Ovarian cyst
| Ovarian cyst | |
|---|---|
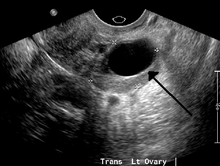
 A simple ovarian cyst of probably follicular origin | |
| Classification and external resources | |
| Specialty | Gynecology |
| ICD-10 | N83.0-N83.2 |
| ICD-9-CM | 620.0-620.2 |
| DiseasesDB | 9433 |
| MedlinePlus | 001504 |
| eMedicine | med/1699 emerg/352 |
| MeSH | D010048 |
An ovarian cyst is any fluid-filled sac within the ovary. Often they cause no symptoms. Occasionally they may produce bloating, lower abdominal pain, or lower back pain. If the cyst either breaks open or causes twisting of the ovary severe pain may occur. This may result in vomiting or feeling faint. The majority of cysts are, however, harmless.[1]
Most ovarian cysts are related to ovulation being either follicular cysts or corpus luteum cysts. Other types include cysts due to endometriosis, dermoid cysts, and cystadenomas. Many small cysts occur in both ovaries in polycystic ovarian syndrome. Pelvic inflammatory disease may also result in cysts. Rarely cysts may be a form of ovarian cancer. Diagnosis is undertaken by pelvic examination with an ultrasound or other testing used to gather further details.[1]
Often cysts are simply observed over time. If they cause pain, medications such as paracetamol (acetaminophen) or ibuprofen may be used. Hormonal birth control may be used to prevent further cysts in those who are frequently affected.[1] However, evidence does not support birth control as a treatment of current cysts.[2] If they do not go away after several months, get larger, look unusual, or cause pain they may be removed by surgery.[1]
Most women of reproductive age develop small cysts each month. Large cysts that cause problems occur in about 8% of women before menopause.[1] Ovarian cysts are present in about 16% of women after menopause and if present are more likely to be cancer.[1][3]
Signs and symptoms
Some or all of the following symptoms may be present, though it is possible not to experience any symptoms:[4]
- Abdominal pain. Dull aching pain within the abdomen or pelvis, especially during intercourse.
- Uterine bleeding. Pain during or shortly after beginning or end of menstrual period; irregular periods, or abnormal uterine bleeding or spotting.
- Fullness, heaviness, pressure, swelling, or bloating in the abdomen.
- When a cyst ruptures from the ovary, there may be sudden and sharp pain in the lower abdomen on one side.
- Change in frequency or ease of urination (such as inability to fully empty the bladder), or difficulty with bowel movements due to pressure on adjacent pelvic anatomy.
- Constitutional symptoms such as fatigue, headaches
- Nausea or vomiting
- Weight gain
Other symptoms may depend on the cause of the cysts:[4]
- Symptoms that may occur if the cause of the cysts is polycystic ovarian syndrome (PCOS) may include increased facial hair or body hair, acne, obesity and infertility.
- If the cause is endometriosis, then periods may be heavy, and intercourse painful.
The effect of cysts not related to PCOS on fertility is unclear.[5]
Cyst rupture
A ruptured ovarian cyst is usually self-limiting, and only requires keeping an eye on the situation and pain medications. The main symptom is abdominal pain, but they can also be asymptomatic. The pain may last from a few days to several weeks.[6] Rupture of large ovarian cysts can cause lots of bleeding inside the abdominal cavity and in some cases shock.
Ovarian torsion
Ovarian cysts increase the risk for ovarian torsion, cysts larger than 4 cm are associated with approximately 17% risk. The torsion can cause obstruction of blood flow and lead to infarction.[7]
Diagnosis
Ovarian cysts are usually diagnosed by either ultrasound, CT scan or MRI, and correlated with clinical presentation and endocrinologic tests as appropriate.
