Myocardial infarction
| Myocardial infarction | |
|---|---|
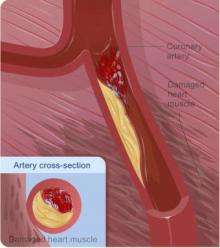
 Diagram of a myocardial infarction (2) of the anterior wall of the heart after blockage (1) of a branch of the left coronary artery (LCA). In the diagram, RCA is the right coronary artery. | |
| Classification and external resources | |
| Specialty | Cardiology |
| ICD-10 | I21-I22 |
| ICD-9-CM | 410 |
| DiseasesDB | 8664 |
| MedlinePlus | 000195 |
| eMedicine | med/1567 emerg/327 ped/2520 |
| Patient UK | Myocardial infarction |
| MeSH | D009203 |
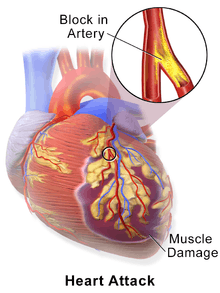
Myocardial infarction (MI) or acute myocardial infarction (AMI), commonly known as a heart attack, occurs when blood flow stops to a part of the heart causing damage to the heart muscle. The most common symptom is chest pain or discomfort which may travel into the shoulder, arm, back, neck, or jaw. Often it is in the center or left side of the chest and lasts for more than a few minutes. The discomfort may occasionally feel like heartburn. Other symptoms may include shortness of breath, nausea, feeling faint, a cold sweat, or feeling tired.[1] About 30% of people have atypical symptoms,[2] with women more likely than men to present atypically.[3] Among those over 75 years old, about 5% have had an MI with little or no history of symptoms.[4] An MI may cause heart failure, an irregular heartbeat, or cardiac arrest.[5][6]
Most MIs occur due to coronary artery disease.[5] Risk factors include high blood pressure, smoking, diabetes, lack of exercise, obesity, high blood cholesterol, poor diet, and excessive alcohol intake, among others.[7][8] The mechanism of an MI often involves the complete blockage of a coronary artery caused by a rupture of an atherosclerotic plaque.[5] MIs are less commonly caused by coronary artery spasms, which may be due to cocaine, significant emotional stress, and extreme cold, among others.[9][10] A number of tests are useful to help with diagnosis, including electrocardiograms (ECGs), blood tests, and coronary angiography.[11] An ECG may confirm an ST elevation MI if ST elevation is present.[2] Commonly used blood tests include troponin and less often creatine kinase MB.[11]
Aspirin is an appropriate immediate treatment for a suspected MI.[12] Nitroglycerin or opioids may be used to help with chest pain; however, they do not improve overall outcomes.[2][12] Supplemental oxygen should be used in those with low oxygen levels or shortness of breath.[12] In ST elevation MIs treatments which attempt to restore blood flow to the heart are typically recommended and include angioplasty, where the arteries are pushed open, or thrombolysis, where the blockage is removed using medications.[2] People who have a non-ST elevation myocardial infarction (NSTEMI) are often managed with the blood thinner heparin, with the additional use angioplasty in those at high risk.[12] In people with blockages of multiple coronary arteries and diabetes, bypass surgery (CABG) may be recommended rather than angioplasty.[13] After an MI, lifestyle modifications, along with long term treatment with aspirin, beta blockers, and statins, are typically recommended.[2]
Worldwide, more than 3 million people have ST elevation MIs and 4 million have NSTEMIs each year.[14] STEMIs occur about twice as often in men as women.[15] About one million people have an MI each year in the United States.[5] In the developed world the risk of death in those who have had an STEMI is about 10%.[2] Rates of MI for a given age have decreased globally between 1990 and 2010.[16]
Signs and symptoms


The onset of symptoms in myocardial infarction (MI) is usually gradual, over several minutes, and rarely instantaneous.[17] Chest pain is the most common symptom of acute MI and is often described as a sensation of tightness, pressure, or squeezing. Chest pain due to ischemia (a lack of blood and hence oxygen supply) of the heart muscle is termed angina pectoris. Pain radiates most often to the left arm, but may also radiate to the lower jaw, neck, right arm, back, and upper abdomen,[18] where it may mimic heartburn. Levine's sign, in which a person localizes the chest pain by clenching their fists over their sternum, has classically been thought to be predictive of cardiac chest pain, although a prospective observational study showed it had a poor positive predictive value.[19]
Shortness of breath (dyspnea) occurs when the damage to the heart limits the output of the left ventricle, causing left ventricular failure and consequent pulmonary edema. Other symptoms include diaphoresis (an excessive form of sweating),[20] weakness, light-headedness, nausea, vomiting, and palpitations. These symptoms are likely induced by a massive surge of catecholamines from the sympathetic nervous system,[21] which occurs in response to pain and the blood flow abnormalities that result from dysfunction of the heart muscle. Loss of consciousness (due to inadequate blood flow to the brain and cardiogenic shock) and sudden death (frequently due to the development of ventricular fibrillation) can occur in MIs.[18]
Atypical symptoms are more frequently reported by women, the elderly, and those with diabetes when compared to their male and younger counterparts.[22][23] Women also report more numerous symptoms compared with men (2.6 on average vs. 1.8 symptoms in men).[22] The most common symptoms of MI in women include dyspnea, weakness, and fatigue. Fatigue, sleep disturbances, and dyspnea have been reported as frequently occurring symptoms that may manifest as long as one month before the actual clinically manifested ischemic event. In women, chest pain may be less predictive of coronary ischemia than in men.[24] Women may also experience back or jaw pain during an episode.[25]
At least one quarter of all MIs are silent, without chest pain or other symptoms.[4] These cases can be discovered later on electrocardiograms, using blood enzyme tests, or at autopsy without a prior history of related complaints. Estimates of the prevalence of silent MIs vary between 22 and 64%.[4] A silent course is more common in the elderly,[4] in people with diabetes mellitus[26] and after heart transplantation, probably because the donor heart is not fully innervated by the nervous system of the recipient.[27] In people with diabetes, differences in pain threshold, autonomic neuropathy, and psychological factors have been cited as possible explanations for the lack of symptoms.[26]
Any group of symptoms compatible with a sudden interruption of the blood flow to the heart, which includes STEMI, NSTEMI or unstable angina, are called an acute coronary syndrome.[28]
Causes
Many of the risk factors for myocardial infarction are modifiable and thus many cases may be preventable.
Lifestyle
Smoking appears to be the cause of about 36% and obesity the cause of 20% of coronary artery disease.[29] Lack of exercise has been linked to 7–12% of cases.[29][30] Less common causes include stress-related causes such as job stress, which accounts for about 3% of cases,[29] and chronic high stress levels.[31]
Tobacco smoking (including secondhand smoke)[32] and short-term exposure to air pollution such as carbon monoxide, nitrogen dioxide, and sulfur dioxide (but not ozone) have been associated with MI.[33] Other factors that increase the risk of MI and are associated with worse outcomes after an MI include lack of physical activity[34] and psychosocial factors including low socioeconomic status, social isolation, and negative emotions. Shift work is also associated with a higher risk of MI.[35] Acute and prolonged intake of high quantities of alcoholic drinks (3-4 or more) increase the risk of a heart attack.[36]
The evidence for saturated fat is unclear. Some state there is evidence of benefit from reducing saturated fat,[37] specifically a benefit from eating polyunsaturated fat instead of saturated fat.[38] While others state there is little evidence that reducing dietary saturated fat or increasing polyunsaturated fat intake affects heart attack risk.[39][40] Dietary cholesterol does not appear to have a significant effect on blood cholesterol and thus recommendations about its consumption may not be needed.[41] Trans fats do appear to increase risk.[39]
Disease
Diabetes mellitus (type 1 or 2),[42] high blood pressure,[32] dyslipidemia/high levels of blood cholesterol (abnormal levels of lipoproteins in the blood), particularly high low-density lipoprotein, low high-density lipoprotein, high triglycerides,[32] and obesity[43] (defined by a body mass index of more than 30 kg/m², or alternatively by waist circumference or waist-hip ratio) have all been linked to MI.
