Sciatica
| Sciatica | |
|---|---|
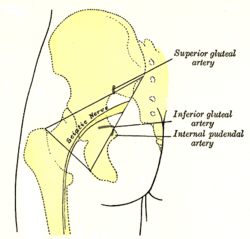 Left buttock, showing surface markings for arteries and sciatic nerve | |
| Classification and external resources | |
| Pronunciation | /saɪˈætɪkə/ |
| Synonyms | sciatic neuritis, sciatic neuralgia, lumbar radiculopathy |
| Specialty | Orthopedics, neurology |
| ICD-10 | M54.3-M54.4 |
| ICD-9-CM | 724.3 |
| MedlinePlus | 000686 |
| eMedicine | emerg/303 |
| MeSH | D012585 |
Sciatica is a medical condition of pain going down the leg from the lower back.[1] This pain may go down the back, outside, or front of the leg. Typically, symptoms are only on one side of the body. Certain causes, however, may result in pain on both sides. Lower back pain is sometimes but not always present. Weakness or numbness may occur in various parts of the leg and foot.[2]
About 90% of the time sciatica is due to a spinal disc herniation pressing on one of the lumbar or sacral nerve roots.[3] Other problems that may result in sciatica include spondylolisthesis, spinal stenosis, piriformis syndrome, pelvic tumors, and compression by a baby's head during pregnancy. The straight-leg-raising test is often helpful in diagnosis. The test is positive if, when the leg is raised while a person is lying on their back, pain shoots below the knee.[2] In most cases medical imaging is not needed. Exceptions to this are when bowel or bladder function is affected, there is significant loss of feeling or weakness, symptoms are long standing, or there is a concern of a tumor or infection.[4] Conditions that may present similarly are diseases of the hip and early herpes zoster before the rash appears.[2]
Treatment initially is typically with pain medications.[4] It is generally recommended that people continue with activities to the best of their abilities.[2] Often all that is required is time and in about 90% of people the problem goes away in less than six weeks. If the pain is severe and lasts for more than six weeks then surgery may be an option.[4] While surgery often speeds pain improvement, long term benefits are unclear.[2] Surgery may be required if complications occur such as bowel or bladder problems.[4] Many treatments including: steroids, gabapentin, acupuncture, heat or ice, and spinal manipulation have poor evidence for their use.[2][5]
Depending on how it is defined, 2% to 40% of people have sciatica at some point in time.[3] It is most common during people's 40s and 50s, and men are more frequently affected than women.[2][4] The condition has been known since ancient times.[2] The first known use of the word sciatica dates from 1451.[6]
Definition
The term sciatica describes a symptom rather than a specific disease. Some use it to mean any pain starting in the lower back and going down the leg. Others use the term more specifically to mean a nerve dysfunction caused by compression of one or more lumbar or sacral nerve roots from a spinal disc herniation. Pain typically occurs in the distribution of a dermatome and goes below the knee to the foot. It may be associated with neurological dysfunction, such as weakness.[3] The pain is characteristically of a shooting type, quickly traveling along the course of the nerve.[7]
Cause
Sciatica is typically caused by irritation of the sciatic nerve.
Spinal disc herniation
Spinal disc herniation pressing on one of the lumbar or sacral nerve roots is the primary cause of sciatica, being present in about 90% of cases.[3]
Sciatica caused by pressure from a disc herniation and swelling of surrounding tissue can spontaneously subside if the tear in the disc heals and the pulposus extrusion and inflammation cease.
Spinal stenosis
Other compressive spinal causes include lumbar spinal stenosis, a condition in which the spinal canal (the spaces the spinal cord runs through) narrows and compresses the spinal cord, cauda equina, or sciatic nerve roots. This narrowing can be caused by bone spurs, spondylolisthesis, inflammation, or a herniated disc, which decreases available space for the spinal cord, thus pinching and irritating nerves from the spinal cord that travel to the sciatic nerves.