Ultrasound
Follow-up imaging in women of reproductive age for incidentally discovered simple cysts on ultrasound is not needed until 5 cm, as these are usually normal ovarian follicles. For simple cysts greater than 5 cm but less than 7 cm in premenopausal females, cysts should be followed yearly. For simple cysts greater than 7 cm, further imaging with MRI or surgical assessment is mandated as, because of their large size, these cysts cannot be reliably assessed by ultrasound alone. The primary concern for larger cysts is the potential for non-visualization of soft tissue nodularity or thickened septation at their posterior wall due to limited penetrance of the ultrasound beam. For the corpus luteum, a dominant ovulating follicle that typically appears as a cyst with circumferentially thickened walls and crenulated inner margins, follow up is not needed if the cyst is less than 3 cm in diameter. In postmenopausal patients, any simple cyst greater than 1 cm but less than 7 cm needs yearly follow-up, while those greater than 7 cm need MRI or surgical evaluation, similar to reproductive age females.[8]

For incidentally discovered dermoids, diagnosed on ultrasound by their pathognomonic echogenic fat, either surgical removal or yearly follow up is indicated, regardless of patient age. For peritoneal inclusion cysts, which have a crumpled tissue-paper appearance and tend to follow the contour of adjacent organs, follow up is based on clinical history. Hydrosalpinx, or fallopian tube dilation, can be mistaken for an ovarian cyst due to its anechoic appearance. Follow-up for this is also based on clinical presentation.[8]
For multiloculate cysts with thin septation less than 3 mm, surgical evaluation is recommended. The presence of multiloculation suggests a neoplasm, although the thin septation implies that the neoplasm is benign. For any thickened septation, nodularity, or vascular flow on color Doppler assessment, surgical removal should be considered due to concern for malignancy.[8]
Scoring systems
There are several systems to assess risk of an ovarian cyst of being an ovarian cancer, including the RMI (risk of malignancy index), LR2 and SR (simple rules). Sensitivities and specificities of these systems are given in tables below:[9]
| Scoring systems | Premenopausal | Postmenopausal | ||
|---|---|---|---|---|
| Sensitivity | Specificity | Sensitivity | Specificity | |
| RMI I | 44% | 95% | 79% | 90% |
| LR2 | 85% | 91% | 94% | 70% |
| SR | 93% | 83% | 93% | 76% |
Ovarian cysts may be classified according to whether they are a variant of the normal menstrual cycle, referred to as a functional or follicular cyst.[4]
Ovarian cysts are considered large when they are over 5 cm and giant when they are over 15 cm. In children ovarian cysts reaching above the level of the umbilicus are considered giant.
Functional
Functional cysts form as a normal part of the menstrual cycle. There are several types of cysts:
- Follicular cyst, the most common type of ovarian cyst. In menstruating women, a follicle containing the ovum (unfertilized egg) will rupture during ovulation. If this does not occur, a follicular cyst of more than 2.5 cm diameter may result.[4]
- Corpus luteum cysts appear after ovulation. The corpus luteum is the remnant of the follicle after the ovum has moved to the fallopian tubes. This normally degrades within 5–9 days. A corpus luteum that is more than 3 cm is defined as cystic.[4]
- Theca lutein cysts occur within the thecal layer of cells surrounding developing oocytes. Under the influence of excessive hCG, thecal cells may proliferate and become cystic. This is usually on both ovaries.[4]
Non-functional


Non-functional cysts may include the following:
- An ovary with many cysts, which may be found in normal women, or within the setting of polycystic ovary syndrome.
- Cysts caused by endometriosis, known as chocolate cysts.
- Hemorrhagic ovarian cyst
- Dermoid cyst
- Ovarian serous cystadenoma
- Ovarian mucinous cystadenoma
- Paraovarian cyst
- Cystic adenofibroma
- Borderline tumoral cysts
Associated medical conditions
In juvenile hypothyroidism multicystic ovaries are present in about 75% of cases, while large ovarian cysts and elevated ovarian tumor marks are one of the symptoms of the Van Wyk and Grumbach syndrome.[10]
The CA-125 marker in children and adolescents can be frequently elevated even in absence of malignancy and conservative management should be considered.
Polycystic ovarian syndrome involves the development of multiple small cysts in both ovaries due to an elevated ratio of leutenizing hormone to follicle stimulating hormone, typically more than 25 cysts in each ovary, or an ovarian volume of greater than 10 mL.[11]
Larger bilateral cysts can develop as a result of fertility treatment due to elevated levels of HCG, as can be seen with the use of clomifene for follicular induction, in extreme cases resulting in a condition known as ovarian hyperstimulation syndrome.[12] Certain malignancies can mimic the effects of clomifene on the ovaries, also due to increased HCG, in particular gestational trophoblastic disease. Ovarian hyperstimulation occurs more often with invasive moles and choriocarcinoma than complete molar pregnancies.[13]
Risk of cancer
A widely recognised method of estimating the risk of malignant ovarian cancer based on initial workup is the risk of malignancy index (RMI).[14] It is recommended that women with an RMI score over 200 should be referred to a centre with experience in ovarian cancer surgery.[15]
The RMI is calculated as follows:[15]
- RMI = ultrasound score x menopausal score x CA-125 level in U/ml.
There are two methods to determine the ultrasound score and menopausal score, with the resultant RMI being called RMI 1 and RMI 2, respectively, depending on what method is used:[15]
| Feature | RMI 1 | RMI 2 |
|---|---|---|
|
Ultrasound abnormalities:
|
|
|
| Menopausal score |
|
|
| CA-125 | Quantity in U/ml | Quantity in U/ml |
An RMI 2 of over 200 has been estimated to have a sensitivity of 74 to 80%, a specificity of 89 to 92% and a positive predictive value of around 80% of ovarian cancer.[15] RMI 2 is regarded as more sensitive than RMI 1.[15]
Treatment
Cysts associated with hypothyroidism or other endocrine problems are managed by treating the underlying condition.