A number of acute and chronic infections including Chlamydophila pneumoniae, influenza, Helicobacter pylori, and Porphyromonas gingivalis among others have been linked to atherosclerosis and myocardial infarction.[44] As of 2013, there is no evidence of benefit from antibiotics or vaccination, however, calling the association into question.[44][45] Myocardial infarction can also occur as a late consequence of Kawasaki disease.[46]
Genetic
Genome-wide association studies have found 27 genetic variants that are associated with an increased risk of myocardial infarction.[47] Strongest association of MI has been found with the 9p21 genomic locus, which contains genes CDKN2A & 2B, although the single nucleotide polymorphisms that are implicated are within a non-coding region.[47] The majority of these variants are in regions that have not been previously implicated in coronary artery disease. The following genes have an association with MI: PCSK9, SORT1, MIA3, WDR12, MRAS, PHACTR1, LPA, TCF21, MTHFDSL, ZC3HC1, CDKN2A, 2B, ABO, PDGF0, APOA5, MNF1ASM283, COL4A1, HHIPC1, SMAD3, ADAMTS7, RAS1, SMG6, SNF8, LDLR, SLC5A3, MRPS6, KCNE2.[47]
Other
At any given age, men are more at risk than women, particularly before menopause,[48] but because in general women live longer than men, ischemic heart disease causes slightly more total deaths in women.[34] Family history of ischemic heart disease or MI, particularly if one has a first-degree relative (father, brother, mother, sister) who suffered a 'premature' myocardial infarction (defined as occurring at or younger than age 55 years (men) or 65 (women)).[34]
Women who use combined oral contraceptive pills have a modestly increased risk of myocardial infarction, especially in the presence of other risk factors, such as smoking.[49] Heart attacks appear to occur more commonly in the morning hours, especially between 6AM and noon.[50] Evidence suggests that heart attacks are at least three times more likely to occur in the morning than in the late evening.[51] Old age increases risk of a heart attack.[34]
Pathophysiology


Acute myocardial infarction refers to two subtypes of acute coronary syndrome, namely non-ST-elevated and ST-elevated MIs, which are most frequently (but not always) a manifestation of coronary artery disease.[52] The most common triggering event is the disruption of an atherosclerotic plaque in an epicardial coronary artery, which leads to a clotting cascade, sometimes resulting in total occlusion of the artery.[53][54] Atherosclerosis is the gradual buildup of cholesterol and fibrous tissue in plaques in the wall of arteries (in this case, the coronary arteries), typically over decades.[55] Bloodstream column irregularities visible on angiography reflect artery lumen narrowing as a result of decades of advancing atherosclerosis.[56] Plaques can become unstable, rupture, and additionally promote the formation of a blood clot that occludes the artery; this can occur in minutes. When a severe enough plaque rupture occurs in the coronary arteries, it leads to MI (necrosis of downstream myocardium).[53][54] It is estimated that one billion cardiac cells are lost in a typical MI.[57]
If impaired blood flow to the heart lasts long enough, it triggers a process called the ischemic cascade; the heart cells in the territory of the occluded coronary artery die (chiefly through necrosis) and do not grow back. A collagen scar forms in their place. Recent studies indicate that another form of cell death, apoptosis, also plays a role in the process of tissue damage following an MI.[58] As a result, the person's heart will be permanently damaged. This myocardial scarring also puts the person at risk for potentially life-threatening abnormal heart rhythms (arrhythmias), and may result in the formation of a ventricular aneurysm that can rupture with catastrophic consequences.
Injured heart tissue conducts electrical impulses more slowly than normal heart tissue. The difference in conduction velocity between injured and uninjured tissue can trigger re-entry or a feedback loop that is believed to be the cause of many lethal arrhythmias. The most serious of these arrhythmias is ventricular fibrillation (V-Fib/VF), an extremely fast and chaotic heart rhythm that is the leading cause of sudden cardiac death. Another life-threatening arrhythmia is ventricular tachycardia (V-tach/VT), which can cause sudden cardiac death. However, VT usually results in rapid heart rates that prevent the heart from pumping blood effectively. Cardiac output and blood pressure may fall to dangerous levels, which can lead to further coronary ischemia and extension of the infarct.
The cardiac defibrillator device was specifically designed to terminate these potentially fatal arrhythmias. The device works by delivering an electrical shock to the person to depolarize a critical mass of the heart muscle, in effect "rebooting" the heart. This therapy is time-dependent, and the odds of successful defibrillation decline rapidly after the onset of cardiopulmonary arrest.
Myocardial infarction in the setting of plaque results from underlying atherosclerosis.[18] Inflammation is known to be an important step in the process of atherosclerotic plaque formation.[59] C-reactive protein (CRP) is a sensitive but nonspecific marker for inflammation. Elevated CRP blood levels, especially measured with high-sensitivity assays, can predict the risk of MI, as well as stroke and development of diabetes.[59] Moreover, some drugs for MI might also reduce CRP levels.[59] The use of high-sensitivity CRP assays as a means of screening the general population is advised against, but it may be used optionally at the physician's discretion in those who already present with other risk factors or known coronary artery disease.[60] Whether CRP plays a direct role in atherosclerosis remains uncertain.[59]
Calcium deposition is another part of atherosclerotic plaque formation. Calcium deposits in the coronary arteries can be detected with CT scans. Several studies have shown that coronary calcium can provide predictive information beyond that of classical risk factors.[61][62][63]
Hyperhomocysteinemia (high blood levels of the amino acid homocysteine) in homocysteinuria is associated with premature atherosclerosis;[64] whether elevated homocysteine in the normal range is causal is controversial.[65]
Pathological types
The two main types of acute myocardial infarction, based on pathology, are:
- Transmural AMI is associated with atherosclerosis involving a major coronary artery. It can be subclassified into anterior, posterior, inferior, lateral, or septal. Transmural infarcts extend through the whole thickness of the heart muscle and are usually a result of complete occlusion of the area's blood supply.[66] In addition, on ECG, ST elevation and Q waves are seen.
- Subendocardial AMI involves a small area in the subendocardial wall of the left ventricle, ventricular septum, or papillary muscles. The subendocardial area is particularly susceptible to ischemia.[66] In addition, ST depression may be seen on ECG in addition to T wave changes.
Diagnosis


A cardiac troponin rise accompanied by either typical symptoms, pathological Q waves, ST elevation or depression, or coronary intervention is diagnostic of MI.[67]
WHO criteria[68] formulated in 1979 have classically been used to diagnose MI; a patient is diagnosed with MI if two (probable) or three (definite) of the following criteria are satisfied:
- Clinical history of ischemic type chest pain lasting for more than 20 minutes
- Changes in serial ECG tracings
- Rise and fall of serum cardiac biomarkers
At autopsy, a pathologist can diagnose an MI based on anatomopathological findings.
Classification
Myocardial infarctions are generally classified into ST elevation MI (STEMI) and non-ST elevation MI (NSTEMI).[52] A STEMI is the combination of symptoms related to poor oxygenation of the heart with elevation of the ST segments on the electrocardiogram followed by an increase in proteins in the blood related to heart muscle's death.[15] They make up about 25 to 40 percent of cases.[15]
The phrase "heart attack" is often used non-specifically to refer to a myocardial infarction and to sudden cardiac death. An MI is different from—but can cause—cardiac arrest, where the heart is not contracting at all or so poorly that all vital organs cease to function. It is also distinct from heart failure, in which the pumping action of the heart is impaired. However, an MI may lead to heart failure.[18]
A 2007 consensus document classifies MI into five main types:[69]
- Type 1 – spontaneous MI related to ischemia due to a primary coronary event such as plaque erosion and/or rupture, fissuring, or dissection
- Type 2 – MI secondary to ischemia due to either increased oxygen demand or decreased supply, e.g. coronary artery spasm, coronary embolism, anemia, arrhythmias, hypertension, or hypotension
- Type 3 – sudden unexpected cardiac death, including cardiac arrest, often with symptoms suggestive of myocardial ischemia, accompanied by new ST elevation, or new left bundle branch block (LBBB), or evidence of fresh thrombus in a coronary artery by angiography and/or at autopsy, but death occurring before blood samples could be obtained, or at a time before the appearance of cardiac biomarkers in the blood
- Type 4 – associated with coronary angioplasty or stents:
- Type 4a – MI associated with percutaneous coronary intervention (PCI)
- Type 4b – MI associated with stent thrombosis as documented by angiography or at autopsy
- Type 5 – MI associated with CABG
The terms Q wave and non-Q wave MI were previously used to indicate STEMI and non-STEMI respectively.[70]
Electrocardiogram
For a person to qualify as having a STEMI, in addition to reported angina, the ECG must show new ST elevation in two or more adjacent ECG leads.[15] This must be greater than 2 mm (0.2 mV) for males and greater than 1.5 mm (0.15mV) in females if in leads V2 and V3 or greater than 1 mm (0.1 mV) if it is in other ECG leads.[15] A left bundle branch block that is believed to be new used to be considered the same as ST elevation; however, this is no longer the case.[15] In early STEMIs there may just be peaked T waves with ST elevation developing later.[15]
Cardiac biomarkers
While there are a number of different biomarkers, troponins are considered to be the best[15] and reliance on older tests (such as CK-MB) or myoglobin is discouraged.[71] This is not the case in the setting of peri-procedural MI where use of troponin and CK-MB assays are considered useful.[72] Copeptin may be useful to rule out MI rapidly when used along with troponin.[73]
Imaging
A chest radiograph and routine blood tests may indicate complications or precipitating causes, and are often performed upon arrival to an emergency department.
In stable patients whose symptoms have resolved by the time of evaluation, technetium (99mTc) sestamibi (i.e. a "MIBI scan") or thallium-201 chloride can be used in nuclear medicine to visualize areas of reduced blood flow in conjunction with physiological or pharmacological stress. Thallium may also be used to determine viability of tissue, distinguishing whether nonfunctional myocardium is actually dead or merely in a state of hibernation or of being stunned.[74] Medical societies and professional guidelines recommend that the physician confirm a person is at high risk for myocardial infarction before conducting imaging tests to make a diagnosis.[75][76] Patients who have a normal ECG and who are able to exercise, for example, do not merit routine imaging.[76] Imaging tests such as stress radionuclide myocardial perfusion imaging or stress echocardiography can confirm a diagnosis when a patient's history, physical exam, ECG, and cardiac biomarkers suggest the likelihood of a problem.[76]
Differential diagnosis
The differential diagnosis for MI includes other catastrophic causes of chest pain, such as pulmonary embolism, aortic dissection, esophageal rupture, tension pneumothorax, or pericardial effusion causing cardiac tamponade. Other noncatastrophic differentials include gastroesophageal reflux and Tietze's syndrome.[77]
Prevention
Myocardial infarction and other related cardiovascular diseases can be prevented to a large extent by a number of lifestyle changes and medical treatments.