Piriformis syndrome
Piriformis syndrome is a controversial condition that, depending on the analysis, varies from a "very rare" cause to contributing to up to 8% of low back or buttock pain.[8] In 17% of the population, the sciatic nerve runs through the piriformis muscle rather than beneath it. When the muscle shortens or spasms due to trauma or overuse, it is posited that this causes compression of the sciatic nerve.[8] It has colloquially been referred to as "wallet sciatica" since a wallet carried in a rear hip pocket compresses the buttock muscles and sciatic nerve when the bearer sits down. Piriformis syndrome causes sciatica when the nerve root is normal.[9][10]
Pregnancy
Sciatica may also occur during pregnancy as a result of the weight of the fetus pressing on the sciatic nerve during sitting or during leg spasms. While most cases do not directly harm the fetus or the mother, indirect harm may come from the numbing effect on the legs, which can cause loss of balance and falling. There is no standard treatment for pregnancy-induced sciatica.[11]
Other
Sciatica can also be caused by tumours impinging on the spinal cord or the nerve roots.[3] Severe back pain extending to the hips and feet, loss of bladder or bowel control, or muscle weakness may result from spinal tumours or cauda equina syndrome. Trauma to the spine, such as from a car accident, may also lead to sciatica.
Pathophysiology
Sciatica is generally caused by the compression of lumbar nerves L4, or L5 or sacral nerves S1, S2, or S3, or by compression of the sciatic nerve itself. When sciatica is caused by compression of a dorsal nerve root (radix), it is considered a lumbar radiculopathy (or radiculitis when accompanied with an inflammatory response). This can occur as a result of a spinal disk bulge or spinal disc herniation (a herniated intervertebral disc), or from roughening, enlarging, or misalignment (spondylolisthesis) of the vertebrae, or as a result of degenerated discs that can reduce the diameter of the lateral foramen (natural hole) through which nerve roots exit the spine. The intervertebral discs consist of an anulus fibrosus, which forms a ring surrounding the inner nucleus pulposus. When there is a tear in the anulus fibrosus, the nucleus pulposus (pulp) may extrude through the tear and press against spinal nerves within the spinal cord, cauda equina, or exiting nerve roots, causing inflammation, numbness, or excruciating pain. Inflammation in the spinal canal can also spread to adjacent facet joints and cause lower back pain and/or referred pain in the posterior thigh(s). Pseudosciatic pain can also be caused by compression of peripheral sections of the nerve, usually from soft tissue tension in the piriformis or related muscles.
The spinal discs are composed of a tough spongiform ring of cartilage ("anulus fibrosus") with a more malleable center ("nucleus pulposus"). The discs separate the vertebrae, thereby allowing room for the nerve roots to properly exit through the spaces between the vertebrae. The discs cushion the spine from compressive forces, but are weak to pressure applied during rotational movements. That is why a person who bends to one side, at a bad angle to pick something up, may more likely herniate a spinal disc than a person jumping from a ladder and landing on their feet.
Herniation of a disc occurs when the liquid center of the disc bulges outwards, tearing the external ring of fibers, extrudes into the spinal canal, and compresses a nerve root against the lamina or pedicle of a vertebra, thus causing sciatica. This extruded liquid from the "nucleus pulposus" may cause inflammation and swelling of surrounding tissue, which may cause further compression of the nerve root in the confined space in the spinal canal.
