Supraspinatus muscle
| Supraspinatus muscle | |
|---|---|
 Position of the supraspinatus muscle (red) seen from the back. | |
 Posterior view of muscles connecting the upper extremity to the vertebral column. Supraspinatus muscle is labeled in red at right, while it is covered by other muscles at left. | |
| Details | |
| Origin | supraspinous fossa of scapula |
| Insertion | superior facet of greater tubercle of humerus |
| Artery | suprascapular artery |
| Nerve | suprascapular nerve |
| Actions | abduction of arm and stabilizes humerus see part on controversy of action. |
| Identifiers | |
| Latin | musculus supraspinatus |
| Dorlands /Elsevier | m_22/12551039 |
| TA | A04.6.02.006 |
| FMA | 9629 |
The supraspinatus (plural supraspinati, from Latin supraspinatus) is a relatively small muscle of the upper back that runs from the supraspinatous fossa superior of the scapula (shoulder blade) to the greater tubercle of the humerus. It is one of the four rotator cuff muscles and also abducts the arm at the shoulder. The spine of the scapula separates the supraspinatus muscle from the infraspinatus muscle, which originates below the spine.
Structure
The supraspinatus muscle arises from the supraspinous fossa, a shallow depression in the body of the scapula above its spine. The supraspinatus muscle tendon passes laterally beneath the cover of the acromion. Research in 1996 showed that the postero-lateral origin was more lateral than classically described.[1][2]
The supraspinatus tendon is inserted into the superior facet of the greater tubercle of the humerus.[3] The distal attachments of the three rotator cuff muscles that insert into the greater tubercle of the humerus can be abbreviated as SIT when viewed from superior to inferior (for supraspinatus, infraspinatus, and teres minor), or SITS when the subscapularis muscle, which attaches to the lesser tubercle of the humerus, is included.[4]
Innervation
The suprascapular nerve innervates the supraspinatus muscle as well as the infraspinatus muscle. It comes from the upper trunk of the brachial plexus.
The intention to contract the supraspinatus muscle begins with neurons in the motor association area of the frontal lobes of the brain. Signals are received by the dendrites on the soma of the neurons. The soma houses the nucleus and the major organelles. The axon extends from one side of the soma, and once the signals sum to reach a potential of -55mV, an action potential will be generated and it will travel down the axon until it reaches the synaptic knob. The potential across the membrane is determined by the ratio of Na+ and K+ ions. Once the -55mV threshold is reached, voltage-gated Na+ channels open quickly, and as Na+ enters the cell, it further depolarizes the membrane. As the rising potential passes 0 mV, Na+ channels begin closing. As they reach +35 mV, they close completely and the K+ channels are fully open. This repolarizes the membrane. The action potential consists of the up-and-down voltage shifts that occur from the time the threshold is reached to the time the voltage returns to the resting membrane potential. As the impulse travels towards the synaptic knob, the speed of propagation is affected by the axon diameter (larger axon, faster conduction), and the presence or absences of myelin. Unmyelinated axons have continuous conduction, whereas myelinated axons have saltatory conduction. With saltatory conduction, the voltage gated channels are concentrated in the nodes of Ranvier. When Na+ enters the axon, it diffuses for a short distance along the inner face of the membrane. Each sodium ion has an electrical field around it. When one Na+ ion moves towards another, its field repels the second ion, which moves slightly and repels another, and so forth. No one ion moves very far, but this energy transfer travels down the axon much faster and farther than any of the individual ions. As the energy travels, channels are opened at subsequent nodes. The intention to contract the supraspinatus muscle travels through the neurons via saltatory conduction.
Neurons in the motor association area assess the degree and sequence of movement required and send the information to upper motor neurons of the precentral gyrus. From there, signals are sent caudally through fibers in projection tracts. The fibers then decussate in the lower medulla oblongata and form the lateral corticospinal tract on each side of the spinal cord. This means that the signal crosses to the opposite side of the body. (Innervation of the right supraspinatus comes from action in the left hemisphere of the brain). The upper motor neuron synapses with the lower motor neuron in the anterior horn of the spinal cord. Synaptic vesicles filled with neurotransmitters are released from the presynaptic membrane on the upper motor neuron and travel across the synapse to signal the dendrites on the lower motor neuron. This is known as an axodendritic synapse. Again, once the membrane potential is raised from -70mV to -55mV, and action potential will be generated for the lower motor neuron. The axon of the lower motor neuron forms the suprascapular nerve (Fig. 2) which is rooted to the spinal cord at C5and C6, and comes off of the upper trunk of the brachial plexus. It then leads the rest of the way to the neuro muscular junction of the supraspinatus muscle.
