Epidural administration
| Epidural administration | |
|---|---|
| Intervention | |
 A freshly inserted lumbar epidural catheter. The site has been prepared with tincture of iodine, and the dressing has not yet been applied. Depth markings may be seen along the shaft of the catheter. | |
| ICD-9-CM | 03.90 |
| MeSH | D000767 |
| OPS-301 code | 8-910 |
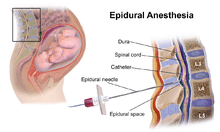
Epidural administration (from Ancient Greek ἐπί, "on, upon" + dura mater) is a medical route of administration in which a drug or contrast agent is injected into the epidural space of the spinal cord. Techniques such as epidural analgesia and epidural anaesthesia employ this route of administration. The epidural route is frequently employed by certain physicians and nurse anaesthetists to administer diagnostic (e.g. radiocontrast agents) and therapeutic (e.g., glucocorticoids) chemical substances, as well as certain analgesic and local anaesthetic agents. Epidural techniques frequently involve injection of drugs through a catheter placed into the epidural space. The injection can result in a loss of sensation—including the sensation of pain—by blocking the transmission of signals through nerve fibers in or near the spinal cord.
Difference from spinal anaesthesia
Spinal anaesthesia is a technique whereby a local anaesthetic drug is injected into the cerebrospinal fluid. This technique has some similarity to epidural anaesthesia, and lay people often confuse the two techniques. Important differences include:
- To achieve epidural analgesia or anaesthesia, a larger dose of drug is typically necessary than with spinal analgesia or anaesthesia.
- The onset of analgesia is slower with epidural analgesia or anaesthesia than with spinal analgesia or anaesthesia.
- An epidural injection may be performed anywhere along the vertebral column (cervical, thoracic, lumbar, or sacral), while spinal injections are typically performed below the second lumbar vertebral body to avoid piercing and consequently damaging the spinal cord.
- It is easier to achieve segmental analgesia or anaesthesia using the epidural route than using the spinal route.
- An indwelling catheter is more commonly placed in the setting of epidural analgesia or anaesthesia than with spinal analgesia or anaesthesia.
Indications
Injecting medication into the epidural space is primarily performed for analgesia. This may be performed using a number of different techniques and for a variety of reasons. Additionally, some of the side-effects of epidural analgesia may be beneficial in some circumstances (e.g., vasodilation may be beneficial if the subject has peripheral vascular disease). When a catheter is placed into the epidural space (see below) a continuous infusion can be maintained for several days, if needed. Epidural analgesia may be used:
- For analgesia alone, where surgery is not contemplated. An epidural injection or infusion for pain relief (e.g. in childbirth) is less likely to cause loss of muscle power, but has to be augmented to be sufficient for surgery.
- As an adjunct to general anaesthesia. The anaesthetist may use epidural analgesia in addition to general anaesthesia. This may reduce the patient's requirement for opioid analgesics. This is suitable for a wide variety of surgery, for example gynaecological surgery (e.g. hysterectomy), orthopaedic surgery (e.g. hip replacement), general surgery (e.g. laparotomy) and vascular surgery (e.g. open aortic aneurysm repair).
- As a sole technique for surgical anaesthesia. Some operations, most frequently Caesarean section, may be performed using an epidural anaesthetic as the sole technique. This can allow the patient to remain awake during the operation. The dose required for anaesthesia is much higher than that required for analgesia.
- For post-operative analgesia, after an operation where the epidural technique is employed as the sole anaesthetic, or in conjunction with general anaesthesia. Analgesics are administered into the epidural space typically for a few days after surgery, provided a catheter has been inserted. Through the use of a patient-controlled epidural analgesia (PCEA) infusion pump, a person can supplement an epidural infusion with occasional doses of pain medication through an epidural catheter.
- For the treatment of back pain. Injection of analgesics and steroids into the epidural space may improve some forms of back pain. See below.
- For the treatment of chronic pain or palliation of symptoms in terminal care, usually in the short- or medium-term.
The epidural space is more difficult and risky to access as one ascends the spine (because the spinal cord gains more nerves as it ascends and fills the epidural space leaving less room for error), so epidural techniques are most suitable for analgesia anywhere in the lower body and as high as the chest. They are (usually) much less suitable for analgesia for the neck, or arms and are not possible for the head (since sensory innervation for the head arises directly from the brain via cranial nerves rather than from the spinal cord via the epidural space.)
Anatomy
The epidural space is the space inside the bony spinal canal but just outside the dura mater ("dura"). In contact with the inner surface of the dura is another membrane called the arachnoid mater ("arachnoid"). The cerebrospinal fluid that surrounds the spinal cord is contained by the arachnoid mater. In adults, the spinal cord terminates around the level of the disc between L1 and L2 (in neonates it extends to L3 but can reach as low as L4), below which lies a bundle of nerves known as the cauda equina ("horse's tail"). Hence, lumbar epidural injections carry a low risk of injuring the spinal cord.
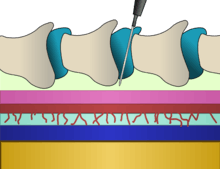
Insertion of an epidural needle involves threading a needle between the bones, through the ligaments and into the epidural potential space taking great care to avoid puncturing the layer immediately below containing CSF under pressure.
Technique
Procedures involving injection of any substance into the epidural space require the operator to be technically proficient in order to avoid complications.
