Niacin
| |||
| Names | |||
|---|---|---|---|
| IUPAC name
pyridine-3-carboxylic acid[1] | |||
| Systematic IUPAC name
Pyridine-3-carboxylic acid[2] | |||
| Other names
Nicotinic Acid Bionic Vitamin B3 | |||
| Identifiers | |||
| 59-67-6 | |||
| 3DMet | B00073 | ||
| 109591 | |||
| ChEBI | CHEBI:15940 | ||
| ChEMBL | ChEMBL573 | ||
| ChemSpider | 913 | ||
| DrugBank | DB00627 | ||
| EC Number | 200-441-0 | ||
| 3340 | |||
| 1588 | |||
| Jmol interactive 3D | Image Image | ||
| KEGG | D00049 | ||
| MeSH | Niacin | ||
| PubChem | 938 | ||
| RTECS number | QT0525000 | ||
| UNII | 2679MF687A | ||
| |||
| |||
| Properties | |||
| C 6NH 5O 2 | |||
| Molar mass | 123.1094 g mol−1 | ||
| Appearance | White, translucent crystals | ||
| Density | 1.473 g cm−3 | ||
| Melting point | 237 °C; 458 °F; 510 K | ||
| 18 g L−1 | |||
| log P | 0.219 | ||
| Acidity (pKa) | 2.0,4.85 | ||
| Isoelectric point | 4.75 | ||
| Refractive index (nD) |
1.4936 | ||
| 0.1271305813 D | |||
| Thermochemistry | |||
| Std enthalpy of formation (ΔfH |
−344.9 kJ mol−1 | ||
| Std enthalpy of combustion (ΔcH |
−2.73083 MJ mol−1 | ||
| Pharmacology | |||
| ATC code | C04 C10AD02 | ||
| Intramuscular, Oral | |||
| Pharmacokinetics: | |||
| 20–45 min | |||
| Hazards | |||
| EU classification (DSD) |
| ||
| R-phrases | R36/37/38 | ||
| S-phrases | S26, S36 | ||
| NFPA 704 | |||
| Flash point | 193 °C (379 °F; 466 K) | ||
| 365 °C (689 °F; 638 K) | |||
| Except where otherwise noted, data are given for materials in their standard state (at 25 °C [77 °F], 100 kPa). | |||
| | |||
| Infobox references | |||



Niacin (also known as vitamin B3 or nicotinic acid) is an organic compound with the formula C
6H
5NO
2 and, depending on the definition used, one of the 20 to 80 essential human nutrients. Pharmaceutical and supplemental niacin are primarily used to treat hypercholesterolemia (high cholesterol) and pellagra (niacin deficiency). Insufficient niacin in the diet can cause nausea, skin and mouth lesions, anemia, headaches, and tiredness. The lack of niacin may also be observed in pandemic deficiency disease, which is caused by a lack of five crucial vitamins (niacin, vitamin C, thiamin, vitamin D, and vitamin A) and is usually found in areas of widespread poverty and malnutrition. Niacin has not been found to be useful in decreasing the risk of cardiovascular disease in those already on a statin[3] but appears to be effective in those not taking a statin.[4]
This colorless, water-soluble solid is a derivative of pyridine, with a carboxyl group (COOH) at the 3-position. Other forms of vitamin B3 include the corresponding amide and nicotinamide ("niacinamide"), where the carboxyl group has been replaced by a carboxamide group (CONH
2), as well as more complex amides and a variety of esters. Nicotinic acid and niacinamide are convertible to each other with steady world demand rising from 8,500 tonnes per year in the 1980s to 40,000 in recent years.[5]
Niacin cannot be directly converted to nicotinamide, but both compounds are precursors of the coenzymes nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP) in vivo.[6] NAD converts to NADP by phosphorylation in the presence of the enzyme NAD+ kinase. NADP and NAD are coenzymes for many dehydrogenases, participating in many hydrogen transfer processes.[7] NAD is important in catabolism of fat, carbohydrate, protein, and alcohol, as well as cell signaling and DNA repair, and NADP mostly in anabolism reactions such as fatty acid and cholesterol synthesis.[7] High energy requirements (brain) or high turnover rate (gut, skin) organs are usually the most susceptible to their deficiency.[8] Although the two are identical in their vitamin activity, nicotinamide does not have the same pharmacological effects (lipid modifying effects) as niacin. Nicotinamide does not reduce cholesterol or cause flushing.[9] Niacin is involved in both DNA repair and the production of steroid hormones in the adrenal gland.
Dietary needs
One recommended daily allowance of niacin is 2–12 mg/day for children, 14 mg/day for women, 16 mg/day for men, and 18 mg/day for pregnant or breast-feeding women.[10] Tolerable upper intake levels (UL) for adult men and women is considered to be 35 mg/day by the Dietary Reference Intake system to avoid flushing. In general, niacin status is tested through urinary biomarkers,[11] which are believed to be more reliable than plasma levels.[12]
Deficiency
Between 1906 and 1940 more than 3 million Americans were affected by pellagra with more than 100,000 deaths. Dr. Joseph Goldberger was assigned to study pellagra by the Surgeon General of the United States and produced good results. In the late 1930s, studies by Dr. Tom Spies, Marion Blankenhorn, and Clark Cooper established that niacin cured pellagra in humans. The disease was greatly reduced as a result.