Lifestyle
Recommendations include increasing the intake of wholegrain starch, reducing sugar intake (particularly of refined sugar), consuming five portions of fruit and vegetables daily, consuming two or more portions of fish per week, and consuming 4–5 portions of unsalted nuts, seeds, or legumes per week.[78] The dietary pattern with the greatest support is the Mediterranean diet.[79] Vitamins and mineral supplements are of no proven benefit,[80] and neither are plant stanols or sterols.[78]
There is some controversy surrounding the effect of dietary fat on the development of cardiovascular disease. People are often advised to keep a diet where less than 30% of the energy intake derives from fat, a diet that contains less than 7% of the energy intake in the form of saturated fat, and a diet that contains less than 300 mg/day of cholesterol.[78] Replacing saturated with mono- polyunsaturated fat is also recommended,[78] as the consumption of polyunsaturated fat instead of saturated fat may decrease coronary heart disease.[81] Olive oil, rapeseed oil and related products are to be used instead of saturated fat.[78]
Physical activity can reduce the risk of cardiovascular disease, and people at risk are advised to engage in 150 minutes of moderate or 75 minutes of vigorous intensity aerobic exercise a week.[78] Keeping a healthy weight, drinking alcohol within the recommended limits, and quitting smoking are measures that also appear to reduce the risk of cardiovascular disease.[78]
On a population level, public health measures may be used to reduce unhealthy diets (excessive salt, saturated fat and trans fat) including food labelling and marketing requirements as well as requirements for catering and restaurants, and stimulating physical activity. This may be part of regional cardiovascular disease prevention programmes, or through the health impact assessment of regional and local plans and policies.[82]
Medication
Aspirin has been studied extensively in people considered at increased risk of myocardial infarction. Based on numerous studies in different groups (e.g. people with or without diabetes), there does not appear to be a benefit strong enough to outweigh the risk of excessive bleeding.[83][84] Nevertheless, many clinical practice guidelines continue to recommend aspirin for primary prevention,[85] and some researchers feel that those with very high cardiovascular risk but low risk of bleeding should continue to receive aspirin.[86]
Cholesterol-lowering drugs from the statin class may be used in those at an elevated risk of cardiovascular disease; this can be calculated with validated risk prediction tools such as QRISK2.[78]
Long term hormone replacement therapy when started around the time of menopause may decrease heart disease.[87][88]
Following a heart attack, nitrates, when taken for two days, and ACE-inhibitors decrease the risk of death.[89]
Management
An MI requires immediate medical attention. Treatment attempts to save as much viable heart muscle as possible and to prevent further complications, hence the phrase "time is [heart] muscle".[90] Aspirin and nitroglycerin may be administered. Nitroglycerin (administered under the tongue or intravenously) may be administered to improve the blood supply to the heart.[71] Morphine may be used if nitroglycerin is not effective.[71] Other analgesics such as nitrous oxide are of unknown benefit.[91]
In the past, high flow oxygen was recommended for everyone with possible myocardial infarction.[71] More recently, routine use was found to lead to increased mortality and infarct size.[92][93] Therefore, oxygen is currently only used if oxygen levels are found to be low or someone is in respiratory distress.[71] A 2015 meta-analysis concluded that the use of an intra-aortic balloon pump during an acute MI with or without cardiogenic shock does not reduce mortality.[94]
STEMI
The main treatment for MI with ECG evidence of ST elevation (STEMI) include thrombolysis and percutaneous coronary intervention.[95] Primary percutaneous coronary intervention (PCI) is the treatment of choice for STEMI if it can be performed in a timely manner.[95][96] If PCI cannot be performed within 90 to 120 minutes then thrombolysis, preferably within 30 minutes of arrival to hospital, is recommended.[96][97][98] If a person has had symptoms for 12 to 24 hours evidence for thrombolysis is less and if they have had symptoms for more than 24 hours it is not recommended.[99]
Thrombolysis involves the administration of medication that activates the enzymes that normally destroy blood clots. Thrombolysis agents include streptokinase, reteplase, alteplase, and tenecteplase. If no contraindications are present (such as a high risk of bleeding), thrombolysis can be given in the pre-hospital or in-hospital setting. When given to people suspected of having a STEMI within 6 hours of the onset of symptoms, thrombolytic drugs save the life of 1 in 43 who received them. The risks were major bleeding (1 in 143) and brain bleeding (1 in 250).[100][101] It is unclear whether pre-hospital thrombolysis reduces death in people with STEMI compared to in-hospital thrombolysis.[102] Pre-hospital thrombolysis reduces time to thrombolytic treatment, based on studies conducted in higher income countries.[102]
If despite thrombolysis there is significant cardiogenic shock, continued severe chest pain, or less than a 50% improvement in ST elevation on the ECG recording after 90 minutes, then rescue PCI is indicated emergently.[97][103] After PCI, people are generally placed on dual antiplatelet therapy for at least a year (which is generally aspirin and clopidogrel).[15][95][104]
When beta blocker medication are given within the first 24–72 hours of a major heart attack (“STEMI”) no lives are saved. However, 1 in 200 people were prevented from a repeat heart attack, and another 1 in 200 from having an abnormal heart rhythm. Additionally, for 1 in 91 the drug causes a temporary poor ability of the heart to pump blood.[105]
Those who have had cardiac arrest may benefit from targeted temperature management with evaluation for implementation of hypothermia protocols. Furthermore, those with cardiac arrest, and ST elevation at any time, should usually have angiography.[106]
NSTEMI
In the absence of ST elevation, diagnosis of MI is based on a blood test for biomarkers (usually troponin). This can take 3–6 hours after the onset of symptoms to become positive. The scenario is referred to as "non-ST elevation acute coronary syndrome" (NSTEACS). In the meantime, the calculated risk of further cardiovascular events (e.g. using the GRACE score) and the presence of other ECG changes and clinical features determines ongoing management.[71][75]
People with an acute coronary syndrome where no ST elevation is demonstrated (non-ST elevation ACS or NSTEACS) are treated with aspirin.[71][75] Clopidogrel is added in many cases, particularly if the risk of cardiovascular events is felt to be high and early PCI is being considered.[71][75] Depending on whether early PCI is planned, a factor Xa inhibitor or a potentiator of antithrombin (fondaparinux or low molecular weight heparin respectively) may be added.[75] In very high-risk scenarios, inhibitors of the platelet glycoprotein αIIbβ3a receptor such as eptifibatide or tirofiban may be used.[71][75]
Heparins in those who have had an NSTEMI or unstable angina do not change the risk of death.[107] They do decrease the risk of having a further myocardial infarction.[107]
As of 2011, P2Y12 inhibitors are recommended for 12 months following NSTEMI in Europe.[108] A 2014 review of P2Y12 inhibitors such as clopidogrel found they do not change the risk of death when given to people with a suspected NSTEMI prior to PCI. They do however increase the risk of bleeding and decrease the risk of further cardiovascular problems. The authors thus concluded that their routine use prior to PCI is of questionable value.[109]
Cardiac rehabilitation
Cardiac rehabilitation benefits many who have experienced myocardial infarction, even if there has been substantial heart damage and resultant left ventricular failure; ideally other medical conditions that could interfere with participation should be managed optimally. It should start soon after discharge from hospital. The program may include lifestyle advice, exercise, social support, as well as recommendations about driving, flying, sport participation, stress management, and sexual intercourse.[110]
Secondary prevention
A number of lifestyle recommendations are available to those who have experienced myocardial infarction. This includes the adoption of a Mediterranean-type diet, maintaining alcohol intake within recommended limits, exercising to the point of mild breathlessness for 20–30 minutes every day, stopping smoking, and trying to achieve a healthy weight.[110] Exercise is both safe and effective even if people have had stents or heart failure.[111]
People are usually started on several long-term medications after an MI, with the aim of preventing further cardiovascular events such as MIs, congestive heart failure, or strokes.
- Aspirin as well as another antiplatelet agent such as clopidogrel or ticagrelor ("dual antiplatelet therapy" or DAPT) is continued for up to twelve months, followed by aspirin indefinitely.[110] If someone has another medical condition that requires anticoagulation (e.g. with warfarin) this may need to be adjusted based on risk of further cardiac events as well as bleeding risk.[110] In those who have had a stent, more than 12 months of clopidogrel plus aspirin does not affect the risk of death.[112]
- Beta blocker therapy such as metoprolol or carvedilol is recommended to be started within 24 hours, provided there is no acute heart failure or heart block.[15][71][110] The dose should be increased to the highest tolerated.[110] Contrary to what was long believed, the use of beta blockers does not appear to affect the risk of death, possibly because other treatments for MI have improved.[113] They should not be used in those who have recently taken cocaine.[114]
- ACE inhibitor therapy should be started when stable and continued indefinitely at the highest tolerated dose. Those who cannot tolerate ACE inhibitors may be treated with an angiotensin II receptor antagonist.[110]
- Statin therapy has been shown to reduce mortality and morbidity.[115] The protective effects of statins may be due to more than their LDL lowering effects. The general consensus is that statins have the ability to stabilize plaques and multiple other ("pleiotropic") effects that may prevent myocardial infarction in addition to their effects on blood lipids.[116]
- Aldosterone antagonists (spironolactone or eplerenone) may be used if there is evidence of left ventricular dysfunction after an MI, ideally after beginning treatment with an ACE inhibitor.[110]
- Previous studies suggested a benefit from omega-3 fatty acid supplementation but this has not been confirmed.[110]
Prognosis
The prognosis after MI varies greatly depending on a person's health, the extent of the heart damage, and the treatment given.