The subject may be in the seated, lateral or prone positions.[1] The level of the spine at which the catheter is best placed depends mainly on the site and type of an intended operation or the anatomical origin of pain. The iliac crest is a commonly used anatomical landmark for lumbar epidural injections, as this level roughly corresponds with the fourth lumbar vertebra, which is usually well below the termination of the spinal cord. The Tuohy needle is usually inserted in the midline, between the spinous processes. When using a paramedian approach, the tip of the needle passes along a shelf of vertebral bone called the lamina until just before reaching the ligamentum flavum and the epidural space.
Along with a sudden loss of resistance to pressure on the plunger of the syringe, a slight clicking sensation may be felt by the operator as the tip of the needle breaches the ligamentum flavum and enters the epidural space. Practitioners commonly use air or saline for identifying the epidural space. However, evidence is accumulating that saline is preferable to air, as it is associated with a better quality of analgesia and lower incidence of post-dural-puncture headache.[2][3] In addition to the loss of resistance technique, realtime observation of the advancing needle is becoming more common. This may be done using a portable ultrasound scanner, or with fluoroscopy (moving X-ray pictures).[4]
After placement of the tip of the needle into the epidural space, a catheter is often threaded through the needle. The needle is then withdrawn over the catheter. Generally the catheter is inserted 4–6 cm into the epidural space.[5] The catheter is typically secured to the skin with adhesive tape or dressings to prevent it becoming dislodged.
The catheter is a fine plastic tube, through which anaesthetics may be injected into the epidural space. Many epidural catheters have a blind end but have three or more orifices along the shaft near the distal tip (far end) of the catheter. This not only disperses the injected agents more widely around the catheter, but also reduces the incidence of catheter blockage.
Choice of agents A person receiving an epidural for pain relief may receive local anaesthetic, an opioid, or both. Common local anaesthetics include lidocaine, mepivacaine, bupivacaine, ropivacaine, and chloroprocaine. Common opioids include hydromorphone, morphine, fentanyl, sufentanil, and pethidine (known as meperidine in the United States). These are injected in relatively small doses, compared to when they are injected intravenously. Other agents such as clonidine or ketamine are also sometimes used.

Bolus or infusion?
For a short procedure, the anaesthetist may introduce a single dose of medication (the "bolus" technique). This will eventually dissipate. Thereafter, the anaesthetist may repeat the bolus provided the catheter remains undisturbed. For a prolonged effect, a continuous infusion of drugs may be employed. There is some evidence that an automated intermittent bolus technique provides better analgesia than a continuous infusion technique, though the total doses are identical.[6][7][8]
Level and intensity of block Typically, the effects of the epidural block are noted below a specific level on the body. This level may be determined by the anaesthetist. A high insertion level may result in sparing of nerve function in the lower spinal nerves. For example, a thoracic epidural may be performed for upper abdominal surgery, but may not have any effect on the perineum (area around the genitals) or pelvic organs.[9] Nonetheless, giving very large volumes into the epidural space may spread the block both higher and lower.
The intensity of the block is determined by the concentration of local anaesthetic solution used. For example, 0.1% bupivacaine may provide adequate analgesia for a woman in labour, but would likely be insufficient for surgical anaesthesia. Conversely, 0.5% bupivacaine would provide a more intense block, likely sufficient for surgery.
Removing the catheter
The catheter is usually removed when the subject is able to take oral pain medications. Catheters can safely remain in place for several days with little risk of bacterial infection,[10][11][12] particularly if the skin is prepared with a chlorhexidine solution.[13] Subcutaneously tunneled epidural catheters may be left in place for longer periods, with a low risk of infection or other complications.[14][15][16]
Special situations
Epidural analgesia during childbirth
Epidural analgesia provides rapid pain relief in most cases. It is more effective than nitrous oxide, opioids, TENS, and other common modalities of analgesia in childbirth.[17] Epidurals during childbirth are the most commonly used anesthesia in this situation. The medication levels are very low to decrease the side effects to both mother and baby. When in labor the mother does not usually feel pain after an epidural but they do still feel the pressure. Women are able to bear down and push with contractions.[18] Epidural clonidine has been extensively studied for management of analgesia during labour.[19] Epidural analgesia is a relatively safe method of relieving pain in labour. In a 2011 Cochrane review which included 38 randomized controlled studies involving 9658 women, wherein all but five studies compared epidural analgesia with opiates, epidural analgesia in childbirth was associated with the following advantages and disadvantages:[20]
| Advantages | Disadvantages |
|---|---|
|
|
However, the review found no difference in overall Caesarean delivery rates, nor were there effects on the baby soon after birth. Also, the occurrence of long-term backache was no different whether an epidural was or was not used.[20]
Though complications are rare, some women and their babies will experience them. Some side effects for the mother include headaches, dizziness, difficulty breathing and seizures. The child may experience slowed heartbeat, temperature regulation issues and there could be high levels of drugs in the babies system from the epidural.[22]
Differing outcomes in frequency of Cesarean section may be explained by differing institutions or their practitioners: epidural anaesthesia and analgesia administered at top-rated institutions does not generally result in a clinically significant increase in caesarean rates, whereas the risk of caesarean delivery at poorly ranked facilities seems to increase with the use of epidural.[23]
Regarding early or late administration of epidural analgesia, there is no overall difference in outcomes for first-time moms in labour.[24] Specifically, the rate of caesarean section, instrumental birth, or duration of labour is equal, as well as baby Apgar scores and cord pH.[24]
Epidurals (other than low-dose ambulatory epidurals[25]) preclude maternal movement, but "walking, movement, and changing positions during labor help labor progress, enhance comfort, and decrease the risk of complications."[26]
One study concluded that women whose epidural infusions contained fentanyl were less likely to fully breastfeed their infant in the few days after birth and more likely to stop breastfeeding in the first 24 weeks.[27] However, this study has been criticised for several reasons, one of which is that the original patient records were not examined in this study, and so many of the epidural infusions were assumed to contain fentanyl when almost certainly they would not have.[28] In addition, all those who had received epidural infusions in this study had also received systemic pethidine, which would be much more likely to be the cause of any effect on breastfeeding due to the higher amounts of medication used via that route. If this were the case, then early epidural analgesia which avoided the need for pethidine would be expected to improve breastfeeding outcomes rather than worsen them. Traditional epidural for labour relieves pain reliably only during first stage of labour (uterine contractions till cervix is fully open). It does not relieve pain as reliably during the second stage of labour( passage of the fetus through the vagina).