At present, niacin deficiency is sometimes seen in developed countries, and it is usually apparent in conditions of poverty, malnutrition, and chronic alcoholism.[13] It also tends to occur in areas where people eat maize (corn) as a staple food, since it is the only grain low in digestible niacin. A special cooking technique called nixtamalization is needed to increase the bioavailability of niacin during maize meal/flour production.
Mild niacin deficiency has been shown to slow metabolism, causing decreased tolerance to cold.
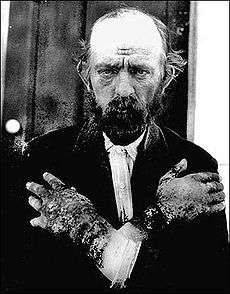
Severe deficiency of niacin in the diet causes the disease pellagra, which is characterized by diarrhea, dermatitis, and dementia, as well as “Casal's necklace” lesions on the lower neck, hyperpigmentation, thickening of the skin, inflammation of the mouth and tongue, digestive disturbances, amnesia, delirium, and eventually death, if left untreated.[14] Common psychiatric symptoms of niacin deficiency include irritability, poor concentration, anxiety, fatigue, restlessness, apathy, and depression.[14] Studies have indicated that, in patients with alcoholic pellagra, niacin deficiency may be an important factor influencing both the onset and severity of this condition. Patients with alcoholism typically experience increased intestinal permeability, leading to negative health outcomes.
Hartnup’s disease is a hereditary nutritional disorder resulting in niacin deficiency.[14] This condition was first identified in the 1950s by the Hartnup family in London. It is due to a deficit in the intestines and kidneys, making it difficult for the body to break down and absorb dietary tryptophan. The resulting condition is similar to pellagra, including symptoms of red, scaly rash, and sensitivity to sunlight. Oral niacin is given as a treatment for this condition in doses ranging from 40–200 mg, with a good prognosis if identified and treated early.[14] Niacin synthesis is also deficient in carcinoid syndrome, because of metabolic diversion of its precursor tryptophan to form serotonin.
Medical uses
Abnormal lipids
Niacin is used in addition to other lipid-lowering medication.[15]
A 2014 review of niacin did not find that it affected either cardiovascular disease or risk of death in those already taking a statin.[3] Niacin alone appears to reduce the risk of cardiovascular disease.[16][17]
The National Cholesterol Education Program (NCEP) in 2002 recommended niacin alone for cardiovascular and atherogenic dyslipidemia in mild or normal LDL levels or in combination for higher HDL levels.[18]
Treatment of deficiency
Nicotinic acid has been also approved by the FDA for pellagra.
Other uses
Nicotinic acid has been used as a topical vasodilator or skin cream. Moreover, niacin is applied topically as a lip plumper, due to its vasodilation effect. The vasodilated lips are slightly swollen and redder, making them appear "full-blooming," which is typically desired.[19]
Contraindications
Niacin is contraindicated with active liver disease, persistent elevated serum transaminases, active peptic ulcer disease, or arterial bleeding.[20]
Side effects
The most common adverse effects are flushing (e.g., warmth, redness, itching and/or tingling), headache, pain, abdominal pain, diarrhea, dyspepsia, nausea, vomiting, rhinitis, pruritus and rash. These can be minimized by initiating therapy at low dosages, increasing dosage gradually, and avoiding administration on an empty stomach.[20] High doses of niacin often temporarily reduce blood pressure as a result of acute vasodilation.[21] Longer term, high-dose niacin use may persistently lower blood pressure in individuals with hypertension, but more research is needed to determine the extent of this effect.[21]
Skin
Pharmacological doses of niacin (1.5 – 6 g per day) lead to side effects that can include dermatological conditions such as skin flushing and itching, dry skin, and skin rashes including eczema exacerbation and acanthosis nigricans.
Facial flushing
Flushing usually lasts for about 15 to 30 minutes, though it can sometimes last up to two hours. It is sometimes accompanied by a prickly or itching sensation, in particular, in areas covered by clothing. Flushing can be blocked by taking 300 mg of aspirin half an hour before taking niacin, by taking one tablet of ibuprofen per day or by co-administering the prostaglandin receptor antagonist laropiprant. Taking niacin with meals also helps reduce this side effect. Acquired tolerance will also help reduce flushing; after several weeks of a consistent dose, most patients no longer experience flushing.[22] Reduction of flushing focuses on altering or blocking the prostaglandin mediated pathway.[23] Slow- or "sustained"-release forms of niacin have been developed to lessen these side effects.[24][25] One study showed the incidence of flushing was significantly lower with a sustained-release formulation,[26] though doses above 2 g per day have been associated with liver damage, in particular, with slow-release formulations.[27]
Prostaglandin (PGD2) is the primary cause of the flushing reaction, with serotonin appearing to have a secondary role in this reaction.[28] The effect is mediated by prostaglandin E2 and D2 due to GPR109A activation of epidermal Langerhans cells and keratinocytes.[29][30] Langerhans cells use cyclooxygenase type 1 (COX-1) for PGE2 production and are more responsible for acute flushing, while keratinocytes are COX-2 dependent and are in active continued vaso-dilation.[31][32] Flushing was often thought to involve histamine, but histamine has been shown not to be involved in the reaction.[28]
Gastrointestinal and hepatic
Gastrointestinal complaints, such as indigestion, nausea and liver failure, have also been reported. Hepatotoxicity is possibly related to metabolism via amidation resulting in NAD production.[33] The time-release form has a lower therapeutic index for lowering serum lipids relative to this form of toxicity.[34]
Metabolic
Although high doses of niacin may elevate blood sugar, thereby worsening diabetes mellitus,[27] recent studies show the actual effect on blood sugar to be only 5–10%. Patients with diabetes who continued to take anti-diabetes drugs containing niacin did not experience major blood glucose changes. Thus overall, niacin continues to be recommended as a drug for preventing cardiovascular disease in patients with diabetes.