About 95% of ovarian cysts are benign, not cancerous.[16]
Functional cysts and hemorrhagic ovarian cysts usually resolve spontaneously.[17] However the bigger an ovarian cyst is, the less likely it is to disappear on its own.[18] Treatment may be required if cysts persist over several months, grow or cause increasing pain.[19]
Cysts that persist beyond two or three menstrual cycles, or occur in post-menopausal women, may indicate more serious disease and should be investigated through ultrasonography and laparoscopy, especially in cases where family members have had ovarian cancer. Such cysts may require surgical biopsy. Additionally, a blood test may be taken before surgery to check for elevated CA-125, a tumour marker, which is often found in increased levels in ovarian cancer, although it can also be elevated by other conditions resulting in a large number of false positives.[20]
Pain
Pain associated with ovarian cysts may be treated in several ways:
- Pain relievers such as acetaminophen, nonsteroidal anti-inflammatory drugs,[1] or opioids.
- While hormonal birth control prevents the development of new cysts in those who frequently get them,[1] it is not useful for the treatment of current cysts.[2]
Surgery
Some cases require surgery. This may involve removing the cyst, or one or both ovaries.[21] Technique is typically laparoscopic, unless the cyst is particularly large, or if pre-operative imaging suggests malignancy or complex anatomy.[22] In certain situations, the cyst is entirely removed, while with cysts with low recurrence risk, younger patients, or which are in anatomically eloquent areas of the pelvis, they can be drained.[23][24] Features that may indicate the need for surgery include:[25]
- Persistent complex ovarian cysts
- Persistent cysts that are causing symptoms
- Complex ovarian cysts larger than 5 cm
- Simple ovarian cysts larger 10 centimeters or larger than 5 cm in postmenopausal patients
- Women who are menopausal or perimenopausal
Frequency
Most women of reproductive age develop small cysts each month. Large cysts that cause problems occur in about 8% of women before menopause.[1] Ovarian cysts are present in about 16% of women after menopause and if present are more likely to be cancer.[1][3]
Benign ovarian cysts are common in asymptomatic premenarchal girls and found in approximately 68% of ovaries of girls 2–12 years old and in 84% of ovaries of girls 0–2 years old. Most of them are smaller than 9 mm while about 10-20% are larger macrocysts. While the smaller cysts mostly disappear within 6 months the larger ones appear to be more persistent.[26][27]
References
- 1 2 3 4 5 6 7 8 9 10 "Ovarian cysts". Office on Women's Health. November 19, 2014. Retrieved 27 June 2015.
- 1 2 Grimes, DA; Jones, LB; Lopez, LM; Schulz, KF (29 April 2014). "Oral contraceptives for functional ovarian cysts.". The Cochrane database of systematic reviews 4: CD006134. doi:10.1002/14651858.CD006134.pub5. PMID 24782304.
- 1 2 Mimoun, C; Fritel, X; Fauconnier, A; Deffieux, X; Dumont, A; Huchon, C (December 2013). "[Epidemiology of presumed benign ovarian tumors].". Journal de gynecologie, obstetrique et biologie de la reproduction 42 (8): 722–9. doi:10.1016/j.jgyn.2013.09.027. PMID 24210235.
- 1 2 3 4 5 6 Helm, William. "Ovarian Cysts". Retrieved 30 August 2013.
- ↑ Legendre, G; Catala, L; Morinière, C; Lacoeuille, C; Boussion, F; Sentilhes, L; Descamps, P (March 2014). "Relationship between ovarian cysts and infertility: what surgery and when?". Fertility and Sterility 101 (3): 608–14. doi:10.1016/j.fertnstert.2014.01.021. PMID 24559614.
- ↑ Ovarian Cyst Rupture at Medscape. Authors: Nathan Webb and David Chelmow. Updated: Nov 30, 2012
- ↑ "Ovarian Cysts Causes, Symptoms, Diagnosis, and Treatment". eMedicineHealth.com.
- 1 2 3 Levine, D; Brown, DL; Andreotti, RF; Benacerraf, B; Benson, CB; Brewster, WR; Coleman, B; Depriest, P; Doubilet, PM; Goldstein, SR; Hamper, UM; Hecht, JL; Horrow, M; Hur, HC; Marnach, M; Patel, MD; Platt, LD; Puscheck, E; Smith-Bindman, R (September 2010). "Management of asymptomatic ovarian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound Consensus Conference Statement.". Radiology 256 (3): 943–54. doi:10.1148/radiol.10100213. PMID 20505067.