At the neuromuscular junction, the signal causes voltage-gated calcium channels to open, which stimulates the release of vesicles containing acetylcholine across the synapse. ACh then binds to receptors on the surface of the sarcolemma of the muscle. The sarcolemma of the supraspinatus muscled has junctional folds to increase the surface area of ACh-senstitive membrane. Acetylcholinesterase breaks down the ACh once it has innervated the muscle. Therefore, the action potential from the suprascapular nerve fibers then leads to an action potential in the supraspinatus muscle fibers. Once ACh binds with receptors on the sarcolemma, Na+ flows into the muscle cell and K+ flows out, creating an end-plate potential. The action potential then spreads over the entire muscle surface. When it reaches the t-tubules, it spreads down them into the cell interior. The potential opens voltage-gated calcium channels which allow Ca2+ to leave the sarcoplasmic reticulum and enter the cytosol. Incoming calcium binds to troponin in the thin filaments of the muscle fiber. The troponin-tropomyosin complex changes shape and exposes the active sites on the actin filaments, making them available for binding to myosin heads. ATP then binds to a myosin head. ATPase hydrolyzes the ATP molecule, creating energy for the myosin head to “cock” in an extended position. The head binds to an actin active site, forming a cross-bridge. Myosin releases the hydrolyzed ADP and Pi, therefore completing a single flexing motion, known as a power stroke. ATP then binds to myosin again to destabilize the myosin-actin bond, and effectively breaking the cross-bridge. The myosin is then prepared to repeat the whole process- it will hydrolyze the new ATP, recock (the recovery stroke), attach to a new active site further down the thin filament, and produce another power stroke. The nerve impulse rapidly propagates through the muscle fibers, causing the supraspinatus muscle to contract. [5] [6]
This nerve can be damaged along its course in fractures of the overlying clavicle, which can reduce the person’s ability to initiate the abduction.
Repair
One study has indicated that arthroscopic surgery for full-thickness supraspinatus tears is effective for improving shoulder functionality.[7]
Function
Contraction of the supraspinatus muscle leads to abduction of the arm at the shoulder joint. It is the main agonist muscle for this movement during the first 15 degrees of its arc. Beyond 15 degrees the deltoid muscle becomes increasingly more effective at abducting the arm and becomes the main propagator of this action.[8]
The supraspinatus muscle is one of the musculotendinous support structures called the rotator cuff that surround and enclose the shoulder. It helps to resist the inferior gravitational forces placed across the shoulder joint due to the downward pull from the weight of the upper limb.
The supraspinatus also helps to stabilize the shoulder joint by keeping the head of the humerus firmly pressed medially against the glenoid fossa of the scapula.
Without a functioning supraspinatus, the physician must start abducting the patient's arm and eventually the patient will be able to finish abduction if the deltoid is functional, which is common because the supraspinatus is innervated by the suprascapular nerve from the superior/upper trunk of the brachial plexus. The deltoid is innervated more distally by the axillary nerve, which arises from the posterior cord of the brachial plexus.
Controversy about action
In a 1963 experimental human study on the function of the supraspinatus muscle by Van Linge and Mulder at the State University in Leiden, data were provided arguing that the supraspinatus does not cause the first 30 degrees of abduction, as widely accepted before this report, but is, rather, a synergistic muscle that assists the deltoid (but does not abduct alone).[9] In the study, the supraspinati of subjects were anaesthetised; the deltoid muscle remained able to complete a full range of abduction. (However, the deltoid was unable to sustain an isometric contraction for more than one minute.) This study suggested that the "true" action of the supraspinatus is to hold the capsule in position to allow greater functional strength and stamina of the deltoid muscle.
In support of this study, one should also consider the basic mechanics of the forces involved in abduction of the shoulder. The supraspinatus is a smaller and weaker muscle compared to deltoid on three counts: deltoid has three large components (anterior, middle, and posterior fiber groups); the middle fibers have a multipennate arrangement believed to pack more muscle power into a relatively compact space;[10] and it attaches to the deltoid tuberosity half way down the humerus, adding to the mechanical advantage to abduct the arm. Thus the bulk, arrangement and insertion of the deltoid fibres are designed for the power needed to overcome the load of the weight of the arm plus any load in the hand. By contrast, supraspinatus is a much smaller muscle with convergent fibers leading to a tendon that attaches on the highest facet on the greater tubersosity of the humerus, thereby affording it minimal traction on the arm. The arm is a very long lever with the added weight of muscles and other soft tissues. In 1994, Sharkey and coworkers reported that the whole of the rotator cuff group contributes to abduction of the arm, reducing the work of deltoid by 41%.[11] They strongly suggested that the rotator cuff acts synergistically in concert with deltoid to stabilize the head of the humerus, while the deltoid provides the turning moment at the gleno-humeral joint to abduct the arm. They note that if the deltoid is palpated when abduction is initiated, active contraction of the muscle can be detected—suggesting co-contraction of deltoid with the rotator cuff, rather than after initiation by any of the rotator cuff muscles.
Additional images
-