Hyperuricemia is another side effect of taking high-dose niacin, and may exacerbate gout.[35]
Other
Side effects of cardiac arrhythmias have also been reported.[27] Increased PT and decreased platelet count have been reported, therefore these should be monitored closely in patients who are also taking anticoagulants.[20]
Particularly the time-release variety, at extremely high doses, can cause acute toxic reactions.[36] Extremely high doses of niacin can also cause niacin maculopathy, a thickening of the macula and retina, which leads to blurred vision and blindness. This maculopathy is reversible after niacin intake ceases.[37]
In pregnancy
Niacin in doses used to lower cholesterol levels has been associated with birth defects in laboratory animals, with possible consequences for infant development in pregnant women.[27]
Pharmacology
Pharmacodynamics
Niacin therapeutic effect is mostly through its binding to G protein coupled receptors, niacin receptor 1 (NIACR1) and niacin receptor 2 (NIACR2), that are highly expressed in adipose tissue, spleen, immune cells and keratinocytes but not in other expected organs such as liver, kidney, heart or intestine.[38][39] A carboxyl group of nicotinic acid is a crucial moiety for the binding in which both oxygen atoms of the carboxyl group can bind to positively charged residue of arginine 111 of transmembrane helices (TMH) 3 via electrostatic interaction. Moreover, nitrogen atom of pyridine ring of nicotinic acid interacts with serine 178 of extracellular loop (ECL) 2 by embedding between TMH2/ECL1 junction and TMH7.[19] NIACR1 and NIACR2 inhibit cyclic adenosine monophosphate (cAMP) production and thus fat breakdown in adipose tissue and free fatty acids available for liver to produce triglycerides and very-low-density lipoproteins (VLDL) and consequently low-density lipoprotein (LDL) or "bad" cholesterol.[33][40] Decrease in free fatty acids also suppress hepatic expression of apolipoprotein C3 (APOC3) and PPARg coactivator-1b (PGC-1b) thus increase VLDL turn over and reduce its production.[41] It also inhibits diacylglycerol acyltransferase-2 (important hepatic TG synthesis).
The mechanism behind increasing HDL is not totally understood but it seems to be done in various ways. Niacin increases apolipoprotein A1 levels due to anti catabolic effects resulting in higher reverse cholesterol transport. It also inhibits HDL hepatic uptake, down-regulating production of the cholesterol ester transfer protein (CETP) gene.[42] Finally, it stimulates the ABCA1 transporter in monocytes and macrophages and up-regulates peroxisome proliferator-activated receptor γ results in reverse cholesterol transport.[43]
It reduces secondary outcomes associated with atherosclerosis, such as low density lipoprotein cholesterol (LDL), very low-density lipoprotein cholesterol (VLDL-C), and triglycerides (TG), but increases high density lipoprotein cholesterol (HDL).[42] Despite the importance of other cardiovascular risk factors, high HDL was associated with fewer cardiovascular events independent of LDL reduction.[44][45] Other effects include anti-thrombotic and vascular inflammation, improving endothelial function, and plaque stability.[46] Adipokines are the adipocytes’ produced mediators. Some adipokines such as tumor necrosis factor (TNF)-a, interleukins and chemokines, have pro-inflammatory effect and some others such as adiponectin have anti-inflammatory effect that regulates inflammatory process, decrease vascular progression and atherosclerosis.[47]
Niacin also appears to upregulate brain-derived neurotrophic factor (BDNF) and tropomyosin receptor kinase B (TrkB) expression.[48]
Research has been able to show the function of niacin in the pathway lipid metabolism. It is seen that this vitamin can decrease the synthesis of apoB-containing lipoproteins such as VLDL, LDL, IDL and Lipoprotein (a) via several mechanisms: (1) Directly inhibiting the action of DGAT2, a key enzyme for triglyceride synthesis; (2) It has the ability to bind to the receptor HCAR2 thereby decreasing lipolysis and FFA flux to the liver for triglyceride synthesis;[11] and (3) increased apoB catabolism. On the other hand, HDL cholesterol levels are increased by niacin through direct and indirect pathways. (4) Niacin decreases CETP mass and activity, and this synergistic effect with the decrease in triglyceride levels, can indirectly raise HDL cholesterol levels. The study has also been able to show direct effects on the beta chain of ATP synthase (5) and on production (6) and hepatic uptake (7) of apoA-I also increase HDL cholesterol levels. Thus by affecting the pathway reducing lipid levels help in reducing CVD.[49]
Pharmacokinetics

Biosynthesis
The liver can synthesize niacin from the essential amino acid tryptophan, requiring 60 mg of tryptophan to make one mg of niacin.[50] Riboflavin, vitamin B6 and iron are required in some of the reactions involved in the conversion of tryptophan to NAD.
Physical and chemical properties
Laboratory synthesis
Several thousand tons of niacin are manufactured each year, starting from 3-methylpyridine.