Epidural analgesia after surgery
Epidural analgesia has been demonstrated to have several benefits after surgery, including:
- Effective analgesia without the need for systemic opioids.[29]
- The incidence of postoperative respiratory problems and chest infections is reduced.[30]
- The incidence of postoperative myocardial infarction ("heart attack") is reduced.[31][32]
- The stress response to surgery is reduced.[31][33]
- Motility of the intestines is improved by blockade of the sympathetic nervous system.[31][34]
- Use of epidural analgesia during surgery reduces blood transfusion requirements.[31]
Despite these benefits, no survival benefit has been proven for high-risk individuals.[35]
Caudal epidural analgesia
The caudal approach to the epidural space involves the use of a Tuohy needle, an intravenous catheter, or a hypodermic needle to puncture the sacrococcygeal membrane. Injecting local anaesthetic at this level can result in analgesia and/or anaesthesia of the perineum and groin areas. The caudal epidural technique is often used in infants and children undergoing surgery involving the groin, pelvis or lower extremities. In this population, caudal epidural analgesia is usually combined with general anaesthesia since most children do not tolerate surgery when regional anaesthesia is employed as the sole modality.
Combined spinal-epidural techniques
For some procedures, the anaesthetist may choose to combine the rapid onset and reliable, dense block of a spinal anaesthetic with the post-operative analgesic effects of an epidural. This is called combined spinal and epidural anaesthesia (CSE). The practitioner may insert the spinal anaesthetic at one level, and the epidural at an adjacent level. Alternatively, after locating the epidural space with the Tuohy needle, a spinal needle may be inserted through the Tuohy needle into the subarachnoid space. The spinal dose is then given, the spinal needle withdrawn, and the epidural catheter inserted as normal. This method, known as the "needle-through-needle" technique, may be associated with a slightly higher risk of placing the catheter into the subarachnoid space.
Epidural steroid injection
Epidural steroid injection may be used to treat radiculopathy, radicular pain and inflammation caused by such conditions as spinal disc herniation, degenerative disc disease, and spinal stenosis. Steroids may be injected at the cervical, thoracic, lumbar, or caudal/sacral levels, depending on the specific area where the pathology (disease, condition, or injury) is located.
Side effects
In addition to blocking the nerves which carry pain, local anaesthetic drugs in the epidural space will block other types of nerves as well, in a dose-dependent manner. Depending on the drug and dose used, the effects may last only a few minutes or up to several hours. Epidural analgesia typically involves using the opiates fentanyl or sufentanil, with bupivacaine or one of its congeners. Fentanyl is a powerful opioid with a potency 80 times that of morphine and side effects common to the opiate class. Sufentanil is another opiate, 5 to 10 times more potent than Fentanyl. Bupivacaine is markedly toxic if inadvertently given intravenously, causing excitation, nervousness, tingling around the mouth, tinnitus, tremor, dizziness, blurred vision, or seizures, followed by depression: drowsiness, loss of consciousness, respiratory depression and apnea. Bupivacaine has caused several deaths by cardiac arrest when epidural anaesthetic has been accidentally inserted into a vein instead of the epidural space.
Sensory nerve fibers are more sensitive to the effects of the local anaesthetics than motor nerve fibers. This means that an epidural can provide analgesia while affecting muscle strength to a lesser extent. For example, a labouring woman may have a continuous epidural during labour that provides good analgesia without impairing her ability to move. If she requires a Caesarean section, she may be given a larger dose of epidural local anaesthetic.
The larger the dose used, the more likely it is that side effects will be evident. For example, very large doses of epidural anaesthetic can cause paralysis of the intercostal muscles and thoracic diaphragm (which are responsible for breathing), and loss of sympathetic nerve input to the heart, which may cause a significant decrease in heart rate and blood pressure. This may require emergency intervention, which may include support of the airway and the cardiovascular system.
The sensation of needing to urinate is often significantly diminished or even abolished after administration of epidural local anaesthetics and/or opioids. Because of this, a urinary catheter is often placed for the duration of the epidural infusion. People with continuous epidural infusions of local anaesthetic solutions typically ambulate only with assistance, if at all, in order to reduce the likelihood of injury due to a fall.
Large doses of epidurally administered opioids may cause troublesome itching, and respiratory depression.[36][37][38][39]
Complications
These include:
- failure to achieve analgesia or anaesthesia occurs in about 5% of cases, while another 15% experience only partial analgesia or anaesthesia. If analgesia is inadequate, another epidural may be attempted.
