Non-alcoholic fatty liver disease
| Non-alcoholic fatty liver disease | |
|---|---|
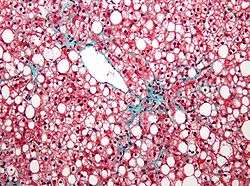 Micrograph of non-alcoholic fatty liver disease, demonstrating marked steatosis (fatty liver appears white). Trichrome stain | |
| Classification and external resources | |
| Specialty | Gastroenterology |
| ICD-10 | K76.0 |
| ICD-9-CM | 571.8 |
| DiseasesDB | 29786 |
| eMedicine | med/775 |
Non-alcoholic fatty liver disease (NAFLD) is one of the causes of fatty liver, occurring when fat is deposited (steatosis) in the liver due to causes other than excessive alcohol use. NAFLD is the most common liver disorder in developed countries.[1][2] A recent study using the National Health and Nutrition Examination Survey (NHANES) found a 30% prevalence of NAFLD in the United States between 2011 and 2012.[3]
NAFLD is related to insulin resistance and the metabolic syndrome and may respond to treatments originally developed for other insulin-resistant states (e.g. diabetes mellitus type 2) such as weight loss, metformin, and thiazolidinediones.[4] Up to 80% of obese people have the disease.[5] Non-alcoholic steatohepatitis (NASH) is the most extreme form of NAFLD, and is regarded as a major cause of cirrhosis of the liver of unknown cause.[6] Most people have a good outcome if the condition is caught in its early stages.[7]
Signs and symptoms
Most people with NAFLD have few or no symptoms. Patients may complain of fatigue, malaise, and dull right-upper-quadrant abdominal discomfort. Mild jaundice may be noticed although this is rare. More commonly NAFLD is diagnosed following abnormal liver function tests during routine blood tests. By definition, alcohol consumption of over 20 g/day (about 25 ml/day of net ethanol) excludes the condition.[4]
NAFLD is associated with insulin resistance and metabolic syndrome (obesity, combined hyperlipidemia, diabetes mellitus (type II), and high blood pressure).[4][6]
Causes
NAFLD can also be caused by some medications:[4]
- Amiodarone
- Antiviral drugs (nucleoside analogues)
- Aspirin rarely as part of Reye's syndrome in children
- Corticosteroids
- Methotrexate
- Tamoxifen
- Tetracycline
Soft drinks
Soft drinks have been linked to NAFLD due to high concentrations of fructose, which may be present either in high-fructose corn syrup or, in similar quantities, as a metabolite of sucrose. The quantity of fructose delivered by soft drinks may cause increased deposition of fat in the abdomen.[8][9]
Genetics
Native American men have a high prevalence of non-alcoholic fatty liver disease. Two genetic mutations for this susceptibility have been identified, and these mutations provided clues to the mechanism of NASH and related diseases.
Polymorphisms (genetic variations) in the single-nucleotide polymorphisms (SNPs) T455C and C482T in APOC3 are associated with fatty liver disease, insulin resistance, and possibly hypertriglyceridemia. 95 healthy Asian Indian men and 163 healthy non-Asian Indian men around New Haven, Connecticut were genotyped for polymorphisms in those SNPs. 20% homogeneous wild both loci. Carriers of T-455C, C-482T, or both (not additive) had a 30% increase in fasting plasma apolipoprotein C3, 60% increase in fasting plasma triglyceride and retinal fatty acid ester, and 46% reduction in plasma triglyceride clearance. Prevalence of non-alcoholic fatty liver disease was 38% in carriers, 0% wild (normal). Subjects with fatty liver disease had marked insulin resistance.[10]
Pathophysiology
NAFLD is considered to cover a spectrum of disease activity. This spectrum begins as fatty accumulation in the liver (hepatic steatosis). A liver can remain fatty without disturbing liver function, but by varying mechanisms and possible insults to the liver may also progress to become non-alcoholic steatohepatitis (NASH), a state in which steatosis is combined with inflammation and fibrosis (steatohepatitis). NASH is a progressive disease: over a 10-year period, up to 20% of patients with NASH will develop cirrhosis of the liver, and 10% will suffer death related to liver disease.[11] Cigarette smoking is not associated with an increased risk of developing NASH.
The exact cause of NAFLD is still unknown. However, both obesity and insulin resistance probably play a strong role in the disease process. The exact reasons and mechanisms by which the disease progresses from one stage to the next are not known.