Preparations
Many preparations of niacin are available over-the-counter as dietary supplements. Non-prescription extended release niacin, such as Endur-acin, which uses a wax matrix to delay release is available as well.[51][52]
Over-the counter plain niacin has FDA regulatory approval.[53] Some “no flush” types, such as inositol hexanicotinate contain convertible niacin compounds, but have little clinical efficacy in reducing cholesterol levels.[54][55] “Slow release” varieties have higher hepatotoxic activity, hence some types of prescription niacin are not recommended due to potential harm.[56]
Nicotinic acid
Extended release
A prescription extended release niacin, Niaspan, has a film coating that delays release of the niacin, resulting in an absorption over a period of 8–12 hours. The extended release formulations generally reduce vasodilation and flushing side effects, but increase the risk of hepatotoxicity compared to the immediate release forms.[57][58][59]
A formulation of laropiprant (Merck & Co., Inc.) and niacin had previously been approved for use in Europe and marketed as Tredaptive. Laropiprant is a prostaglandin D2 binding drug shown to reduce vasodilatation and flushing up to 73%.[42][60][61][62] The HPS2-THRIVE study,[63] a study sponsored by Merck, showed no additional efficacy of Tredaptive in lowering cholesterol when used together with other statin drugs, but did show an increase in other side effects. The study resulted in the complete withdrawal of Tredaptive from the international market.[64][65]
Inositol hexanicotinate
One form of dietary supplement is inositol hexanicotinate (IHN), which is inositol that has been esterified with niacin on all six of inositol's alcohol groups. IHN is usually sold as "flush-free" or "no-flush" niacin in units of 250, 500, or 1000 mg/tablets or capsules. It is sold as an over-the-counter formulation, and often is marketed and labeled as niacin, thus misleading consumers into thinking they are getting the active form of the medication. While this form of niacin does not cause the flushing associated with the immediate-release products, the evidence that it has lipid-modifying functions is contradictory, at best. As the clinical trials date from the early 1960s (Dorner, Welsh) or the late 1970s (Ziliotto, Kruse, Agusti), it is difficult to assess them by today's standards.[66] One of the last of those studies affirmed the superiority of inositol and xantinol esters of nicotinic acid for reducing serum free fatty acid,[67] but other studies conducted during the same period found no benefit.[68] Studies explain that this is primarily because "flush-free" preparations do not contain any free nicotinic acid. A more recent placebo-controlled trial was small (n=11/group), but results after three months at 1500 mg/day showed no trend for improvements in total cholesterol, LDL-C, HDL-C or triglycerides.[69] Thus, so far there is not enough evidence to recommend IHN to treat dyslipidemia.
Nicotinamide
Nicotinamide may be obtained from the diet where it is present primarily as NAD+ and NADP+. These are hydrolysed in the intestine and the resulting nicotinamide is absorbed either as such, or following its hydrolysis to nicotinic acid. Nicotinamide is present in nature in only small amounts. In unprepared foods, niacin is present mainly in the form of the cellular pyridine nucleotides NAD and NADP. Enzymatic hydrolysis of the co-enzymes can occur during the course of food preparation. Boiling releases most of the total niacin present in sweet corn as nicotinamide (up to 55 mg/kg).[70]
Nicotinamide may be toxic to the liver at doses exceeding 3 g/day for adults.[71]
Food sources
Niacin is found in variety of foods, including liver, chicken, beef, fish, cereal, peanuts, and legumes, and is also synthesized from tryptophan, an essential amino acid found in most forms of protein.
Animal products:
- liver, heart and kidney (9 – 15 mg niacin per 100 grams)
- chicken, chicken breast (6.5 mg)
- beef (5 – 6 mg)
- fish: tuna, salmon, halibut (2.5 – 13 mg)
- eggs (0.1 mg)
- venison (8.43 mg)
Fruits and vegetables:
- avocados (1 mg niacin per 100 grams)
- dates (2 mg)
- tomatoes (0.7 mg)
- leaf vegetables (0.3 – 0.4 mg)
- broccoli (0.6 mg)
- carrots (0.3 – 0.6 mg)
- sweet potatoes (0.5 – 0.6 mg)
- asparagus (0.4 mg)
Seeds:
- nuts (2 mg niacin per 100 grams)
- whole grain products (4 – 29.5 mg)
- legumes (0.4 – 16 mg)
- saltbush seeds
Fungi:
- mushrooms, shiitake mushrooms (3.5 – 4 mg niacin per 100 grams)
- brewer's yeast (36 mg)
Other:
- beer (6 mg per pint,[72] less if filtered)
- Ovaltine (18 mg)
- Peanut butter (15 mg)
- Tofu
- Soy sauce (0.4 mg)
- Vegemite (from spent brewer's yeast) (50 mg niacin per 100 grams)[73]
- Marmite (from spent brewer's yeast) (50 mg niacin per 100 grams)[74]
History
Niacin was first described by chemist Hugo Weidel in 1873 in his studies of nicotine.[75] The original preparation remains useful: The oxidation of nicotine using nitric acid.[76] For the first time, niacin was extracted by Casimir Funk, but he thought that it was thiamine and due to the discovered amine group he coined the term "vitamine". Niacin was extracted from livers by biochemist Conrad Elvehjem in 1937, who later identified the active ingredient, then referred to as the "pellagra-preventing factor" and the "anti-blacktongue factor."[77] Soon after, in studies conducted in Alabama and Cincinnati, Dr. Tom Spies found that nicotinic acid cured the sufferers of pellagra.[78]
Niacin is referred to as vitamin B3 because it was the third of the B vitamins to be discovered. It has historically been referred to as "vitamin PP", "vitamin P-P" and "PP-factor", that are derived from the term "pellagra-preventive factor".[79] When the biological significance of nicotinic acid was realized, it was thought appropriate to choose a name to dissociate it from nicotine, to avoid the perception that vitamins or niacin-rich food contains nicotine, or that cigarettes contain vitamins. The resulting name 'niacin' was derived from nicotinic acid + vitamin.[79]
Carpenter found in 1951 that niacin in corn is biologically unavailable, and can be released only in very alkaline lime water of pH 11.[80]
In 1955, Altschul and colleagues described niacin as having a lipid lowering property.[81] Niacin is the oldest lipid lowering drug.