- The following factors are associated with failure to achieve epidural analgesia/anaesthesia:[40]
- Obesity
- Multiparity
- History of a previous failure of epidural anaesthesia
- History of regular opiate use
- Cervical dilation of more than 7 cm at insertion
- The use of air to find the epidural space while inserting the epidural instead of alternatives such as saline or lidocaine
- The following factors are associated with failure to achieve epidural analgesia/anaesthesia:[40]
- Accidental dural puncture with headache (common, about 1 in 100 insertions[41][42][43]). The epidural space in the adult lumbar spine is only 3-5mm deep, which means it is comparatively easy to cross it and accidentally puncture the dura (and arachnoid) with the needle. This may cause cerebrospinal fluid (CSF) to leak out into the epidural space, which may in turn cause a post dural puncture headache (PDPH). This can be severe and last several days, and in some rare cases weeks or months. It is caused by a reduction in CSF pressure and is characterised by postural exacerbation when the subject raises his/her head above the lying position. If severe it may be successfully treated with an epidural blood patch (a small amount of the subject's own blood given into the epidural space via another epidural needle which clots and seals the leak). Most cases resolve spontaneously with time. A change in headache pattern (e.g., headache worse when the subject lies down) should alert the physician to the possibility of development of rare but dangerous complications, such as subdural hematoma or cerebral venous thrombosis.[44]
- Delayed onset of breastfeeding and shorter duration of breastfeeding: In a study looking at breastfeeding 2 days after epidural anaesthesia, epidural analgesia in combination with oxytocin infusion caused women to have significantly lower oxytocin and prolactin levels in response to the baby breastfeeding on day 2 postpartum, which means less milk is produced. In many women undergoing epidural analgesia during labour oxytocin is used to augment uterine contractions.[45]
- Bloody tap (occurs in about 1 in 30–50).[46] It is easy to injure an epidural vein with the needle. In people who have normal blood clotting, it is extremely rare (estimated less than 0.07%) for permanent neurological problems to develop.[47] However, people who have a coagulopathy may be at risk of epidural hematoma.
- Catheter misplaced into a vein (uncommon, less than 1 in 300). Occasionally the catheter may be misplaced into an epidural vein, which results in all the anaesthetic being injected intravenously, where it can cause seizures or cardiac arrest[48][49] in large doses (about 1 in 10,000 insertions[43]). This also results in block failure.
- High block, as described above (uncommon, less than 1 in 500).
- Catheter misplaced into the subarachnoid space (rare, less than 1 in 1000). If the catheter is accidentally misplaced into the subarachnoid space (e.g. after an unrecognised accidental dural puncture), normally cerebrospinal fluid can be freely aspirated from the catheter (which would usually prompt the anaesthetist to withdraw the catheter and resite it elsewhere). If, however, this is not recognised, large doses of anaesthetic may be delivered directly into the cerebrospinal fluid. This may result in a high block, or, more rarely, a total spinal, where anaesthetic is delivered directly to the brainstem, causing unconsciousness and sometimes seizures.
- Neurological injury lasting less than 1 year (rare, about 1 in 6,700).[50]
- Epidural abscess formation (very rare, about 1 in 145,000).[50] Infection risk increases with the duration catheters are left in place, although infection was still uncommon after an average of 3 to 5 days' duration.[51]
- Epidural haematoma formation (very rare, about 1 in 168,000).[50]
- Neurological injury lasting longer than 1 year (extremely rare, about 1 in 240,000).[50]
- Paraplegia (1 in 250,000).[52]
- Arachnoiditis (extremely rare, fewer than 1000 cases in the past 50 years)[53]
- Death (extremely rare, less than 1 in 100,000).[52]
The figures above relate to epidural anaesthesia and analgesia in healthy individuals.
Evidence to support the assertion that epidural analgesia increases the risk of anastomotic breakdown following bowel surgery is lacking.[34][54]
Controversial claims:
- "epidural anaesthesia and analgesia significantly slows the second stage of labour". The following are a few plausible hypotheses for this phenomenon:
- The release of oxytocin, which stimulates the uterine contractions that are needed to move the child out through the vagina, may be decreased with epidural anaesthesia or analgesia due to factors involving the reduction of stress, such as:
- Epidural analgesia may reduce the endocrine stress response to pain[55]
- Diminished release of epinephrine from the adrenal medulla slows the release of oxytocin[56]
- Diminished blood pressure, accommodated by both decreased stress and less adrenal release, may decrease the release of oxytocin as a natural mechanism to avoid hypotension.[57] It may also affect the heart-rate of the fetus.[58]
- Epidural analgesia may reduce the endocrine stress response to pain[55]
- The release of oxytocin, which stimulates the uterine contractions that are needed to move the child out through the vagina, may be decreased with epidural anaesthesia or analgesia due to factors involving the reduction of stress, such as:
- Still plausible (though less studied without a documented reproduction in a laboratory setting) are the effects of the reclined position of the woman on the fetus, both immediately prior to and during delivery.
- These hypotheses generally posit an interaction with the force of gravity on fetal position and movement, as demonstrated by the following examples:
- Transverse or posterior fetal positioning may become more likely as a result of the shift in orientation to gravitational force.
- Diminished gravitational assistance is present in building pressure for commencing delivery and for progressing the fetus along the vagina.
- It is important to note that the orientation of the fetus can be established by ultrasonic stenography prior to, during, and after the administration of an epidural block. This would seem a fine experiment for testing the first hypothesis. It should also be noted that the majority of fetal movement through the vagina is accomplished by cervical contractions, and so the role of gravity and its force relative to the position of the woman in labour (on delivery, not development) is difficult to establish.