- ↑ Kaijser J, Sayasneh A, Van Hoorde K, Ghaem-Maghami S, Bourne T, Timmerman D, Van Calster B (2013). "Presurgical diagnosis of adnexal tumours using mathematical models and scoring systems: a systematic review and meta-analysis". Human Reproduction Update 20 (3): 449–462. doi:10.1093/humupd/dmt059. ISSN 1355-4786. PMID 24327552.
- ↑ Durbin KL, Diaz-Montes T, Loveless MB (2011). "Van wyk and grumbach syndrome: An unusual case and review of the literature". Journal of pediatric and adolescent gynecology 24 (4): e93–6. doi:10.1016/j.jpag.2010.08.003. PMID 21600802.
- ↑ Dewailly, D; Lujan, ME; Carmina, E; Cedars, MI; Laven, J; Norman, RJ; Escobar-Morreale, HF (May 2014). "Definition and significance of polycystic ovarian morphology: a task force report from the Androgen Excess and Polycystic Ovary Syndrome Society.". Human Reproduction Update 20 (3): 334–52. doi:10.1093/humupd/dmt061. PMID 24345633.
- ↑ Altinkaya, SO; Talas, BB; Gungor, T; Gulerman, C (October 2009). "Treatment of clomiphene citrate-related ovarian cysts in a prospective randomized study. A single center experience.". The journal of obstetrics and gynaecology research 35 (5): 940–5. doi:10.1111/j.1447-0756.2009.01041.x. PMID 20149045.
- ↑ Suzuki, H; Matsubara, S; Uchida, S; Ohkuchi, A (October 2014). "Ovary hyperstimulation syndrome accompanying molar pregnancy: case report and review of the literature.". Archives of gynecology and obstetrics 290 (4): 803–6. doi:10.1007/s00404-014-3319-0. PMID 24966119.
- ↑ NICE clinical guidelines Issued: April 2011. Guideline CG122. Ovarian cancer: The recognition and initial management of ovarian cancer, Appendix D: Risk of malignancy index (RMI I).
- 1 2 3 4 5 EPITHELIAL OVARIAN CANCER SECTION 3: DIAGNOSIS from The Scottish Intercollegiate Guidelines Network. Guideline No 75. October 2003.ISBN 1899893 93 8
- ↑ http://www.nhs.uk/Conditions/Ovarian-cyst/Pages/Symptoms.aspx
- ↑ V.T. (14 May 2014). Understanding Ovarian Cyst. V.T. pp. 25–. GGKEY:JTX84XQARW9.
- ↑ Edward I. Bluth (2000). Ultrasound: A Practical Approach to Clinical Problems. Thieme. p. 190. ISBN 978-0-86577-861-0.
- ↑ Susan A. Orshan (2008). Maternity, Newborn, and Women's Health Nursing: Comprehensive Care Across the Lifespan. Lippincott Williams & Wilkins. p. 161. ISBN 978-0-7817-4254-2.
- ↑ MedlinePlus Encyclopedia CA-125
- ↑ "HealthHints: Gynecologic Health (January/February, 2003)". Texas AgriLife Extension Service: HealthHints.
- ↑ Surgit, O; Inegol Gumus, I (2014). "Single-port Laparoscopic Total Hysterectomy and Bilateral Salpingo-oopherectomy Combined with Burch Colposuspension.". Acta chirurgica Belgica 114 (4): 0. PMID 26021429.
- ↑ Cho, MJ; Kim, DY; Kim, SC (October 2015). "Ovarian Cyst Aspiration in the Neonate: Minimally Invasive Surgery.". Journal of pediatric and adolescent gynecology 28 (5): 348–53. doi:10.1016/j.jpag.2014.10.003. PMID 26148782.
- ↑ Nohuz, E (11 December 2015). "[How I do…the aspiration of an adnexal cyst without iterative needle punctures neither irrigation-aspiration device during a laparoscopy].". Gynecologie, obstetrique & fertilite 44: 63–6. doi:10.1016/j.gyobfe.2015.11.001. PMID 26701109.
- ↑ Ovarian cysts from MedlinePlus. Update Date: 2/26/2012. Updated by: Linda J. Vorvick and Susan Storck. Also reviewed by David Zieve
- ↑ Cohen HL, Eisenberg P, Mandel F, Haller JO (1992). "Ovarian cysts are common in premenarchal girls: A sonographic study of 101 children 2-12 years old". AJR. American journal of roentgenology 159 (1): 89–91. doi:10.2214/ajr.159.1.1609728. PMID 1609728.
- ↑ Qublan HS, Abdel-hadi J (2000). "Simple ovarian cysts: Frequency and outcome in girls aged 2-9 years". Clinical and experimental obstetrics & gynecology 27 (1): 51–3. PMID 10758801.