In those who have an STEMI in the United States, between 5 to 6 percent die before leaving the hospital and 7 to 18 percent die within a year.[15]
Using variables available in the emergency room, people with a higher risk of adverse outcome can be identified. One study found 0.4% of patients with a low-risk profile died after 90 days, whereas in high-risk people it was 21.1%.[117]
Some risk factors for death include age, hemodynamic parameters (such as heart failure, cardiac arrest on admission, systolic blood pressure, or Killip class of two or greater), ST-segment deviation, diabetes, serum creatinine, peripheral vascular disease, and elevation of cardiac markers.[117][118][119] Assessment of left ventricular ejection fraction may increase the predictive power.[120] Prognosis is worse if a mechanical complication such as papillary muscle or myocardial free wall rupture occurs.[121] Morbidity and mortality from myocardial infarction has improved over the years due to better treatment.[122]
Throughout hospital departments, practitioners use TIMI scores to assess mortality risk. There are TIMI (Thrombolysis in Myocardial Infarction) scores for unstable angina or NSTEMI[123] and STEMI,[124] both using routine patient data from history taking, medication use and lab results. Both scores have been found effective and reliable in multiple settings, including the emergency room.
Complications
Complications may occur immediately following the heart attack (in the acute phase), or may need time to develop (a chronic problem). Acute complications may include heart failure if the damaged heart is no longer able to pump blood adequately around the body; aneurysm of the left ventricle myocardium; ventricular septal rupture or free wall rupture; mitral regurgitation, in particular if the infarction causes dysfunction of the papillary muscle; Dressler's syndrome; and abnormal heart rhythms, such as ventricular fibrillation, ventricular tachycardia, atrial fibrillation, and heart block. Longer-term complications include heart failure, atrial fibrillation, and an increased risk of a second MI.
Epidemiology
Myocardial infarction is a common presentation of coronary artery disease. The World Health Organization estimated in 2004, that 12.2% of worldwide deaths were from ischemic heart disease;[125] with it being the leading cause of death in high- or middle-income countries and second only to lower respiratory infections in lower-income countries.[125] Worldwide, more than 3 million people have STEMIs and 4 million have NSTEMIs a year.[14] STEMIs occur about twice as often in men as women.[15]
Rates of death from ischemic heart disease (IHD) have slowed or declined in most high-income countries, although cardiovascular disease still accounted for one in three of all deaths in the USA in 2008.[126] For example, rates of death from cardiovascular disease have decreased almost a third between 2001 and 2011 in the United States.[127]
In contrast, IHD is becoming a more common cause of death in the developing world. For example, in India, IHD had become the leading cause of death by 2004, accounting for 1.46 million deaths (14% of total deaths) and deaths due to IHD were expected to double during 1985–2015.[128] Globally, disability adjusted life years (DALYs) lost to ischemic heart disease are predicted to account for 5.5% of total DALYs in 2030, making it the second-most-important cause of disability (after unipolar depressive disorder), as well as the leading cause of death by this date.[125]
Society and culture
In the United States, women who have had an MI are often treated with fewer medical interventions than men.[15]
Economics
In 2011, AMI was one of the top five most expensive conditions seen during inpatient hospitalizations in the U.S., with an aggregate cost of about $11.5 billion for 612,000 hospital stays.[129]
Legal implications
At common law, in general, a myocardial infarction is a disease, but may sometimes be an injury. This can create coverage issues in administration of no-fault insurance schemes such as workers' compensation. In general, a heart attack is not covered;[130] however, it may be a work-related injury if it results, for example, from unusual emotional stress or unusual exertion.[131] In addition, in some jurisdictions, heart attacks suffered by persons in particular occupations such as police officers may be classified as line-of-duty injuries by statute or policy. In some countries or states, a person having suffered from an MI may be prevented from participating in activity that puts other people's lives at risk, for example driving a car or flying an airplane.[132]
Etymology
Myocardial infarction Latin: infarctus myocardii.
References
- ↑ "What Are the Signs and Symptoms of Coronary Heart Disease?". http://www.nhlbi.nih.gov/. September 29, 2014. Retrieved 23 February 2015. External link in
|website=(help) - 1 2 3 4 5 6 Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology, (ESC); Steg, PG; James, SK; Atar, D; Badano, LP; Blömstrom-Lundqvist, C; Borger, MA; Di Mario, C; Dickstein, K; Ducrocq, G; Fernandez-Aviles, F; Gershlick, AH; Giannuzzi, P; Halvorsen, S; Huber, K; Juni, P; Kastrati, A; Knuuti, J; Lenzen, MJ; Mahaffey, KW; Valgimigli, M; van 't Hof, A; Widimsky, P; Zahger, D (October 2012). "ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation.". European Heart Journal 33 (20): 2569–619. doi:10.1093/eurheartj/ehs215. PMID 22922416.
- ↑ Coventry, LL; Finn, J; Bremner, AP (2011). "Sex differences in symptom presentation in acute myocardial infarction: a systematic review and meta-analysis.". Heart & lung : the journal of critical care 40 (6): 477–91. doi:10.1016/j.hrtlng.2011.05.001. PMID 22000678.
- 1 2 3 4 Valensi P, Lorgis L, Cottin Y; Lorgis; Cottin (March 2011). "Prevalence, incidence, predictive factors and prognosis of silent myocardial infarction: a review of the literature". Arch Cardiovasc Dis 104 (3): 178–88. doi:10.1016/j.acvd.2010.11.013. PMID 21497307.
- 1 2 3 4 "What Is a Heart Attack?". http://www.nhlbi.nih.gov/. December 17, 2013. Retrieved 24 February 2015. External link in
|website=(help) - ↑ "Heart Attack or Sudden Cardiac Arrest: How Are They Different?". http://www.heart.org/. Jul 30, 2014. Retrieved 24 February 2015. External link in
|website=(help) - ↑ Mehta, PK; Wei, J; Wenger, NK (16 October 2014). "Ischemic heart disease in women: A focus on risk factors.". Trends in Cardiovascular Medicine 25 (2): 140–151. doi:10.1016/j.tcm.2014.10.005. PMID 25453985.
- ↑ Mendis, Shanthi; Puska,, Pekka; Norrving, Bo (2011). Global atlas on cardiovascular disease prevention and control (PDF) (1st ed.). Geneva: World Health Organization in collaboration with the World Heart Federation and the World Stroke Organization. pp. 3–18. ISBN 9789241564373. Missing
|last1=in Authors list (help) - ↑ "What Causes a Heart Attack?". http://www.nhlbi.nih.gov. December 17, 2013. Retrieved 24 February 2015. External link in
|website=(help) - ↑ Devlin, RJ; Henry, JA (2008). "Clinical review: Major consequences of illicit drug consumption.". Critical care (London, England) 12 (1): 202. doi:10.1186/cc6166. PMC 2374627. PMID 18279535.
- 1 2 "How Is a Heart Attack Diagnosed?". http://www.nhlbi.nih.gov/. December 17, 2013. Retrieved 24 February 2015. External link in
|website=(help) - 1 2 3 4 O'Connor, RE; Brady, W; Brooks, SC; Diercks, D; Egan, J; Ghaemmaghami, C; Menon, V; O'Neil, BJ; Travers, AH; Yannopoulos, D (2 November 2010). "Part 10: acute coronary syndromes: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.". Circulation 122 (18 Suppl 3): S787–817. doi:10.1161/CIRCULATIONAHA.110.971028. PMID 20956226.
- ↑ Hamm CW, Bassand JP, Agewall S, Bax J, Boersma E, Bueno H, Caso P, Dudek D, Gielen S, Huber K, Ohman M, Petrie MC, Sonntag F, Uva MS, Storey RF, Wijns W, Zahger D (December 2011). "ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC)". Eur. Heart J. 32 (23): 2999–3054. doi:10.1093/eurheartj/ehr236. PMID 21873419.
- 1 2 White HD, Chew DP; Chew (August 2008). "Acute myocardial infarction". Lancet 372 (9638): 570–84. doi:10.1016/S0140-6736(08)61237-4. PMID 18707987.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 O'Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX, Anderson JL, Jacobs AK, Halperin JL, Albert NM, Brindis RG, Creager MA, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Kushner FG, Ohman EM, Stevenson WG, Yancy CW (Jan 29, 2013). "2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.". Circulation 127 (4): e362–425. doi:10.1161/CIR.0b013e3182742cf6. PMID 23247304.
- ↑ Moran, AE; Forouzanfar, MH; Roth, GA; Mensah, GA; Ezzati, M; Flaxman, A; Murray, CJ; Naghavi, M (8 April 2014). "The global burden of ischemic heart disease in 1990 and 2010: the Global Burden of Disease 2010 study.". Circulation 129 (14): 1493–501. doi:10.1161/circulationaha.113.004046. PMID 24573351.
- ↑ National Heart, Lung and Blood Institute. Heart Attack Warning Signs. Retrieved November 22, 2006.
- 1 2 3 4 Van de Werf F, Bax J, Betriu A, Blomstrom-Lundqvist C, Crea F, Falk V, Filippatos G, Fox K, Huber K, Kastrati A, Rosengren A, Steg PG, Tubaro M, Verheugt F, Weidinger F, Weis M (December 2008). "Management of acute myocardial infarction in patients presenting with persistent ST-segment elevation: the Task Force on the Management of ST-Segment Elevation Acute Myocardial Infarction of the European Society of Cardiology". Eur. Heart J. 29 (23): 2909–45. doi:10.1093/eurheartj/ehn416. PMID 19004841.
- ↑ Marcus GM, Cohen J, Varosy PD, Vessey J, Rose E, Massie BM, Chatterjee K, Waters D (2007). "The utility of gestures in patients with chest discomfort". Am. J. Med. 120 (1): 83–9. doi:10.1016/j.amjmed.2006.05.045. PMID 17208083.
- ↑ Mallinson, T (2010). "Myocardial Infarction". Focus on First Aid (15): 15. Archived from the original on May 21, 2010. Retrieved 2010-06-08.
- ↑ Little RA, Frayn KN, Randall PE, Stoner HB, Morton C, Yates DW, Laing GS (1986). "Plasma catecholamines in the acute phase of the response to myocardial infarction". Arch Emerg Med 3 (1): 20–7. doi:10.1136/emj.3.1.20. PMC 1285314. PMID 3524599.