- These hypotheses generally posit an interaction with the force of gravity on fetal position and movement, as demonstrated by the following examples:
- There has been a good deal of concern, based on older observational studies, that women who have epidural analgesia during labour are more likely to require a cesarean delivery.[59] However, the preponderance of evidence now supports the conclusion that the use of epidural analgesia during labour does not have a significant effect on rates of cesarean delivery. A Cochrane review of twenty trials involving a total of 6534 women estimated that women undergoing labour using epidural analgesia were only slightly more likely (1.07 times as likely) to undergo cesarean delivery than those in whom epidural analgesia was not used.
Epidural analgesia does increase the duration of the second stage of labour by 15 to 30 minutes and may increase the rate of instrument-assisted vaginal deliveries as well as that of oxytocin administration.[60][61] Some people have also been concerned about whether the use of epidural analgesia in early labour increases the risk of cesarean delivery. Three randomized, controlled trials showed that early initiation of epidural analgesia (cervical dilatation, <4 cm) does not increase the rate of cesarean delivery among women with spontaneous or induced labour, as compared with early initiation of analgesia with parenteral opioids.[62][63][64]
History

In 1885, American neurologist James Leonard Corning (1855–1923), of Acorn Hall in Morristown, NJ, was the first to perform neuraxial blockade, when he injected 111 mg of cocaine into the epidural space of a healthy male volunteer[65] (although at the time he believed he was injecting it into the subarachnoid space).[66]
In 1921, Spanish military surgeon Fidel Pagés (1886–1923) developed the technique of "single-shot" lumbar epidural anaesthesia,[67] which was later popularized by Italian surgeon Achille Mario Dogliotti (1897–1966).[68]
In 1941, Robert Andrew Hingson (1913–1996) and Waldo B. Edwards developed the technique of continuous caudal anaesthesia using an indwelling needle.[69] The first use of continuous caudal anaesthesia in a labouring woman was in 1942.[70]
In 1947, Manuel Martínez Curbelo (1906–1962) was the first to describe placement of a lumbar epidural catheter.[71]
References
- ↑ "Epidural Steroid Injections". Pain Management Specialists.
- ↑ Norman D (2003). "Epidural analgesia using loss of resistance with air versus saline: does it make a difference? Should we reevaluate our practice?". AANA J 71 (6): 449–53. PMID 15098532.
- ↑ Beilin Y, Arnold I, Telfeyan C, Bernstein HH, Hossain S (2000). "Quality of analgesia when air versus saline is used for identification of the epidural space in the parturient". Reg Anesth Pain Med 25 (6): 596–9. doi:10.1053/rapm.2000.9535. PMID 11097666.
- ↑ Rapp HJ, Folger A, Grau T (2005). "Ultrasound-guided epidural catheter insertion in children". Anesth Analg 101 (2): 333–9, table of contents. doi:10.1213/01.ANE.0000156579.11254.D1. PMID 16037140.
- ↑ Beilin Y, Bernstein HH, Zucker-Pinchoff B (1995). "The optimal distance that a multiorifice epidural catheter should be threaded into the epidural space". Anesth Analg 81 (2): 301–4. doi:10.1097/00000539-199508000-00016. PMID 7618719.
- ↑ Lim Y, Sia AT, Ocampo C (2005). "Automated regular boluses for epidural analgesia: a comparison with continuous infusion". Int J Obstet Anesth 14 (4): 305–9. doi:10.1016/j.ijoa.2005.05.004. PMID 16154735.
- ↑ Wong CA, Ratliff JT, Sullivan JT, Scavone BM, Toledo P, McCarthy RJ (2006). "A randomized comparison of programmed intermittent epidural bolus with continuous epidural infusion for labor analgesia". Anesth Analg 102 (3): 904–9. doi:10.1213/01.ane.0000197778.57615.1a. PMID 16492849.
- ↑ Sia AT, Lim Y, Ocampo C (2007). "A comparison of a basal infusion with automated mandatory boluses in parturient-controlled epidural analgesia during labor". Anesth Analg 104 (3): 673–8. doi:10.1213/01.ane.0000253236.89376.60. PMID 17312228.
- ↑ Basse L, Werner M, Kehlet H (2000). "Is urinary drainage necessary during continuous epidural analgesia after colonic resection?". Reg Anesth Pain Med 25 (5): 498–501. doi:10.1053/rapm.2000.9537. PMID 11009235.
- ↑ Kost-Byerly S, Tobin JR, Greenberg RS, Billett C, Zahurak M, Yaster M (1998). "Bacterial colonization and infection rate of continuous epidural catheters in children". Anesth Analg 86 (4): 712–6. doi:10.1097/00000539-199804000-00007. PMID 9539589.
- ↑ Kostopanagiotou G, Kyroudi S, Panidis D, Relia P, Danalatos A, Smyrniotis V, Pourgiezi T, Kouskouni E, Voros D (2002). "Epidural catheter colonization is not associated with infection". Surgical Infections 3 (4): 359–65. doi:10.1089/109629602762539571. PMID 12697082.
- ↑ Yuan HB, Zuo Z, Yu KW, Lin WM, Lee HC, Chan KH (2008). "Bacterial colonization of epidural catheters used for short-term postoperative analgesia: microbiological examination and risk factor analysis". Anesthesiology 108 (1): 130–7. doi:10.1097/01.anes.0000296066.79547.f3. PMID 18156891.
- ↑ Kinirons B, Mimoz O, Lafendi L, Naas T, Meunier J, Nordmann P (2001). "Chlorhexidine versus povidone iodine in preventing colonization of continuous epidural catheters in children: a randomized, controlled trial". Anesthesiology 94 (2): 239–44. doi:10.1097/00000542-200102000-00012. PMID 11176087.
