Congenital conditions occur when an individual’s legs rotate abnormally, which in turn causes the lower extremities to overstretch and contract; this puts stress on the Achilles tendon and will eventually cause Achilles tendinitis.[20]
References
- ↑ Fenwick S. A.; Hazleman B. L.; Riley G. P. (2002). "The vasculature and its role in the damaged and healing tendon". Arthritis Research. 4 (4): 252–260.
- 1 2 Maffulli N.; Sharma P.; Luscombe K. L. (2004). "Achilles tendinopathy: aetiology and management". Journal of the Royal Society of Medicine. 97 (10): 472–476. doi:10.1258/jrsm.97.10.472.
- 1 2 Hintermann B., Nigg B. M. (1998). "Pronation in runners". Sports Medicine. 26 (3): 169–176. PMID 9802173. doi:10.2165/00007256-199826030-00003.
- ↑ Kannus P (1997). "Etiology and pathophysiology of chronic tendon disorders in sports". Scandinavian Journal of Sports Medicine. 7 (2): 78–85.
- 1 2 McCrory J. L.; Martin D. F.; Lowery R. B.; Cannon D. W.; Curl W. W.; Read Jr H. M.; Hunter D.M.; Craven T.; Messier S. P. (1999). "Etiologic factors associated with Achilles tendinitis in runners". Medicine and Science in Sports and Exercise. 31 (10): 1374–1381. doi:10.1097/00005768-199910000-00003.
- ↑ Alfredson, H.; Ohberg, L.; Forsgren, S. (Sep 2003). "Is vasculo-neural ingrowth the cause of pain in chronic Achilles tendinosis? An investigation using ultrasonography and colour Doppler, immunohistochemistry, and diagnostic injections.". Knee Surg Sports Traumatol Arthrosc. 11 (5): 334–8. PMID 14520512. doi:10.1007/s00167-003-0391-6.
- 1 2 Hess G.W. (2009). "Achilles Tendon Rupture: A Review of Etiology, Population, Anatomy, Risk Factors, and Injury Prevention". Foot & Ankle Specialist. 3 (1): 29–32. doi:10.1177/1938640009355191.
- ↑ Leppilahti J., Orava S. (1998). "Total Achilles Tendon Rupture: A Review" (PDF). Sports Medicine. 2: 79–100.
- 1 2 3 4 Alfredson H., Lorentzon R. (2012). "Chronic Achilles Tendinosis: Recommendations for Treatment and Prevention". Sports Medicine. 29: 135–146. doi:10.2165/00007256-200029020-00005.
- ↑ Floyd, R.T. (2009). Manual of Structural Kinesiology. New York, NY: McGraw Hill
- ↑ G T Allison, C Purdam. Eccentric loading for Achilles tendinopathy — strengthening or stretching? Br J Sports Med 2009;43:276-279
- 1 2 "Insertional Achilles Tendinitis". American Orthopaedic Foot & Ankle Society. Retrieved 2017-01-17.
- ↑ Christopoulos DG, Nicolaides AN, Szendro G, Irvine AT, Bull M, Eastcott HH (1987). "Air-plethysmography and the effect of elastic compression on venous hemodynamics of the leg.". J Vasc Surg. 5 (1): 148–59. PMID 3795381. doi:10.1067/mva.1987.avs0050148.
- ↑ Nannini CC (2012). "Achilles Tendon Rupture". emedicinehealth.com. Retrieved February 12, 2012.
- ↑ "JBJS | Limited Evidence Supports the Effectiveness of Autologous Blood Injections for Chronic Tendinopathies". jbjs.org. 2012. Retrieved February 12, 2012.
- ↑ de Vos RJ, van Veldhoven PL, Moen MH, Weir A, Tol JL, Maffulli N (2012). "Autologous growth factor injections in chronic tendinopathy: a systematic review". bmb.oxfordjournals.org. Retrieved February 12, 2012.
- ↑ Maffulli N, Longo UG, Denaro V (Nov 3, 2010). "Novel approaches for the management of tendinopathy.". The Journal of bone and joint surgery. American volume. 92 (15): 2604–13. PMID 21048180. doi:10.2106/JBJS.I.01744.
- 1 2 3 Leach R. E.; James S.; Wasilewski S. (1981). "Achilles tendinitis". The American journal of sports medicine. 9 (2): 93–98. doi:10.1177/036354658100900204.
- ↑ Leppilant J.; Puranen J.; Orava S. (1996). "Incidence of Achilles Tendon Injury". Acta Orthopaedica. 67 (3): 277–79.
- 1 2 Kainberger, F; Fialka, V; Breitenseher, M; Kritz, H; Baldt, M; Czerny, C; Imhof, H (1996). "Differential diagnosis of diseases of the Achilles tendon. A clinico-sonographic concept". Der Radiologe. 36 (1): 38–46. PMID 8820370.