- 1 2 Canto JG, Goldberg RJ, Hand MM, Bonow RO, Sopko G, Pepine CJ, Long T (December 2007). "Symptom presentation of women with acute coronary syndromes: myth vs reality". Arch. Intern. Med. 167 (22): 2405–13. doi:10.1001/archinte.167.22.2405. PMID 18071161.
- ↑ Brown, Anthony (2011). Emergency Medicine Diagnosis and Management 6th Edition.
- ↑ McSweeney JC, Cody M, O'Sullivan P, Elberson K, Moser DK, Garvin BJ (2003). "Women's early warning symptoms of acute myocardial infarction". Circulation 108 (21): 2619–23. doi:10.1161/01.CIR.0000097116.29625.7C. PMID 14597589.
- ↑ http://feministing.com/2012/02/23/for-women-heart-attacks-look-different-and-so-do-heart-health-outcomes/
- 1 2 Davis TM, Fortun P, Mulder J, Davis WA, Bruce DG (2004). "Silent myocardial infarction and its prognosis in a community-based cohort of Type 2 diabetic patients: the Fremantle Diabetes Study". Diabetologia 47 (3): 395–9. doi:10.1007/s00125-004-1344-4. PMID 14963648.
- ↑ Rubin, Emanuel; Gorstein, Fred; Rubin, Raphael; Schwarting, Roland; Strayer, David (2001). Rubin's Pathology — Clinicopathological Foundations of Medicine. Maryland: Lippincott Williams & Wilkins. p. 549. ISBN 0-7817-4733-3.
- ↑ Acute Coronary Syndrome. American Heart Association. Retrieved November 25, 2006. Archived September 25, 2006 at the Wayback Machine
- 1 2 3 Kivimäki M, Nyberg ST, Batty GD, Fransson EI, Heikkilä K, Alfredsson L, Bjorner JB, Borritz M, Burr H, Casini A, Clays E, De Bacquer D, Dragano N, Ferrie JE, Geuskens GA, Goldberg M, Hamer M, Hooftman WE, Houtman IL, Joensuu M, Jokela M, Kittel F, Knutsson A, Koskenvuo M, Koskinen A, Kouvonen A, Kumari M, Madsen IE, Marmot MG, Nielsen ML, Nordin M, Oksanen T, Pentti J, Rugulies R, Salo P, Siegrist J, Singh-Manoux A, Suominen SB, Väänänen A, Vahtera J, Virtanen M, Westerholm PJ, Westerlund H, Zins M, Steptoe A, Theorell T (31 August 2012). "Job strain as a risk factor for coronary heart disease: a collaborative meta-analysis of individual participant data". The Lancet 380 (9852): 1491–7. doi:10.1016/S0140-6736(12)60994-5. PMC 3486012. PMID 22981903.
- ↑ Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT (1 July 2012). "Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy". The Lancet 380 (9838): 219–29. doi:10.1016/S0140-6736(12)61031-9. PMC 3645500. PMID 22818936.
- ↑ Steptoe A, Kivimäki M (April 2012). "Stress and cardiovascular disease". Nature Reviews Cardiology 9 (6): 360–70. doi:10.1038/nrcardio.2012.45. PMID 22473079.
- 1 2 3 Smith SC, Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, Grundy SM, Hiratzka L, Jones D, Krumholz HM, Mosca L, Pearson T, Pfeffer MA, Taubert KA (May 2006). "AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update endorsed by the National Heart, Lung, and Blood Institute". J. Am. Coll. Cardiol. 47 (10): 2130–9. doi:10.1016/j.jacc.2006.04.026. PMID 16697342.
- ↑ Mustafic H, Jabre P, Caussin C, Murad MH, Escolano S, Tafflet M, Périer MC, Marijon E, Vernerey D, Empana JP, Jouven X (Feb 15, 2012). "Main air pollutants and myocardial infarction: a systematic review and meta-analysis". JAMA: the Journal of the American Medical Association 307 (7): 713–21. doi:10.1001/jama.2012.126. PMID 22337682.
- 1 2 3 4 Graham I, Atar D, Borch-Johnsen K, Boysen G, Burell G, Cifkova R, Dallongeville J, De Backer G, Ebrahim S, Gjelsvik B, Herrmann-Lingen C, Hoes A, Humphries S, Knapton M, Perk J, Priori SG, Pyorala K, Reiner Z, Ruilope L, Sans-Menendez S, Scholte op Reimer W, Weissberg P, Wood D, Yarnell J, Zamorano JL, Walma E, Fitzgerald T, Cooney MT, Dudina A (October 2007). "European guidelines on cardiovascular disease prevention in clinical practice: executive summary: Fourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (Constituted by representatives of nine societies and by invited experts)". Eur. Heart J. 28 (19): 2375–414. doi:10.1093/eurheartj/ehm316. PMID 17726041.
- ↑ Vyas MV, Garg AX, Iansavichus AV, Costella J, Donner A, Laugsand LE, Janszky I, Mrkobrada M, Parraga G, Hackam DG (July 2012). "Shift work and vascular events: systematic review and meta-analysis". British Medical Journal (Clinical Research Edition) 26 (345): e4800. doi:10.1136/bmj.e4800. PMC 3406223. PMID 22835925.
- ↑ Krenz M, Korthuis RJ (January 2012). "Moderate ethanol ingestion and cardiovascular protection: from epidemiologic associations to cellular mechanisms". Journal of molecular and cellular cardiology 52 (1): 93–104. doi:10.1016/j.yjmcc.2011.10.011. PMC 3246046. PMID 22041278.
- ↑ U.S. Departments of Agriculture and Health and Human Services. "Dietary Guidelines 2015 - 2020". Retrieved 9 January 2016.
- ↑ Hooper, L; Martin, N; Abdelhamid, A; Davey Smith, G (10 June 2015). "Reduction in saturated fat intake for cardiovascular disease.". The Cochrane database of systematic reviews 6: CD011737. doi:10.1002/14651858.CD011737. PMID 26068959.
- 1 2 Chowdhury R, Warnakula S, Kunutsor S, Crowe F, Ward HA, Johnson L, Franco OH, Butterworth AS, Forouhi NG, Thompson SG, Khaw KT, Mozaffarian D, Danesh J, Di Angelantonio E (2014). "Association of dietary, circulating, and supplement fatty acids with coronary risk: a systematic review and meta-analysis". Ann. Intern. Med. 160 (6): 398–406. doi:10.7326/M13-1788. PMID 24723079.
- ↑ de Souza, RJ; Mente, A; Maroleanu, A; Cozma, AI; Ha, V; Kishibe, T; Uleryk, E; Budylowski, P; Schünemann, H; Beyene, J; Anand, SS (11 August 2015). "Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies.". BMJ (Clinical research ed.) 351: h3978. doi:10.1136/bmj.h3978. PMC 4532752. PMID 26268692.
- ↑ "Scientific Report of the 2015 Dietary Guidelines Advisory COmmittee" (PDF). health.gov. Feb 2015. p. 17.
- ↑ Buse JB, Ginsberg HN, Bakris GL, Clark NG, Costa F, Eckel R, Fonseca V, Gerstein HC, Grundy S, Nesto RW, Pignone MP, Plutzky J, Porte D, Redberg R, Stitzel KF, Stone NJ (January 2007). "Primary prevention of cardiovascular diseases in people with diabetes mellitus: a scientific statement from the American Heart Association and the American Diabetes Association". Circulation 115 (1): 114–26. doi:10.1161/CIRCULATIONAHA.106.179294. PMID 17192512.
- ↑ Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, Lang CC, Rumboldt Z, Onen CL, Lisheng L, Tanomsup S, Wangai P, Razak F, Sharma AM, Anand SS (2005). "Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control study". Lancet 366 (9497): 1640–9. doi:10.1016/S0140-6736(05)67663-5. PMID 16271645.
- 1 2 Chatzidimitriou D, Kirmizis D, Gavriilaki E, Chatzidimitriou M, Malisiovas N (Oct 2012). "Atherosclerosis and infection: is the jury still not in?". Future microbiology 7 (10): 1217–30. doi:10.2217/fmb.12.87. PMID 23030426.
- ↑ Charakida M, Tousoulis D (2013). "Infections and atheromatous plaque: current therapeutic implications.". Current pharmaceutical design 19 (9): 1638–50. doi:10.2174/138161213805219658. PMID 23016720.
- ↑ Sánchez-Manubens J, Bou R, Anton J (February 2014). "Diagnosis and classification of Kawasaki disease". Journal of Autoimmunity. 48-49: 113–7. doi:10.1016/j.jaut.2014.01.010. PMID 24485156.
- 1 2 3 Feero, W. Gregory; Guttmacher, Alan E.; O'Donnell, Christopher J.; Nabel, Elizabeth G. (Dec 2011). "Genomics of Cardiovascular Disease". New England Journal of Medicine 365 (22): 2098–2109. doi:10.1056/NEJMra1105239. PMID 22129254.
- ↑ Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB (1998). "Prediction of coronary heart disease using risk factor categories" (PDF). Circulation 97 (18): 1843–44. doi:10.1161/01.CIR.97.18.1837. PMID 9603539.
- ↑ Khader YS, Rice J, John L, Abueita O (2003). "Oral contraceptives use and the risk of myocardial infarction: a meta-analysis". Contraception 68 (1): 11–7. doi:10.1016/S0010-7824(03)00073-8. PMID 12878281.
- ↑ Culić V (April 2007). "Acute risk factors for myocardial infarction". International journal of cardiology 117 (2): 260–9. doi:10.1016/j.ijcard.2006.05.011. PMID 16860887.