Diagnosis
Sciatica is typically diagnosed by physical examination, and the history of the symptoms.[3] Generally if a person reports the typical radiating pain in one leg as well as one or more neurological indications of nerve root tension or neurological deficit, sciatica can be diagnosed.[12]
The most applied diagnostic test is the straight leg raise to produce Lasègue's sign, which is considered positive if pain in the distribution of the sciatic nerve is reproduced with between 30 and 70 degrees passive flexion of the straight leg.[13] While this test is positive in about 90% of people with sciatica, approximately 75% of people with a positive test do not have sciatica.[3]
Imaging tests such as computerised tomography or magnetic resonance imaging can help with the diagnosis of lumbar disc herniation.[14] The utility of MR neurography in the diagnoses of piriformis syndrome is controversial.[8]
Management
When the cause of sciatica is lumbar disc herniation, most cases resolve spontaneously over weeks to months.[15] Initially treatment in the first 6–8 weeks should be conservative.[3] There does not appear to be a significant difference in outcomes between advice to stay active and recommendations of bed rest.[16] Similarly, physical therapy (directed exercise) has not been found better than bed rest.[17]
Medication
Although medicines are commonly prescribed for the treatment of sciatica, evidence for pain medication is poor.[18] Specifically, low-quality evidence indicates that NSAIDs do not appear to improve immediate pain and all NSAIDs appear about equivalent.[18] Evidence is also lacking in use of opioids and muscle relaxants by usual means.[18] In those with sciatica due to piriformis syndrome, botulinum toxin injections may improve pain and or function.[19] There is little evidence for steroids, either epidural or by pill.[20][21] Low-quality evidence supports the use of gabapentin for acute pain relief in those with chronic sciatica.[18]
Surgery
Surgery for unilateral sciatica involves the removal of part of the disc, known as a discectomy. While it results in short term benefits, long term benefits appear to be equivalent to conservative care.[3][22] Treatment of the underlying cause of the compression is needed in cases of epidural abscess, epidural tumors, and cauda equina syndrome.
Alternative medicine
Low to moderate-quality evidence suggests that spinal manipulation is an effective treatment for acute sciatica.[2][23] For chronic sciatica, the evidence is poor.[23] Spinal manipulation has been found generally safe for the treatment of disc-related pain; however, case reports have found an association with cauda equina syndrome[24] and it is contraindicated when there are progressive neurological deficits.[25]
Epidemiology
Depending on how it is defined, 2% to 40% of people have sciatica at some point in time.[3] It is most common during peoples 40s and 50s and men are more frequently affected than women.[2][4]
References
- ↑ "Sciatica". Retrieved 2 July 2015.
- 1 2 3 4 5 6 7 8 9 10 Ropper, AH; Zafonte, RD (26 March 2015). "Sciatica.". The New England Journal of Medicine 372 (13): 1240–8. doi:10.1056/NEJMra1410151. PMID 25806916.
- 1 2 3 4 5 6 7 8 9 10 Valat, JP; Genevay, S; Marty, M; Rozenberg, S; Koes, B (April 2010). "Sciatica.". Best practice & research. Clinical rheumatology 24 (2): 241–52. doi:10.1016/j.berh.2009.11.005. PMID 20227645.
- 1 2 3 4 5 6 Institute for Quality and Efficiency in Health Care (October 9, 2014). "Slipped disk: Overview". Retrieved 2 July 2015.
- ↑ Markova, Tsvetio (2007). "Treatment of Acute Sciatica". Am Fam Physician 75 (1): 99–100.
- ↑ Simpson, John (2009). Oxford English dictionary (2nd ed.). Oxford: Oxford University Press. ISBN 0199563837.
- ↑ Bhat, Sriram (2013). SRB's Manual of Surgery. p. 364. ISBN 9789350259443.
- 1 2 3 Miller TA, White KP, Ross DC (September 2012). "The diagnosis and management of Piriformis Syndrome: myths and facts". Can J Neurol Sci 39 (5): 577–83. doi:10.1017/s0317167100015298. PMID 22931697.
- ↑ Kirschner, Jonathan S.; Foye, Patrick M.; Cole, Jeffrey L. (2009). "Piriformis syndrome, diagnosis and treatment". Muscle & Nerve 40 (1): 10–18. doi:10.1002/mus.21318. PMID 19466717.
- ↑ Lewis, A. M.; Layzer, R.; Engstrom, J. W.; Barbaro, N. M.; Chin, C. T. (2006). "Magnetic Resonance Neurography in Extraspinal Sciatica". Archives of Neurology 63 (10): 1469–1472. doi:10.1001/archneur.63.10.1469. PMID 17030664.
- ↑ Sciatic nerve compression during pregnancy
- ↑ Koes, B W; Van Tulder, M W; Peul, W C (2007). "Diagnosis and treatment of sciatica". BMJ 334 (7607): 1313–1317. doi:10.1136/bmj.39223.428495.BE. PMC 1895638. PMID 17585160.