- ↑ Aram L, Krane EJ, Kozloski LJ, Yaster M (2001). "Tunneled epidural catheters for prolonged analgesia in pediatric patients". Anesth Analg 92 (6): 1432–8. doi:10.1097/00000539-200106000-00016. PMID 11375820.
- ↑ Bubeck J, Boos K, Krause H, Thies KC (2004). "Subcutaneous tunneling of caudal catheters reduces the rate of bacterial colonization to that of lumbar epidural catheters". Anesth Analg 99 (3): 689–93, table of contents. doi:10.1213/01.ANE.0000130023.48259.FB. PMID 15333395.
- ↑ Nitescu P, Sjöberg M, Appelgren L, Curelaru I (1995). "Complications of intrathecal opioids and bupivacaine in the treatment of "refractory" cancer pain". Clin J Pain 11 (1): 45–62. doi:10.1097/00002508-199503000-00006. PMID 7540439.
- ↑ Howell CJ (1999). "Epidural versus non-epidural analgesia for pain relief in labour". The Cochrane Library (2): CD000331. doi:10.1002/14651858.CD000331. PMID 10796196. Also summarized at Bandolier
- ↑ Buckley, Sarah. "Epidurals: risks and concerns for mother and baby". Mothering No.133. Retrieved 18 April 2014.
- ↑ Patel SS, Dunn CJ, Bryson HM (1996). "Epidural clonidine: a review of its pharmacology and efficacy in the management of pain during labour and postoperative and intractable pain". CNS Drugs 6 (6): 474–497. doi:10.2165/00023210-199606060-00007.
- 1 2 Anim-Somuah M, Smyth RM, Jones L (2011). Anim-Somuah, Millicent, ed. "Epidural versus non-epidural or no analgesia in labour". The Cochrane Library (12): CD000331. doi:10.1002/14651858.CD000331.pub3. PMID 22161362.
- ↑ Salem IC, Fukushima FB, Nakamura G, Ferrari F, Navarro LC, Castiglia YM, Ganem EM (2007). "Side effects of subarachnoid and epidural sufentanil associated with a local anesthetic in patients undergoing labor analgesia". Revista brasileira de anestesiologia 57 (2): 125–135. PMID 19466346.
- ↑ "Anesthesia". Harvard University Press. Retrieved 18 April 2014.
- ↑ Thorp JA, Breedlove G (1996). "Epidural analgesia in labor: an evaluation of risks and benefits". Birth 23 (2): 63–83. doi:10.1111/j.1523-536X.1996.tb00833.x. PMID 8826170.
- 1 2 Sng BL, Leong WL, Zeng Y, Siddiqui FJ, Assam PN, Lim Y, Chan ES, Sia AT (Oct 9, 2014). "Early versus late initiation of epidural analgesia for labour.". The Cochrane database of systematic reviews 10: CD007238. doi:10.1002/14651858.CD007238.pub2. PMID 25300169.
- ↑ Dr Hayley Willacy; Dr Colin Tidy (2014-06-16). "Pain relief in labour". Patient.info. EMIS. Retrieved 2014-09-02.
- ↑ Lothian JA (2009). "Safe, healthy birth: what every pregnant woman needs to know". J Perinat Educ 18 (3): 48–54. doi:10.1624/105812409X461225. PMC 2730905. PMID 19750214.
- ↑ Torvaldsen S, Roberts CL, Simpson JM, Thompson JF, Ellwood DA (2006). "Intrapartum epidural analgesia and breastfeeding: a prospective cohort study". Int Breastfeed J 1 (1): 24. doi:10.1186/1746-4358-1-24. PMC 1702531. PMID 17134489.
- ↑ Camann W (2007). "Labor analgesia and breast feeding: avoid parenteral narcotics and provide lactation support". Int J Obstet Anesth 16 (3): 199–201. doi:10.1016/j.ijoa.2007.03.008. PMID 17521903.
- ↑ Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA, Wu CL (2003). "Efficacy of postoperative epidural analgesia: a meta-analysis". JAMA 290 (18): 2455–63. doi:10.1001/jama.290.18.2455. PMID 14612482.
- ↑ Ballantyne JC, Carr DB, deFerranti S, Suarez T, Lau J, Chalmers TC, Angelillo IF, Mosteller F (1998). "The comparative effects of postoperative analgesic therapies on pulmonary outcome: cumulative meta-analyses of randomized, controlled trials". Anesth Analg 86 (3): 598–612. doi:10.1097/00000539-199803000-00032. PMID 9495424.
- 1 2 3 4 Wilson IH, Allman KG (2006). Oxford handbook of anaesthesia. Oxford: Oxford University Press. p. 1038. ISBN 0-19-856609-3.
- ↑ Beattie WS, Badner NH, Choi P (2001). "Epidural analgesia reduces postoperative myocardial infarction: a meta-analysis". Anesth Analg 93 (4): 853–8. doi:10.1097/00000539-200110000-00010. PMID 11574345.
- ↑ Yokoyama M, Itano Y, Katayama H, Morimatsu H, Takeda Y, Takahashi T, Nagano O, Morita K (2005). "The effects of continuous epidural anesthesia and analgesia on stress response and immune function in patients undergoing radical esophagectomy". Anesth Analg 101 (5): 1521–7. doi:10.1213/01.ANE.0000184287.15086.1E. PMID 16244024.