- ↑ Shaw E, Tofler GH (July 2009). "Circadian rhythm and cardiovascular disease". Current atherosclerosis reports 11 (4): 289–95. doi:10.1007/s11883-009-0044-4. PMID 19500492.
- 1 2 Moe KT, Wong P (March 2010). "Current trends in diagnostic biomarkers of acute coronary syndrome" (PDF). Ann. Acad. Med. Singap. 39 (3): 210–5. PMID 20372757.
- 1 2 Tsujita K, Kaikita K, Soejima H, Sugiyama S, Ogawa H (April 2010). "[Acute coronary syndrome-initiating factors]". Nippon Rinsho (in Japanese) 68 (4): 607–14. PMID 20387549.
- 1 2 Dohi T, Daida H (April 2010). "[Change of concept and pathophysiology in acute coronary syndrome]". Nippon Rinsho (in Japanese) 68 (4): 592–6. PMID 20387546.
- ↑ Woollard KJ, Geissmann F (February 2010). "Monocytes in atherosclerosis: subsets and functions". Nature Reviews Cardiology 7 (2): 77–86. doi:10.1038/nrcardio.2009.228. PMC 2813241. PMID 20065951.
- ↑ Spaan J, Kolyva C, van den Wijngaard J, ter Wee R, van Horssen P, Piek J, Siebes M (September 2008). "Coronary structure and perfusion in health and disease". Philosophical Transactions of the Royal Society A 366 (1878): 3137–53. doi:10.1098/rsta.2008.0075. PMID 18559321.
- ↑ Laflamme, MA; Murry, CE (July 2005). "Regenerating the heart". Nature Biotechnology 23 (7): 845–56. doi:10.1038/nbt1117. PMID 16003373.
- ↑ Krijnen PA, Nijmeijer R, Meijer CJ, Visser CA, Hack CE, Niessen HW (2002). "Apoptosis in myocardial ischaemia and infarction". J Clin Pathol 55 (11): 801–11. doi:10.1136/jcp.55.11.801. PMC 1769793. PMID 12401816.
- 1 2 3 4 Wilson AM, Ryan MC, Boyle AJ (2006). "The novel role of C-reactive protein in cardiovascular disease: risk marker or pathogen". Int J Cardiol 106 (3): 291–7. doi:10.1016/j.ijcard.2005.01.068. PMID 16337036.
- ↑ Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO, Criqui M, Fadl YY, Fortmann SP, Hong Y, Myers GL, Rifai N, Smith SC, Taubert K, Tracy RP, Vinicor F (2003). "Markers of inflammation and cardiovascular disease: application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association" (PDF). Circulation 107 (3): 499–511. doi:10.1161/01.CIR.0000052939.59093.45. PMID 12551878.
- ↑ Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC (2004). "Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals". JAMA 291 (2): 210–5. doi:10.1001/jama.291.2.210. PMID 14722147.
- ↑ Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, Liu K, Shea S, Szklo M, Bluemke DA, O'Leary DH, Tracy R, Watson K, Wong ND, Kronmal RA (2008). "Coronary calcium as a predictor of coronary events in four racial or ethnic groups". N. Engl. J. Med. 358 (13): 1336–45. doi:10.1056/NEJMoa072100. PMID 18367736.
- ↑ Arad Y, Goodman KJ, Roth M, Newstein D, Guerci AD (2005). "Coronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study". J. Am. Coll. Cardiol. 46 (1): 158–65. doi:10.1016/j.jacc.2005.02.088. PMID 15992651.
- ↑ Clarke R, Halsey J, Bennett D, Lewington S (February 2011). "Homocysteine and vascular disease: review of published results of the homocysteine-lowering trials". J. Inherit. Metab. Dis. 34 (1): 83–91. doi:10.1007/s10545-010-9235-y. PMID 21069462.
- ↑ Lonn E (September 2007). "Homocysteine in the prevention of ischemic heart disease, stroke and venous thromboembolism: therapeutic target or just another distraction?". Current Opinion in Hematology 14 (5): 481–7. doi:10.1097/MOH.0b013e3282c48bd8. PMID 17934354.
- 1 2 Reznik AG (2010). "[Morphology of acute myocardial infarction at prenecrotic stage]". Kardiologiia (in Russian) 50 (1): 4–8. PMID 20144151.
- ↑ Alpert JS, Thygesen K, Antman E, Bassand JP (2000). "Myocardial infarction redefined—a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction". J Am Coll Cardiol 36 (3): 959–69. doi:10.1016/S0735-1097(00)00804-4. PMID 10987628.
- ↑ Anonymous (March 1979). "Nomenclature and criteria for diagnosis of ischemic heart disease. Report of the Joint International Society and Federation of Cardiology/World Health Organization task force on standardization of clinical nomenclature". Circulation 59 (3): 607–9. doi:10.1161/01.CIR.59.3.607. PMID 761341.
- ↑ Thygesen K, Alpert JS, White HD (October 2007). "Universal definition of myocardial infarction". Eur. Heart J. 28 (20): 2525–38. doi:10.1093/eurheartj/ehm355. PMID 17951287.
- ↑ Primary Care: Art and Science of Advanced Practice Nursing. F.A. Davis. 2015. p. 464. ISBN 9780803644946.
- 1 2 3 4 5 6 7 8 9 10 Amsterdam, E. A.; Wenger, N. K.; Brindis, R. G.; Casey, D. E.; Ganiats, T. G.; Holmes, D. R.; Jaffe, A. S.; Jneid, H.; Kelly, R. F.; Kontos, M. C.; Levine, G. N.; Liebson, P. R.; Mukherjee, D.; Peterson, E. D.; Sabatine, M. S.; Smalling, R. W.; Zieman, S. J. (23 September 2014). "2014 AHA/ACC Guideline for the Management of Patients With Non-ST-Elevation Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines". Circulation 130 (Online first): e344–e426. doi:10.1161/CIR.0000000000000134. PMID 25249585.
- ↑ Lansky, A. J.; Stone, G. W. (14 December 2010). "Periprocedural Myocardial Infarction: Prevalence, Prognosis, and Prevention". Circulation: Cardiovascular Interventions 3 (6): 602–610. doi:10.1161/CIRCINTERVENTIONS.110.959080.
- ↑ Lipinski, MJ; Escárcega, RO; D'Ascenzo, F; Magalhães, MA; Baker, NC; Torguson, R; Chen, F; Epstein, SE; Miró, O; Llorens, P; Giannitsis, E; Lotze, U; Lefebvre, S; Sebbane, M; Cristol, JP; Chenevier-Gobeaux, C; Meune, C; Eggers, KM; Charpentier, S; Twerenbold, R; Mueller, C; Biondi-Zoccai, G; Waksman, R (May 1, 2014). "A systematic review and collaborative meta-analysis to determine the incremental value of copeptin for rapid rule-out of acute myocardial infarction.". The American journal of cardiology 113 (9): 1581–91. doi:10.1016/j.amjcard.2014.01.436. PMID 24731654.
- ↑ Schinkel AF, Valkema R, Geleijnse ML, Sijbrands EJ, Poldermans D (May 2010). "Single-photon emission computed tomography for assessment of myocardial viability". Eurointervention 6 (Supplement G): G115–22. PMID 20542817.
- 1 2 3 4 5 6 National Institute for Health and Clinical Excellence. Clinical guideline cg94: Unstable angina and NSTEMI. London, 2010.
- 1 2 3 American Society of Nuclear Cardiology. "Five Things Physicians and Patients Should Question" (PDF). Choosing Wisely: an initiative of the ABIM Foundation (American Society of Nuclear Cardiology). Retrieved August 17, 2012., which cites
- Hendel RC, Berman DS, Di Carli MF, Heidenreich PA, Henkin RE, Pellikka PA, Pohost GM, Williams KA (2009). "ACCF/ASNC/ACR/AHA/ASE/SCCT/SCMR/SNM 2009 Appropriate Use Criteria for Cardiac Radionuclide Imaging". Journal of the American College of Cardiology 53 (23): 2201–2229. doi:10.1016/j.jacc.2009.02.013. PMID 19497454.
- Taylor AJ, Cerqueira M, Hodgson JM, Mark D, Min J, O'Gara P, Rubin GD, Kramer CM, Berman D, Brown A, Chaudhry FA, Cury RC, Desai MY, Einstein AJ, Gomes AS, Harrington R, Hoffmann U, Khare R, Lesser J, McGann C, Rosenberg A, Schwartz R, Shelton M, Smetana GW, Smith SC (2010). "ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 Appropriate Use Criteria for Cardiac Computed Tomography". Journal of the American College of Cardiology 56 (22): 1864–1894. doi:10.1016/j.jacc.2010.07.005. PMID 21087721.
- Anderson, J. L.; Adams, C. D.; Antman, E. M.; Bridges, C. R.; Califf, R. M.; Casey, D. E.; Chavey, W. E.; Fesmire, F. M.; Hochman, J. S.; Levin, T. N.; Lincoff, A. M.; Peterson, E. D.; Theroux, P.; Wenger, N. K.; Wright, R. S. (2007). "ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction): Developed in Collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons: Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine". Circulation 116 (7): 803–877. doi:10.1161/CIRCULATIONAHA.107.185752.
- ↑ Boie ET (2005). "Initial evaluation of chest pain". Emerg. Med. Clin. North Am. 23 (4): 937–57. doi:10.1016/j.emc.2005.07.007. PMID 16199332.
- 1 2 3 4 5 6 7 8 National Institute for Health and Clinical Excellence. Clinical guideline 181: Lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease. London, 2014.