On April 22, 2014, Pennsylvania State University researchers working with NASA at the Goddard Astrobiology Analytical Laboratory reported[82] of finding niacin within eight CM-2 type carbonaceous chondrite meteorites. The meteorite’s vitamin B3 levels ranged from 30–600 parts per billion, the study reports. Related molecules discovered in the meteorites include pyridine carboxylic acids and pyridine dicarboxylic acids.
References
- ↑ "Niacin". DrugBank: a knowledgebase for drugs, drug actions and drug targets. Retrieved 14 January 2012.
- ↑ CID 938 from PubChem
- 1 2 Keene, D; Price, C; Shun-Shin, MJ; Francis, DP (18 July 2014). "Effect on cardiovascular risk of high density lipoprotein targeted drug treatments niacin, fibrates, and CETP inhibitors: meta-analysis of randomised controlled trials including 117,411 patients.". BMJ (Clinical research ed.) 349: g4379. doi:10.1136/bmj.g4379. PMC 4103514. PMID 25038074.
- ↑ Bruckert, Eric; Labreuche, Julien; Amarenco, Pierre (June 2010). "Meta-analysis of the effect of nicotinic acid alone or in combination on cardiovascular events and atherosclerosis". Atherosclerosis 210 (2): 353–361. doi:10.1016/j.atherosclerosis.2009.12.023. PMID 20079494. Retrieved 13 December 2014.
- ↑ Cantarella L, Gallifuoco A, Malandra A, Martínková L, Spera A, Cantarella M (2011). "High-yield continuous production of nicotinic acid via nitrile hydratase-amidase cascade reactions using cascade CSMRs". Enzyme and Microbial Technology 48 (4–5): 345–50. doi:10.1016/j.enzmictec.2010.12.010. PMID 22112948.
- ↑ Cox, Michael; Lehninger, Albert L; Nelson, David R. (2000). Lehninger principles of biochemistry. New York: Worth Publishers. ISBN 1-57259-153-6.
- 1 2 Wan P, Moat S, Anstey A (2011). "Pellagra: A review with emphasis on photosensitivity". The British journal of dermatology 164 (6): 1188–200. doi:10.1111/j.1365-2133.2010.10163.x. PMID 21128910.
- ↑ Ishii N, Nishihara Y (1981). "Pellagra among chronic alcoholics: Clinical and pathological study of 20 necropsy cases". Journal of neurology, neurosurgery, and psychiatry 44 (3): 209–15. doi:10.1136/jnnp.44.3.209. PMC 490893. PMID 7229643.
- ↑ Jaconello P (October 1992). "Niacin versus niacinamide". CMAJ 147 (7): 990. PMC 1336277. PMID 1393911.
- ↑ Jacobson, EL (2007). "Niacin". Linus Pauling Institute. Retrieved 8 August 2011.
- ↑ Institute of Medicine (2006). Dietary Reference Intakes Research Synthesis: Workshop Summary. National Academies Press. p. 37.
- ↑ Jacob RA, Swendseid ME, McKee RW, Fu CS, Clemens RA (April 1989). "Biochemical markers for assessment of niacin status in young men: urinary and blood levels of niacin metabolites". J. Nutr. 119 (4): 591–8. PMID 2522982.
- ↑ Pitsavas S, Andreou C, Bascialla F, Bozikas VP, Karavatos A (2004). "Pellagra encephalopathy following B-complex vitamin treatment without niacin". Int J Psychiatry Med 34 (1): 91–5. doi:10.2190/29XV-1GG1-U17K-RGJH. PMID 15242145.
- 1 2 3 4 Prakash R, Gandotra S, Singh LK, Das B, Lakra A (2008). "Rapid resolution of delusional parasitosis in pellagra with niacin augmentation therapy". General Hospital Psychiatry 30 (6): 581–4. doi:10.1016/j.genhosppsych.2008.04.011. PMID 19061687.
- ↑ Niacin tablet label Updated March 14, 2013. Page accessed Feb 11, 2016
- ↑ Bruckert E, Labreuche J, Amarenco P (2010). "Meta-analysis of the effect of nicotinic acid alone or in combination on cardiovascular events and atherosclerosis". Atherosclerosis 210 (2): 353–61. doi:10.1016/j.atherosclerosis.2009.12.023. PMID 20079494.
- ↑ Duggal JK, Singh M, Attri N, Singh PP, Ahmed N, Pahwa S, Molnar J, Singh S, Khosla S, Arora R (2010). "Effect of niacin therapy on cardiovascular outcomes in patients with coronary artery disease". Journal of cardiovascular pharmacology and therapeutics 15 (2): 158–66. doi:10.1177/1074248410361337. PMID 20208032.
- ↑ NCEP (2002). "Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report". Circulation 106 (25): 3143–3421.