- 1 2 Gendall KA, Kennedy RR, Watson AJ, Frizelle FA (2007). "The effect of epidural analgesia on postoperative outcome after colorectal surgery". Colorectal Dis 9 (7): 584–98; discussion 598–600. doi:10.1111/j.1463-1318.2007.1274.x. PMID 17506795.
- ↑ Rigg JR, Jamrozik K, Myles PS, Silbert BS, Peyton PJ, Parsons RW, Collins KS (2002). "Epidural anaesthesia and analgesia and outcome of major surgery: a randomised trial". Lancet 359 (9314): 1276–82. doi:10.1016/S0140-6736(02)08266-1. PMID 11965272.
- ↑ Krane EJ, Tyler DC, Jacobson LE (1989). "The dose response of caudal morphine in children". Anesthesiology 71 (1): 48–52. doi:10.1097/00000542-198907000-00009. PMID 2751139.
- ↑ Jacobson L, Chabal C, Brody MC (1988). "A dose-response study of intrathecal morphine: efficacy, duration, optimal dose, and side effects". Anesth Analg 67 (11): 1082–8. doi:10.1213/00000539-198867110-00011. PMID 3189898.
- ↑ Wüst HJ, Bromage PR (1987). "Delayed respiratory arrest after epidural hydromorphone". Anaesthesia 42 (4): 404–6. doi:10.1111/j.1365-2044.1987.tb03982.x. PMID 2438964.
- ↑ Haberkern CM, Lynn AM, Geiduschek JM, Nespeca MK, Jacobson LE, Bratton SL, Pomietto M (1996). "Epidural and intravenous bolus morphine for postoperative analgesia in infants". Can J Anaesth 43 (12): 1203–10. doi:10.1007/BF03013425. PMID 8955967.
- ↑ Agaram R, Douglas MJ, McTaggart RA, Gunka V. Inadequate pain relief with labour epidurals: a multivariate analysis of associated factors. Int J Obstet Anesth. 2009.18(1):10–4.
- ↑ Norris MC, Leighton BL, DeSimone CA (1989). "Needle bevel direction and headache after inadvertent dural puncture". Anesthesiology 70 (5): 729–31. doi:10.1097/00000542-198905000-00002. PMID 2655500.
- ↑ Sprigge JS, Harper SJ (2008). "Accidental dural puncture and post dural puncture headache in obstetric anaesthesia: presentation and management: a 23-year survey in a district general hospital". Anaesthesia 63 (1): 36–43. doi:10.1111/j.1365-2044.2007.05285.x. PMID 18086069.
- 1 2 Wilson IH, Allman KG (2006). Oxford handbook of anaesthesia. Oxford: Oxford University Press. p. 20. ISBN 0-19-856609-3.
- ↑ Wang, Yen-Feng; Wang, Shuu-Jiun (March 10, 1994). "Headache associated with low CSF pressure". MedLink.
- ↑ Jonas K, Johansson LM, Nissen E, Ejdebäck M, Ransjö-Arvidson AB, Uvnäs-Moberg K (2009). "Effects of Intrapartum Oxytocin Administration and Epidural Analgesia on the Concentration of Plasma Oxytocin and Prolactin, in Response to Suckling During the Second Day Postpartum". Breastfeed Med 4 (2): 71–82. doi:10.1089/bfm.2008.0002. PMID 19210132.
- ↑ Shih CK, Wang FY, Shieh CF, Huang JM, Lu IC, Wu LC, Lu DV (2012). "Soft catheters reduce the risk of intravascular cannulation during epidural block—a retrospective analysis of 1,117 cases in a medical center". Kaohsiung J. Med. Sci. 28 (7): 373–6. doi:10.1016/j.kjms.2012.02.004. PMID 22726899.
- ↑ Giebler RM, Scherer RU, Peters J (1997). "Incidence of neurologic complications related to thoracic epidural catheterization". Anesthesiology 86 (1): 55–63. doi:10.1097/00000542-199701000-00009. PMID 9009940.
- ↑ Clarkson CW, Hondeghem LM (1985). "Mechanism for bupivacaine depression of cardiac conduction: fast block of sodium channels during the action potential with slow recovery from block during diastole". Anesthesiology 62 (4): 396–405. doi:10.1097/00000542-198504000-00006. PMID 2580463.
- ↑ Groban L, Deal DD, Vernon JC, James RL, Butterworth J (2001). "Cardiac resuscitation after incremental overdosage with lidocaine, bupivacaine, levobupivacaine, and ropivacaine in anesthetized dogs". Anesth Analg 92 (1): 37–43. doi:10.1097/00000539-200101000-00008. PMID 11133597.
- 1 2 3 4 "Epidurals and risk: it all depends [May 2007; 159–3]".
- ↑ Scott DA, Beilby DS, McClymont C (1995). "Postoperative analgesia using epidural infusions of fentanyl with bupivacaine. A prospective analysis of 1,014 patients". Anesthesiology 83 (4): 727–37. doi:10.1097/00000542-199510000-00012. PMID 7574052.
- 1 2 Wilson IH, Allman KG (2006). Oxford handbook of anaesthesia. Oxford: Oxford University Press. p. 21. ISBN 0-19-856609-3.
- ↑ Rice I, Wee MY, Thomson K (2004). "Obstetric epidurals and chronic adhesive arachnoiditis". Br J Anaesth 92 (1): 109–20. doi:10.1093/bja/aeh009. PMID 14665562.
- ↑ Wilson IH, Allman KG (2006). Oxford handbook of anaesthesia. Oxford: Oxford University Press. p. 1039. ISBN 0-19-856609-3.