- ↑ Speed, C (May 8, 2004). "Low back pain.". BMJ (Clinical research ed.) 328 (7448): 1119–21. doi:10.1136/bmj.328.7448.1119. PMC 406328. PMID 15130982.
- ↑ Gregory, DS; Seto, CK; Wortley, GC; Shugart, CM (2008). "Acute lumbar disk pain: navigating evaluation and treatment choices". American family physician 78 (7): 835–42. PMID 18841731.
- ↑ Casey, E (February 2011). "Natural history of radiculopathy.". Physical medicine and rehabilitation clinics of North America 22 (1): 1–5. doi:10.1016/j.pmr.2010.10.001. PMID 21292142.
- ↑ Hagen, KB; Hilde, G; Jamtvedt, G; Winnem, M (Oct 18, 2004). "Bed rest for acute low-back pain and sciatica.". Cochrane database of systematic reviews (Online) (4): CD001254. doi:10.1002/14651858.CD001254.pub2. PMID 15495012.
- ↑ Luijsterburg, Pim A. J.; Verhagen, Arianne P.; Ostelo, Raymond W. J. G.; Os, Ton A. G.; Peul, Wilco C.; Koes, Bart W. (2007). "Effectiveness of conservative treatments for the lumbosacral radicular syndrome: a systematic review". European Spine Journal 16 (7): 881–899. doi:10.1007/s00586-007-0367-1. PMC 2219647. PMID 17415595.
- 1 2 3 4 Pinto, RZ; Maher, CG; Ferreira, ML; Ferreira, PH; Hancock, M; Oliveira, VC; McLachlan, AJ; Koes, B (Feb 13, 2012). "Drugs for relief of pain in patients with sciatica: systematic review and meta-analysis.". BMJ (Clinical research ed.) 344: e497. doi:10.1136/bmj.e497. PMC 3278391. PMID 22331277.
- ↑ Waseem, Z; Boulias, C; Gordon, A; Ismail, F; Sheean, G; Furlan, AD (Jan 19, 2011). "Botulinum toxin injections for low-back pain and sciatica.". Cochrane database of systematic reviews (Online) (1): CD008257. doi:10.1002/14651858.CD008257.pub2. PMID 21249702.
- ↑ Balagué, F.; Piguet, V.; Dudler, J. (2012). "Steroids for LBP - from rationale to inconvenient truth.". Swiss Med Wkly 142: w13566. doi:10.4414/smw.2012.13566. PMID 22495738.
- ↑ Chou, R; Hashimoto, R; Friedly, J; Fu, R; Bougatsos, C; Dana, T; Sullivan, SD; Jarvik, J (25 August 2015). "Epidural Corticosteroid Injections for Radiculopathy and Spinal Stenosis: A Systematic Review and Meta-analysis.". Annals of Internal Medicine 163: 373–81. doi:10.7326/M15-0934. PMID 26302454.
- ↑ Bruggeman, AJ; Decker, RC (February 2011). "Surgical treatment and outcomes of lumbar radiculopathy.". Physical medicine and rehabilitation clinics of North America 22 (1): 161–77. doi:10.1016/j.pmr.2010.10.002. PMID 21292152.
- 1 2 Leininger, Brent; Bronfort, Gert; Evans, Roni; Reiter, Todd (2011). "Spinal Manipulation or Mobilization for Radiculopathy: A Systematic Review". Physical Medicine and Rehabilitation Clinics of North America 22 (1): 105–125. doi:10.1016/j.pmr.2010.11.002. PMID 21292148.
- ↑ Tamburrelli, FC; Genitiempo, M; Logroscino, CA (May 2011). "Cauda equina syndrome and spine manipulation: case report and review of the literature.". European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 20 Suppl 1: S128–31. doi:10.1007/s00586-011-1745-2. PMC 3087049. PMID 21404036.
- ↑ WHO guidelines on basic training and safety in chiropractic. "2.1 Absolute contraindications to spinal manipulative therapy", p. 21. WHO
| ||||||||||||||||||||||||||||||