- 1 2 Sinthupoom, Nujarin; Prachayasittikul, Veda; Prachayasittikul, Supaluk; Ruchirawat, Somsak; Prachayasittikul, Virapong. "Nicotinic acid and derivatives as multifunctional pharmacophores for medical applications". Eur Food Res Technol 240 (1): 1–17. doi:10.1007/s00217-014-2354-1.
- 1 2 3 Kos Pharmaceuticals Inc. Niaspan® (niacin extended-release) tablets prescribing information. Cranbury, NJ; 2005 Oct.
- 1 2 Bays HE, Rader DJ (2009). "Does nicotinic acid (niacin) lower blood pressure?". Int. J. Clin. Pract. 63 (1): 151–9. doi:10.1111/j.1742-1241.2008.01934.x. PMC 2705821. PMID 19054161.
- ↑ "Guidelines for Niacin Therapy For the Treatment of Elevated Lipoprotein a (Lpa)" (PDF). Rush Hemophilia & Thrombophilia Center. 27 July 2005 [15 August 2002]. Retrieved 20 November 2009.
facial flushing is a common side effect of niacin therapy that usually subsides after several weeks of consistent niacin use
- ↑ Kamanna VS, Kashyap ML (2008). "Mechanism of action of niacin". The American journal of cardiology 101 (8A): 20B–26B. doi:10.1016/j.amjcard.2008.02.029. PMID 18375237.
- ↑ Katzung, Bertram G. (2006). Basic and clinical pharmacology. New York: McGraw-Hill Medical Publishing Division. ISBN 0-07-145153-6.
- ↑ Barter, P (2006). "Options for therapeutic intervention: How effective are the different agents?". European Heart Journal Supplements 8 (F): F47–F53. doi:10.1093/eurheartj/sul041.
- ↑ Chapman MJ, Assmann G, Fruchart JC, Shepherd J, Sirtori C (2004). "Raising high-density lipoprotein cholesterol with reduction of cardiovascular risk: the role of nicotinic acid—a position paper developed by the European Consensus Panel on HDL-C". Curr Med Res Opin 20 (8): 1253–68. doi:10.1185/030079904125004402. PMID 15324528.
- 1 2 3 4 Brunton, Laurence L.; Lazo, John S.; Parker, Keith, eds. (2005). Goodman & Gilman's The Pharmacological Basis of Therapeutics (11th ed.). New York: McGraw-Hill. ISBN 0-07-142280-3.
- 1 2 Papaliodis D, Boucher W, Kempuraj D, Michaelian M, Wolfberg A, House M, Theoharides TC (December 2008). "Niacin-induced "Flush" Involves Release of Prostaglandin D2 from Mast Cells and Serotonin from Platelets: Evidence from Human Cells in Vitro and an Animal Model". J Pharmacol Exp Ther 327 (3): 665–72. doi:10.1124/jpet.108.141333. PMID 18784348.
- ↑ Benyó Z, Gille A, Kero J, Csiky M, Suchánková MC, Nüsing RM, Moers A, Pfeffer K, Offermanns S (2005). "GPR109A (PUMA-G/HM74A) mediates nicotinic acid-induced flushing". The Journal of Clinical Investigation 115 (12): 3634–40. doi:10.1172/JCI23626. PMC 1297235. PMID 16322797.
- ↑ Benyó Z, Gille A, Bennett CL, Clausen BE, Offermanns S (2006). "Nicotinic acid-induced flushing is mediated by activation of epidermal langerhans cells". Molecular Pharmacology 70 (6): 1844–9. doi:10.1124/mol.106.030833. PMID 17008386.
- ↑ Hanson J, Gille A, Zwykiel S, Lukasova M, Clausen BE, Ahmed K, Tunaru S, Wirth A, Offermanns S (2010). "Nicotinic acid- and monomethyl fumarate-induced flushing involves GPR109A expressed by keratinocytes and COX-2-dependent prostanoid formation in mice". The Journal of Clinical Investigation 120 (8): 2910–9. doi:10.1172/JCI42273. PMC 2912194. PMID 20664170.
- ↑ Maciejewski-Lenoir D, Richman JG, Hakak Y, Gaidarov I, Behan DP, Connolly DT (2006). "Langerhans cells release prostaglandin D2 in response to nicotinic acid". The Journal of investigative dermatology 126 (12): 2637–46. doi:10.1038/sj.jid.5700586. PMID 17008871.
- 1 2 Gille A, Bodor ET, Ahmed K, Offermanns S (2008). "Nicotinic acid: Pharmacological effects and mechanisms of action". Annual review of pharmacology and toxicology 48 (1): 79–106. doi:10.1146/annurev.pharmtox.48.113006.094746. PMID 17705685.
- ↑ Rader JI, Calvert RJ, Hathcock JN (January 1992). "Hepatic toxicity of unmodified and time-release preparations of niacin". The American Journal of Medicine 92 (1): 77–81. doi:10.1016/0002-9343(92)90018-7. PMID 1731514.
- ↑ Capuzzi DM, Morgan JM, Brusco OA, Intenzo CM (2000). "Niacin dosing: relationship to benefits and adverse effects". Curr Atheroscler Rep 2 (1): 64–71. doi:10.1007/s11883-000-0096-y. PMID 11122726.
- ↑ Mittal MK, Florin T, Perrone J, Delgado JH, Osterhoudt KC (2007). "Toxicity from the use of niacin to beat urine drug screening". Ann Emerg Med 50 (5): 587–90. doi:10.1016/j.annemergmed.2007.01.014. PMID 17418450.
- ↑ Gass JD (2003). "Nicotinic acid maculopathy". Retina (Philadelphia, Pa.) 23 (6 Suppl): 500–10. PMID 15035390.