- ↑ Stradling, C; Hamid, M; Taheri, S; Thomas, GN (2014). "A review of dietary influences on cardiovascular health: part 2: dietary patterns.". Cardiovascular & hematological disorders drug targets 14 (1): 50–63. doi:10.2174/1871529x14666140701095426. PMID 24993125.
- ↑ Fortmann, SP; Burda, BU; Senger, CA; Lin, JS; Whitlock, EP (17 December 2013). "Vitamin and mineral supplements in the primary prevention of cardiovascular disease and cancer: An updated systematic evidence review for the U.S. Preventive Services Task Force.". Annals of Internal Medicine 159 (12): 824–34. doi:10.7326/0003-4819-159-12-201312170-00729. PMID 24217421.
- ↑ Mozaffarian D, Micha R, Wallace S (2010). Katan, Martijn B, ed. "Effects on Coronary Heart Disease of Increasing Polyunsaturated Fat in Place of Saturated Fat: A Systematic Review and Meta-Analysis of Randomized Controlled Trials". PLoS Med. 7 (3): e1000252. doi:10.1371/journal.pmed.1000252. PMC 2843598. PMID 20351774.
- ↑ McPherson K, et al. (June 2010). "Prevention of cardiovascular disease – NICE public health guidance 25". London: National Institute for Health and Care Excellence.
- ↑ Antithrombotic Trialists' (ATT), Collaboration; Baigent, C; Blackwell, L; Collins, R; Emberson, J; Godwin, J; Peto, R; Buring, J; Hennekens, C; Kearney, P; Meade, T; Patrono, C; Roncaglioni, MC; Zanchetti, A (30 May 2009). "Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials.". Lancet 373 (9678): 1849–60. doi:10.1016/S0140-6736(09)60503-1. PMC 2715005. PMID 19482214.
- ↑ Sutcliffe, P; Connock, M; Gurung, T; Freeman, K; Johnson, S; Kandala, NB; Grove, A; Gurung, B; Morrow, S; Clarke, A (September 2013). "Aspirin for prophylactic use in the primary prevention of cardiovascular disease and cancer: a systematic review and overview of reviews.". Health technology assessment (Winchester, England) 17 (43): 1–253. doi:10.3310/hta17430. PMID 24074752.
- ↑ Matthys, F; De Backer, T; De Backer, G; Stichele, RV (March 2014). "Review of guidelines on primary prevention of cardiovascular disease with aspirin: how much evidence is needed to turn a tanker?". European journal of preventive cardiology 21 (3): 354–65. doi:10.1177/2047487312472077. PMID 23610452.
- ↑ Hodis, Howard (July 2014). "Hormone replacement therapy and the association with coronary heart disease and overall mortality: Clinical application of the timing hypothesis". The Journal of Steroid Biochemistry and Molecular Biology 142: 68–75. doi:10.1016/j.jsbmb.2013.06.011. PMID 23851166.
- ↑ Hodis, Howard; Mack, Wendy (July 2014). "Hormone replacement therapy and the association with coronary heart disease and overall mortality: Clinical application of the timing hypothesis". The Journal of Steroid Biochemistry and Molecular Biology 142: 68–75. doi:10.1016/j.jsbmb.2013.06.011. PMID 23851166. Retrieved 2015-03-25.
- ↑ Hodis, HN; Mack, WJ (2009). "Coronary heart disease and hormone replacement therapy after the menopause.". Climacteric : the journal of the International Menopause Society. 12 Suppl 1: 71–5. doi:10.1080/13697130903095178. PMID 19811246.
- ↑ Perez, MI; Musini, VM; Wright, JM (7 October 2009). "Effect of early treatment with anti-hypertensive drugs on short and long-term mortality in patients with an acute cardiovascular event.". The Cochrane database of systematic reviews (4): CD006743. doi:10.1002/14651858.CD006743.pub2. PMID 19821384.
- ↑ Gulli, American Academy of Orthopaedic Surgeons ; editors, Leaugeay Barnes, Joseph A. Ciotola, Benjamin (2010-03-23). Emergency care and transportation of the sick and injured. (10th ed.). Sudbury, Mass.: Jones and Bartlett. p. 575. ISBN 978-0-7637-7828-6.
- ↑ O'Connor RE, Brady W, Brooks SC, Diercks D, Egan J, Ghaemmaghami C, Menon V, O'Neil BJ, Travers AH, Yannopoulos D (November 2010). "Part 10: acute coronary syndromes: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care". Circulation 122 (18 Suppl 3): S787–817. doi:10.1161/CIRCULATIONAHA.110.971028. PMID 20956226.
- ↑ Wijesinghe M, Perrin K, Ranchord A, Simmonds M, Weatherall M, Beasley R (March 2009). "Routine use of oxygen in the treatment of myocardial infarction: systematic review". Heart 95 (3): 198–202. doi:10.1136/hrt.2008.148742. PMID 18708420.
- ↑ Cabello JB, Burls A, Emparanza JI, Bayliss S, Quinn T (2013). Cabello, Juan B, ed. "Oxygen therapy for acute myocardial infarction". Cochrane Database Syst Rev 8: CD007160. doi:10.1002/14651858.CD007160.pub3. PMID 23963794.
- ↑ Ahmad Y, Sen S, Shun-Shin MJ, Ouyang J, Finegold JA, Al-Lamee RK, Davies JE, Cole GD, Francis DP (June 2015). "Intra-aortic Balloon Pump Therapy for Acute Myocardial Infarction: A Meta-analysis". JAMA Internal Medicine 175 (6): 931–9. doi:10.1001/jamainternmed.2015.0569. PMID 25822657.
- 1 2 3 Bates ER, Menees DS (Oct 2012). "Acute ST-elevation myocardial infarction". Current Opinion in Critical Care. 5 18 (5): 417–23. doi:10.1097/MCC.0b013e328357f07b. PMID 22889871.
- 1 2 Bagai, A; Dangas, GD; Stone, GW; Granger, CB (6 June 2014). "Reperfusion strategies in acute coronary syndromes.". Circulation Research 114 (12): 1918–28. doi:10.1161/CIRCRESAHA.114.302744. PMID 24902975.
- 1 2 Wang, edited by Reza Ardehali, Marco Perez, Paul (2011). A practical approach to cardiovascular medicine. Chichester, West Sussex, UK: Wiley-Blackwell. p. 57. ISBN 9781444393873.
- ↑ Lassen JF, Bøtker HE, Terkelsen CJ (Jan 2013). "Timely and optimal treatment of patients with STEMI". Nature Reviews Cardiology. 1 10 (1): 41–8. doi:10.1038/nrcardio.2012.156. PMID 23165072.
- ↑ Neumar, RW; Shuster, M; Callaway, CW; Gent, LM; Atkins, DL; Bhanji, F; Brooks, SC; de Caen, AR; Donnino, MW; Ferrer, JM; Kleinman, ME; Kronick, SL; Lavonas, EJ; Link, MS; Mancini, ME; Morrison, LJ; O'Connor, RE; Samson, RA; Schexnayder, SM; Singletary, EM; Sinz, EH; Travers, AH; Wyckoff, MH; Hazinski, MF (3 November 2015). "Part 1: Executive Summary: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.". Circulation 132 (18 Suppl 2): S315–67. doi:10.1161/cir.0000000000000252. PMID 26472989.
- ↑ "Thrombolytics for Major Heart Attack (STEMI)". TheNNT.com. Retrieved 1 December 2015.
- ↑ "Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Fibrinolytic Therapy Trialists' (FTT) Collaborative Group.". Lancet 19 (343(8899)): 742. Mar 1994. doi:10.1016/s0140-6736(94)91161-4. PMID 7905143.
- 1 2 McCaul, M; Lourens, A; Kredo, T (Sep 10, 2014). "Pre-hospital versus in-hospital thrombolysis for ST-elevation myocardial infarction.". The Cochrane database of systematic reviews 9: CD010191. doi:10.1002/14651858.CD010191.pub2. PMID 25208209.
- ↑ Jindal, editor-in-chief SK (2011). Textbook of pulmonary and critical care medicine. New Delhi: Jaypee Brothers Medical Publishers. p. 1758. ISBN 9789350250730.
- ↑ Brilakis ES, Patel VG, Banerjee S (Jul 10, 2013). "Medical management after coronary stent implantation: a review". JAMA: the Journal of the American Medical Association 310 (2): 189–98. doi:10.1001/jama.2013.7086. PMID 23839753.
- ↑ "Beta Blockers for Acute Heart Attack (Myocardial Infarction)". TheNNT.com. Retrieved 11 December 2015.
- ↑ O'Gara, P. T.; Kushner, F. G.; Ascheim, D. D.; Casey, D. E.; Chung, M. K.; de Lemos, J. A.; Ettinger, S. M.; Fang, J. C.; Fesmire, F. M.; Franklin, B. A.; Granger, C. B.; Krumholz, H. M.; Linderbaum, J. A.; Morrow, D. A.; Newby, L. K.; Ornato, J. P.; Ou, N.; Radford, M. J.; Tamis-Holland, J. E.; Tommaso, C. L.; Tracy, C. M.; Woo, Y. J.; Zhao, D. X. (17 December 2012). "2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines". Circulation 127 (4): e362–e425. doi:10.1161/CIR.0b013e3182742cf6. PMID 23247304.
- 1 2 Andrade-Castellanos, CA; Colunga-Lozano, LE; Delgado-Figueroa, N; Magee, K (Jun 27, 2014). "Heparin versus placebo for non-ST elevation acute coronary syndromes.". The Cochrane database of systematic reviews 6: CD003462. doi:10.1002/14651858.CD003462.pub3. PMID 24972265.