Position of the supraspinatus muscle (shown in red). Animation.
-

Muscles around the left shoulder, seen from behind.
3. Latissimus dorsi muscle
5. Teres major muscle
6. Teres minor muscle
7. Supraspinatus muscle
8. Infraspinatus muscle
13. long head of Triceps brachii muscle. -
.gif)
Action of right supraspinatus muscle, anterior view. Three bones shown are acromion (top) and coracoid process (center) of scapula, and humerus (left).
-

Diagram of the human shoulder joint
-

Left scapula. Dorsal surface.
-
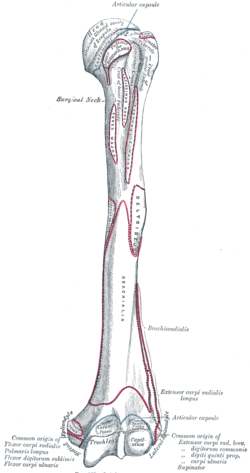
Left humerus. Anterior view.
-

The scapular and circumflex arteries.
-

The right brachial plexus with its short branches, viewed from in front.
-

Suprascapular and axillary nerves of right side, seen from behind.
-

The suprascapular, axillary, and radial nerves.
References
- ↑ Thomazeau, H.; Duval, J. M.; Darnault, P.; Dréano, T. (1996). "Anatomical relationships and scapular attachments of the supraspinatus muscle". Surgical and Radiologic Anatomy 18 (3): 221–5. doi:10.1007/BF02346130. PMID 8873337.
- ↑ D.F. Gazielly, P. Gleyze & T. Thomas, 1996, "The Cuff," Elsevier, ISBN 2906077844, see , accessed 21 November 2014.
- ↑ "Injured Shoulder". Retrieved 16 December 2015.
- ↑ MedicalMnemonics.com: 35
- ↑ http://thebrain.mcgill.ca/flash/d/d_06/d_06_m/d_06_m_mou/d_06_m_mou.html
- ↑ Saladin, Kenneth S. Anatomy & Physiology: The Unity of Form and Function. New York, NY: McGraw-Hill, 2007. Print.
- ↑ Bennett, William F. "Arthroscopic Supraspinatus Repair". Bennett Orthopedics & Sportsmedicine. Retrieved 19 December 2014.
- ↑ Gray´s Anatomy for students 3rd edition
- ↑ van Linge, B.; Mulder, J. D. (1963). "Function of the Supraspinatus Muscle and Its Relation to the Supraspinatus Syndrome. An Experimental Study in Man". The Journal of bone and joint surgery. British volume 45 (4): 750–4. PMID 14074328.
- ↑ Gray's Anatomy 37th Edition 1987
- ↑ Sharkey, Neil A.; Marder, Richard A.; Hanson, Peter B. (1994). "The entire rotator cuff contributes to elevation of the arm". Journal of Orthopaedic Research 12 (5): 699–708. doi:10.1002/jor.1100120513. PMID 7931787.
External links
| Wikimedia Commons has media related to Supraspinatus muscles. |
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||