- ↑ Soga T, Kamohara M, Takasaki J, Matsumoto S, Saito T, Ohishi T, Hiyama H, Matsuo A, Matsushime H, Furuichi K (2003). "Molecular identification of nicotinic acid receptor". Biochemical and Biophysical Research Communications 303 (1): 364–9. doi:10.1016/S0006-291X(03)00342-5. PMID 12646212.
- ↑ Wise A, Foord SM, Fraser NJ, Barnes AA, Elshourbagy N, Eilert M, Ignar DM, Murdock PR, Steplewski K, Green A, Brown AJ, Dowell SJ, Szekeres PG, Hassall DG, Marshall FH, Wilson S, Pike NB (2003). "Molecular identification of high and low affinity receptors for nicotinic acid". The Journal of Biological Chemistry 278 (11): 9869–74. doi:10.1074/jbc.M210695200. PMID 12522134.
- ↑ Wanders D, Judd RL (2011). "Future of GPR109A agonists in the treatment of dyslipidaemia". Diabetes, obesity & metabolism 13 (8): 685–91. doi:10.1111/j.1463-1326.2011.01400.x. PMID 21418500.
- ↑ Hernandez C, Molusky M, Li Y, Li S, Lin JD (2010). "Regulation of hepatic ApoC3 expression by PGC-1β mediates hypolipidemic effect of nicotinic acid". Cell metabolism 12 (4): 411–9. doi:10.1016/j.cmet.2010.09.001. PMC 2950832. PMID 20889132.
- 1 2 3 Villines TC, Kim AS, Gore RS, Taylor AJ (2012). "Niacin: The evidence, clinical use, and future directions". Current atherosclerosis reports 14 (1): 49–59. doi:10.1007/s11883-011-0212-1. PMID 22037771.
- ↑ Rubic T, Trottmann M, Lorenz RL (2004). "Stimulation of CD36 and the key effector of reverse cholesterol transport ATP-binding cassette A1 in monocytoid cells by niacin". Biochemical pharmacology 67 (3): 411–9. doi:10.1016/j.bcp.2003.09.014. PMID 15037193.
- ↑ Barter P, Gotto AM, LaRosa JC, Maroni J, Szarek M, Grundy SM, Kastelein JJ, Bittner V, Fruchart JC (2007). "HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular events". The New England Journal of Medicine 357 (13): 1301–10. doi:10.1056/NEJMoa064278. PMID 17898099.
- ↑ Jafri H, Alsheikh-Ali AA, Karas RH (2010). "Meta-analysis: Statin therapy does not alter the association between low levels of high-density lipoprotein cholesterol and increased cardiovascular risk". Annals of internal medicine 153 (12): 800–8. doi:10.1059/0003-4819-153-12-201012210-00006. PMID 21173414.
- ↑ Wu BJ, Yan L, Charlton F, Witting P, Barter PJ, Rye KA (2010). "Evidence that niacin inhibits acute vascular inflammation and improves endothelial dysfunction independent of changes in plasma lipids". Arteriosclerosis, thrombosis, and vascular biology 30 (5): 968–75. doi:10.1161/ATVBAHA.109.201129. PMID 20167660.
- ↑ Gustafson B (2010). "Adipose tissue, inflammation and atherosclerosis". Journal of atherosclerosis and thrombosis 17 (4): 332–41. doi:10.5551/jat.3939. PMID 20124732.
- ↑ Fu L, Doreswamy V, Prakash R (2014). "The biochemical pathways of central nervous system neural degeneration in niacin deficiency". Neural Regen Res 9 (16): 1509–1513. doi:10.4103/1673-5374.139475. PMC 4192966. PMID 25317166.
Recent evidences suggest that niacin administration may up-regulate the expression of BDNF-TrkB. ... At present, we can safely raise the possibility that niacin-mediated neural growth by the BDNF-TrkB pathway could be at least partially mediated by enhanced HDL-C levels.
- ↑ Creider, JC; Hegele, RA; Joy, TR (September 2012). "Niacin: another look at an underutilized lipid-lowering medication.". Nature reviews. Endocrinology 8 (9): 517–28. doi:10.1038/nrendo.2012.22. PMID 22349076.
- ↑ Jacobson, EL (2007). "Niacin". Linus Pauling Institute. Retrieved 31 March 2008.
- ↑ Endur-Acin Oral : Uses, Side Effects, Interactions, Pictures, Warnings & Dosing – WebMD
- ↑ L-arginine, niacin, phytosterols, pantethine, calcium, vitamin c, b complex, cholesterol control without diet, 8 week cholesterol cure, linus pauling
- ↑ http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.SearchAction&SearchType=BasicSearch&SearchTerm=NIACIN
- ↑ Study Finds Extended Release Niacin, but not IHN, Effective in Lowering Cholesterol Levels
- ↑ Norris RB (2006). ""Flush-free niacin": Dietary supplement may be "benefit-free"". Preventive cardiology 9 (1): 64–5. doi:10.1111/j.1520-037X.2006.04736.x. PMID 16407706.
- ↑ "A case for immediate-release niacin". Heart Lung 41: 95–8. 2012. doi:10.1016/j.hrtlng.2010.07.019. PMID 21414665.