- ↑ Hamm, CW; Bassand, JP; Agewall, S; Bax, J; Boersma, E; Bueno, H; Caso, P; Dudek, D; Gielen, S; Huber, K; Ohman, M; Petrie, MC; Sonntag, F; Uva, MS; Storey, RF; Wijns, W; Zahger, D; ESC Committee for Practice, Guidelines (December 2011). "ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC).". European Heart Journal 32 (23): 2999–3054. doi:10.1093/eurheartj/ehr236. PMID 21873419.
- ↑ Bellemain-Appaix, A.; Kerneis, M.; O'Connor, S. A.; Silvain, J.; Cucherat, M.; Beygui, F.; Barthelemy, O.; Collet, J.-P.; Jacq, L.; Bernasconi, F.; Montalescot, G. (24 October 2014). "Reappraisal of thienopyridine pretreatment in patients with non-ST elevation acute coronary syndrome: a systematic review and meta-analysis". BMJ 347 (aug06 2): g6269–g6269. doi:10.1136/bmj.g6269.
- 1 2 3 4 5 6 7 8 9 National Institute for Health and Clinical Excellence. Clinical guideline 172: Secondary prevention in primary and secondary care for patients following a myocardial infarction. London, 2013.
- ↑ Anderson, L; Taylor, RS (12 December 2014). "Cardiac rehabilitation for people with heart disease: an overview of Cochrane systematic reviews.". The Cochrane database of systematic reviews 12: CD011273. doi:10.1002/14651858.CD011273.pub2. PMID 25503364.
- ↑ Elmariah, Sammy; Mauri, Laura; Doros, Gheorghe; Galper, Benjamin Z; O'Neill, Kelly E; Steg, Philippe Gabriel; Kereiakes, Dean J; Yeh, Robert W (November 2014). "Extended duration dual antiplatelet therapy and mortality: a systematic review and meta-analysis". The Lancet 385: 792–798. doi:10.1016/S0140-6736(14)62052-3.
- ↑ Bangalore, S; Makani, H; Radford, M; Thakur, K; Toklu, B; Katz, SD; DiNicolantonio, JJ; Devereaux, PJ; Alexander, KP; Wetterslev, J; Messerli, FH (October 2014). "Clinical outcomes with β-blockers for myocardial infarction: a meta-analysis of randomized trials.". The American Journal of Medicine 127 (10): 939–53. doi:10.1016/j.amjmed.2014.05.032. PMID 24927909.
- ↑ McCord, J; Jneid, H; Hollander, JE; de Lemos, JA; Cercek, B; Hsue, P; Gibler, WB; Ohman, EM; Drew, B; Philippides, G; Newby, LK; American Heart Association Acute Cardiac Care Committee of the Council on Clinical, Cardiology (8 April 2008). "Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology.". Circulation 117 (14): 1897–907. doi:10.1161/CIRCULATIONAHA.107.188950. PMID 18347214.
- ↑ Taylor F, Huffman MD, Macedo AF, Moore TH, Burke M, Davey Smith G, Ward K, Ebrahim S (Jan 31, 2013). "Statins for the primary prevention of cardiovascular disease". The Cochrane database of systematic reviews 1: CD004816. doi:10.1002/14651858.CD004816.pub5. PMID 23440795.
- ↑ Ray KK, Cannon CP; Cannon (2005). "The potential relevance of the multiple lipid-independent (pleiotropic) effects of statins in the management of acute coronary syndromes". J. Am. Coll. Cardiol. 46 (8): 1425–33. doi:10.1016/j.jacc.2005.05.086. PMID 16226165.
- 1 2 López de Sá E, López-Sendón J, Anguera I, Bethencourt A, Bosch X; López-Sendón; Anguera; Bethencourt; Bosch; Proyecto de Estudio del Pronostico de la Angina (PEPA) Investigators (November 2002). "Prognostic value of clinical variables at presentation in patients with non-ST-segment elevation acute coronary syndromes: results of the Proyecto de Estudio del Pronóstico de la Angina (PEPA)". Medicine (Baltimore) 81 (6): 434–42. doi:10.1097/00005792-200211000-00004. PMID 12441900.
- ↑ Fox KA, Dabbous OH, Goldberg RJ, Pieper KS, Eagle KA, Van de Werf F, Avezum A, Goodman SG, Flather MD, Anderson FA, Granger CB; Dabbous; Goldberg; Pieper; Eagle; Van De Werf; Avezum; Goodman; Flather; Anderson Jr; Granger (November 2006). "Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE)". BMJ 333 (7578): 1091. doi:10.1136/bmj.38985.646481.55. PMC 1661748. PMID 17032691.
- ↑ Weir RA, McMurray JJ, Velazquez EJ; McMurray; Velazquez (2006). "Epidemiology of heart failure and left ventricular systolic dysfunction after acute myocardial infarction: prevalence, clinical characteristics, and prognostic importance". Am J Cardiol 97 (10A): 13F–25F. doi:10.1016/j.amjcard.2006.03.005. PMID 16698331.
- ↑ Bosch X, Théroux P; Théroux (2005). "Left ventricular ejection fraction to predict early mortality in patients with non-ST-segment elevation acute coronary syndromes". Am Heart J 150 (2): 215–20. doi:10.1016/j.ahj.2004.09.027. PMID 16086920.
- ↑ Becker RC, Gore JM, Lambrew C, Weaver WD, Rubison RM, French WJ, Tiefenbrunn AJ, Bowlby LJ, Rogers WJ; Gore; Lambrew; Weaver; Rubison; French; Tiefenbrunn; Bowlby; Rogers (1996). "A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction". J Am Coll Cardiol 27 (6): 1321–6. doi:10.1016/0735-1097(96)00008-3. PMID 8626938.
- ↑ Liew R, Sulfi S, Ranjadayalan K, Cooper J, Timmis AD; Sulfi; Ranjadayalan; Cooper; Timmis (2006). "Declining case fatality rates for acute myocardial infarction in South Asian and white patients in the past 15 years". Heart 92 (8): 1030–4. doi:10.1136/hrt.2005.078634. PMC 1861115. PMID 16387823.
- ↑ Antman EM, Cohen M, et. al. (2000). "The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making.". JAMA 284 (7): 835–42. doi:10.1001/jama.284.7.835. PMID 10938172.
- ↑ David A. Morrow, et. al. (2000). "TIMI Risk Score for ST-Elevation Myocardial Infarction: A Convenient, Bedside, Clinical Score for Risk Assessment at Presentation: An Intravenous nPA for Treatment of Infarcting Myocardium Early II Trial Substudy.". Circulation 102 (17): 2031–37. doi:10.1161/01.CIR.102.17.2031. PMID 11044416.
- 1 2 3 World Health Organization (2008). The Global Burden of Disease: 2004 Update. Geneva: World Health Organization. ISBN 92-4-156371-0.
- ↑ Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Soliman EZ, Sorlie PD, Sotoodehnia N, Turan TN, Virani SS, Wong ND, Woo D, Turner MB; Go; Lloyd-Jones; Benjamin; Berry; Borden; Bravata; Dai; Ford; Fox; Fullerton; Gillespie; Hailpern; Heit; Howard; Kissela; Kittner; Lackland; Lichtman; Lisabeth; Makuc; Marcus; Marelli; Matchar; Moy; Mozaffarian; Mussolino; Nichol; Paynter; Soliman (January 2012). "Executive summary: heart disease and stroke statistics—2012 update: a report from the American Heart Association". Circulation 125 (1): 188–97. doi:10.1161/CIR.0b013e3182456d46. PMID 22215894.
- ↑ Mozaffarian, D; Benjamin, EJ; Go, AS; Arnett, DK; Blaha, MJ; Cushman, M; de Ferranti, S; Després, JP; Fullerton, HJ; Howard, VJ; Huffman, MD; Judd, SE; Kissela, BM; Lackland, DT; Lichtman, JH; Lisabeth, LD; Liu, S; Mackey, RH; Matchar, DB; McGuire, DK; Mohler ER, 3rd; Moy, CS; Muntner, P; Mussolino, ME; Nasir, K; Neumar, RW; Nichol, G; Palaniappan, L; Pandey, DK; Reeves, MJ; Rodriguez, CJ; Sorlie, PD; Stein, J; Towfighi, A; Turan, TN; Virani, SS; Willey, JZ; Woo, D; Yeh, RW; Turner, MB; American Heart Association Statistics Committee and Stroke Statistics, Subcommittee (27 January 2015). "Heart disease and stroke statistics--2015 update: a report from the American Heart Association.". Circulation 131 (4): e29–322. doi:10.1161/cir.0000000000000152. PMID 25520374.
From 2001 to 2011, death rates attributable to CVD declined 30.8%.
- ↑ Gupta R, Joshi P, Mohan V, Reddy KS, Yusuf S; Joshi; Mohan; Reddy; Yusuf (January 2008). "Epidemiology and causation of coronary heart disease and stroke in India". Heart 94 (1): 16–26. doi:10.1136/hrt.2007.132951. PMID 18083949.
- ↑ Torio CM, Andrews RM. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011. HCUP Statistical Brief #160. Agency for Healthcare Research and Quality, Rockville, MD. August 2013.
- ↑ Workers' Compensation FAQ. Prairie View A&M University. Retrieved November 22, 2006.
- ↑ SIGNIFICANT DECISIONS Subject Index. Board of Industrial Insurance Appeals. Retrieved November 22, 2006.
- ↑ "Classification of Drivers' Licenses Regulations". Nova Scotia Registry of Regulations. May 24, 2000. Retrieved April 22, 2007.
External links
- Cardiac disorders – Open Directory Project
- American Heart Association's Heart Attack web site — Information and resources for preventing, recognizing and treating heart attack.
- TIMI Score for UA/NSTEMI and STEMI
- HEART Score for Major Cardiac Events
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||
|