- ↑ Whitehead SA, Nussey S (2001). Endocrinology: an integrated approach. Oxford: BIOS. p. 122. ISBN 1-85996-252-1.
- ↑ Gregory M. "Endocrine System: Posterior Pituitary". Retrieved 5 July 2011.
- ↑ Takayanagi Y, Yoshida M, Bielsky IF, Ross HE, Kawamata M, Onaka T, Yanagisawa T, Kimura T, Matzuk MM, Young LJ, Nishimori K (2005). "Pervasive social deficits, but normal parturition, in oxytocin receptor-deficient mice". Proceedings of the National Academy of Sciences of the United States of America 102 (44): 16096–101. doi:10.1073/pnas.0505312102. PMC 1276060. PMID 16249339.
- ↑ Mayo Clinic Staff. "Labor and Delivery: Pain Medications – Epidural Block". Retrieved 2011-07-05.
- ↑ Seyb ST, Berka RJ, Socol ML, Dooley SL (1999). "Risk of cesarean delivery with elective induction of labour at term in nulliparous women". Obstet Gynecol 94 (4): 600–607. doi:10.1016/S0029-7844(99)00377-4. PMID 10511367.
- ↑ Liu EHC, Sia ATH (2004). "Rates of caesarean section and instrumental vaginal delivery in nulliparous women after low concentration epidural infusions or opioid analgesia: systematic review". BMJ 328 (7453): 1410–1415. doi:10.1136/bmj.38097.590810.7C.
- ↑ Halpern SH, Muir H, Breen TW, Campbell DC, Barrett J, Liston R, Blanchard JW (2004). "A multicenter randomized controlled trial comparing patient-controlled epidural with intravenous analgesia for pain relief in labor". Anesth Analg 99 (5): 1532–1538. doi:10.1213/01.ANE.0000136850.08972.07. PMID 15502060.
- ↑ Wong CA, Scavone BM, Peaceman AM, McCarthy RJ, Sullivan JT, Diaz NT, Yaghmour E, Marcus RJ, Sherwani SS, Sproviero MT, Yilmaz M, Patel R, Robles C, Grouper S (2005). "The risk of cesarean delivery with neuraxial analgesia given early versus late in labor". N Engl J Med 352 (7): 655–665. doi:10.1056/NEJMoa042573. PMID 15716559.
- ↑ Ohel G, Gonen R, Vaida S, Barak S, Gaitini L (2006). "Early versus late initiation of epidural analgesia in labor: does it increase the risk of cesarean section? A randomized trial". Am J Obstet Gynecol 194 (3): 600–605. doi:10.1016/j.ajog.2005.10.821. PMID 16522386.
- ↑ Wong CA, McCarthy RJ, Sullivan JT, Scavone BM, Gerber SE, Yaghmour EA (2009). "Early compared with late neuraxial analgesia in nulliparous labor induction: a randomized controlled trial". Obstet Gynecol 113 (5): 1066–74. doi:10.1097/AOG.0b013e3181a1a9a8. PMID 19384122.
- ↑ Corning, JL (1885). "Spinal anaesthesia and local medication of the cord". New York Medical Journal 42: 483–5.
- ↑ Marx GF (1994). "The first spinal anesthesia. Who deserves the laurels?". Regional Anesthesia 19 (6): 429–30. PMID 7848956.
- ↑ Pagés, F (1921). "Anestesia metamérica". Revista de Sanidad Militar (in Spanish) 11: 351–4.
- ↑ Dogliotti, AM (1933). "Research and clinical observations on spinal anesthesia: with special reference to the peridural technique" (PDF). Anesthesia & Analgesia 12 (2): 59–65. doi:10.1213/00000539-193301000-00014.
- ↑ Edwards, WB; Hingson, RA (1942). "Continuous caudal anesthesia in obstetrics". American Journal of Surgery 57 (3): 459–64. doi:10.1016/S0002-9610(42)90599-3.
- ↑ Hingson, RA; Edwards, WB (1943). "Continuous Caudal Analgesia in Obstetrics". Journal of the American Medical Association 121 (4): 225–9. doi:10.1001/jama.1943.02840040001001.
- ↑ Martinez Curbelo M (1949). "Continuous peridural segmental anesthesia by means of a ureteral catheter". Curr Res Anesth Analg 28 (1): 13–23. doi:10.1213/00000539-194901000-00002. PMID 18105827.
Further reading
- Boqing Chen and Patrick M. Foye, UMDNJ: New Jersey Medical School, Epidural Steroid Injections: Non-surgical Treatment of Spine Pain, eMedicine: Physical Medicine and Rehabilitation (PM&R), August 2005. Also available online.
- Leighton BL, Halpern SH (2002). "The effects of epidural analgesia on labor, maternal, and neonatal outcomes: a systematic review". Am J Obstet Gynecol 186 (5 Suppl Nature): S69–77. PMID 12011873.
- Zhang J, Yancey MK, Klebanoff MA, Schwarz J, Schweitzer D (2001). "Does epidural analgesia prolong labor and increase risk of cesarean delivery? A natural experiment". Am J Obstet Gynecol 185 (1): 128–34. doi:10.1067/mob.2001.113874. PMID 11483916.
External links
| Wikimedia Commons has media related to Epidural. |
- Epidurals for pain relief in labour Comprehensive information with women's stories – informedhealthonline.org, Accessed July 2, 2009.
- What Is An Epidural Headache? – Epidural Headaches Explained
- MedlinePlus Encyclopedia
| ||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
-solution.jpg)




|