- ↑ Pharmacokinetics and dose recommendations of Niaspan® in chronic kidney disease and dialysis patients
- ↑ Niaspan (Niacin) Drug Information: Description, User Reviews, Drug Side Effects, Interactions – Prescribing Information at RxList
- ↑ About NIASPAN® (niacin extended-release)
- ↑ Lai E, De Lepeleire I, Crumley TM, Liu F, Wenning LA, Michiels N, Vets E, O'Neill G, Wagner JA, Gottesdiener K (2007). "Suppression of niacin-induced vasodilation with an antagonist to prostaglandin D2 receptor subtype 1". Clinical pharmacology and therapeutics 81 (6): 849–57. doi:10.1038/sj.clpt.6100180. PMID 17392721.
- ↑ Paolini JF, Bays HE, Ballantyne CM, Davidson M, Pasternak R, Maccubbin D, Norquist JM, Lai E, Waters MG, Kuznetsova O, Sisk CM, Mitchel YB (November 2008). "Extended-release niacin/laropiprant: reducing niacin-induced flushing to better realize the benefit of niacin in improving cardiovascular risk factors". Cardiol Clin 26 (4): 547–60. doi:10.1016/j.ccl.2008.06.007. PMID 19031552.
- ↑ Kamanna VS, Vo A, Kashyap ML (2008). "Nicotinic acid: Recent developments". Current Opinion in Cardiology 23 (4): 393–8. doi:10.1097/HCO.0b013e3283021c82. PMID 18520725..
- ↑ Treatment of HDL to Reduce the Incidence of Vascular Events HPS2-THRIVE – Full Text View – ClinicalTrials.gov
- ↑ Medscape: Medscape Access
- ↑ "Merck begins overseas recall of HDL cholesterol drug". Reuters. 11 January 2013.
- ↑ Taheri, R (15 January 2003). "No-Flush Niacin for the Treatment of Hyperlipidemia". Medscape. Retrieved 31 March 2008.
- ↑ Kruse W, Kruse W, Raetzer H, Heuck CC, Oster P, Schellenberg B, Schlierf G (1979). "Nocturnal inhibition of lipolysis in man by nicotinic acid and derivatives". European Journal of Clinical Pharmacology 16 (1): 11–15. doi:10.1007/BF00644960. PMID 499296.
- ↑ Meyers CD, Carr MC, Park S, Brunzell JD (2003). "Varying cost and free nicotinic acid content in over-the-counter niacin preparations for dyslipidemia" (PDF). Annals of Internal Medicine 139 (12): 996–1002. doi:10.7326/0003-4819-139-12-200312160-00009. PMID 14678919.
- ↑ Benjó AM, Maranhão RC, Coimbra SR, Andrade AC, Favarato D, Molina MS, Brandizzi LI, da Luz PL (2006). "Accumulation of chylomicron remnants and impaired vascular reactivity occur in subjects with isolated low HDL cholesterol: effects of niacin treatment". Atherosclerosis 187 (1): 116–122. doi:10.1016/j.atherosclerosis.2005.08.025. PMID 16458316.
- ↑ F. Aguilar, U.R. Charrondiere, B. Dusemund, P. Galtier, J. Gilbert, D.M. Gott, S. Grilli, R. Guertler, G.E.N. Kass, J. Koenig, C. Lambré, J-C. Larsen, J-C. Leblanc, A. Mortensen, D. Parent-Massin, I. Pratt, I.M.C.M. Rietjens, I. Stankovic, P. Tobback, T. Verguieva, R.A. Woutersen (2009). "Inositol hexanicotinate (inositol hexaniacinate) as a source of niacin (vitamin B3) added for nutritional purposes in food supplements" (PDF). The EFSA Journal 949: 1–20.
- ↑ Knip M, Douek IF, Moore WP, Gillmor HA, McLean AE, Bingley PJ, Gale EA (2000). "Safety of high-dose nicotinamide: a review". Diabetologia 43 (11): 1337–45. doi:10.1007/s001250051536. PMID 11126400.
- ↑ Diet & Fitness today. "Niacin in beer".
- ↑ "Vegemite – Nutritional information". Retrieved 6 November 2013.
- ↑ "Marmite – Nutritional information". Retrieved 19 November 2014.
- ↑ Weidel, H (1873). "Zur Kenntniss des Nicotins". Justus Liebigs Annalen der Chemie und Pharmacie 165 (2): 330–349. doi:10.1002/jlac.18731650212.
- ↑ Samuel M. McElvain (1941). "Nicotinic Acid" (PDF). Org. Synth.; Coll. Vol. 1, p. 385
- ↑ Elvehjem CA, Madden RJ, Strongandd FM, Woolley DW (1938). "The isolation and identification of the anti-blacktongue factor J" (PDF). J. Biol. Chem. 123 (1): 137–149.
- ↑ Dr. Joseph Goldberger and the war on Pellagra – Office of NIH History
- 1 2 "Pellagra And Its Prevention And Control In Major Emergencies" (PDF). World Health Organization. World Health Organization. Retrieved 17 April 2015.
- ↑ Laguna J, Carpenter KJ (September 1951). "Raw versus processed corn in niacin-deficient diets". J. Nutr. 45 (1): 21–8. PMID 14880960.
- ↑ Altschul R, Hoffer A, Stephen JD (1955). "Influence of nicotinic acid on serum cholesterol in man". Archives of biochemistry and biophysics 54 (2): 558–9. doi:10.1016/0003-9861(55)90070-9. PMID 14350806.
- ↑ Vitamins B3 found in Meteorites http://canadajournal.net/science/vitamins-b3-found-meteorites-study-6534-2014/
External links
| ||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||