One debated mechanism proposes a "second hit", or further injury, enough to cause change that leads from hepatic steatosis to hepatic inflammation. Oxidative stress, hormonal imbalances, and mitochondrial abnormalities are potential causes for this "second hit" phenomenon.[4]
Diagnosis
Common findings are elevated liver enzymes and a liver ultrasound showing steatosis. An ultrasound may also be used to exclude gallstone problems (cholelithiasis). A liver biopsy (tissue examination) is the only test widely accepted as definitively distinguishing NASH from other forms of liver disease and can be used to assess the severity of the inflammation and resultant fibrosis.[4]
Non-invasive diagnostic tests have been developed, such as FibroTest, that estimates liver fibrosis,[12] and SteatoTest, that estimates steatosis,[13] however their use has not been widely adopted.[14] Apoptosis has been indicated as a potential mechanism of hepatocyte injury as caspase-cleaved cytokeratin 18 (M30-Apoptosense ELISA) in serum/plasma is often elevated in patients with NASH; however, as the role of oncotic necrosis has yet to be examined it is unknown to what degree apoptosis acts as the predominant form of injury.[15][16]
Other diagnostic tests are available. Relevant blood tests include erythrocyte sedimentation rate, glucose, albumin, and kidney function. Because the liver is important for making proteins used in coagulation some coagulation related studies are often carried out especially the INR (international normalized ratio). Blood tests (serology) are usually used to rule out viral hepatitis (hepatitis A, B, C and herpes viruses like EBV or CMV), rubella, and autoimmune related diseases. Hypothyroidism is more prevalent in NASH patients which would be detected by determining the TSH.[17]
It has been suggested that in cases involving overweight patients whose blood tests do not improve on losing weight and exercising that a further search of other underlying causes be undertaken. This would also apply to those with fatty liver who are very young or not overweight or insulin-resistant. In addition those whose physical appearance indicates the possibility of a congenital syndrome, have a family history of liver disease, have abnormalities in other organs, and those that present with moderate to advanced fibrosis or cirrhosis.[18]
Management
No pharmacological treatment has received approval as of 2015.[19] Some studies suggest diet, exercise, and antiglycemic drugs may alter the course of the disease. General recommendations include improving metabolic risk factors and reducing alcohol intake.[4][20] While many treatments appear to improve biochemical markers such as alanine transaminase levels, most have not been shown to reverse histological abnormalities or reduce clinical endpoints.[4]
Nutrition
Treatment of NAFLD typically involves counseling to improve nutrition and consequently body weight and composition. Diet changes have shown significant histological improvement.[21] Specifically, avoiding food containing high-fructose corn syrup and trans-fats is recommended.[22] A systematic review and meta-analysis found that omega-3 fatty acid supplementation in those with NAFLD/NASH using doses approaching or higher than 1 gram daily (median dose 4 grams/day with median duration 6 months treatment) has been associated with improvements in liver fat.[23][24] The best dose of omega-3 fatty acids for individuals with NAFLD/NASH is unclear.[23]
Epidemiological data have suggested that coffee consumption may be associated with a decreased incidence of NAFLD and may reduce the risk of liver fibrosis in those who already have NAFLD/NASH.[23] Olive oil consumption, as part of the Mediterranean diet, is also a reasonable dietary intervention; the optimal dose of olive oil supplementation for people with NAFLD/NASH has not been well-established.[23] Few studies have been performed to evaluate the respective impact of a diet rich in avocados, red wine, tree nuts, or tea in people with NAFLD/NASH.[23] However, limited evidence suggests that avocados may improve other areas of cardiovascular health (i.e., lipid profile) and their addition to a balanced diet is reasonable.[23] Red wine consumption (in modest amounts) is likely safe and may improve insulin resistance but definitive studies are lacking.[23]
Exercise
Gradual weight loss may improve the process in obese patients; rapid loss may worsen NAFLD. Specifically, walking or some form of aerobic exercise at least 30–45 minutes daily is recommended.[22] The negative effects of rapid weight loss are controversial: the results of a meta-analysis showed that the risk of progression is very low.[25]
Medication
Insulin sensitizers (metformin and thiazolidinediones) are commonly used to combat insulin resistance in those with NAFLD.[26] Improvements in liver biochemistry and histology in patients with NAFLD through treatment with statins have been observed in numerous cases, although these studies were carried out on a relatively small sample of patients.[27] Statins have also been recommended for use in treating dyslipidemia for patients with NAFLD. Treatment with pentoxifylline has demonstrated improvements in the histological appearance of fatty liver tissue under the microscope in many small trials.[26]
Surgery
A recent meta-analysis presented at the Annual Meeting of the American Association for the Study of Liver Diseases (AASLD) reported that weight-loss surgery leads to improvement and or resolution of NASH in around 80% of patients.[28]
Epidemiology
The percentage of people with non-alcoholic fatty liver disease ranges from 9 to 36.9% in different parts of the world.[29][30][31] Approximately 20% of the United States population have non-alcoholic fatty liver, and the number of people affected is increasing.[32] This means about 75 to 100 million people in the United States are affected.[33]
The rates of non-alcoholic fatty liver disease is higher in Hispanics, which can be attributed to high rates of obesity and type 2 diabetes in Hispanic populations.[34] Non-alcoholic fatty liver disease is also more common among men than women in all age groups until age 60, where the prevalence between sex equalize. This is due to the protective nature of estrogen.[35] Fatty liver and NASH occur all ages, with the highest rates in the 40- to 49-year-old age group. It is the most common liver abnormality in children ages 2 to 19.[36]
Children
Pediatric nonalcoholic fatty liver disease (NAFLD) was first reported in 1983.[37] It is currently the primary form of liver disease among children.[38] NAFLD has been associated with the metabolic syndrome, which is a cluster of risk factors that contribute to the development of cardiovascular disease and type 2 diabetes mellitus. Studies have demonstrated that abdominal obesity and insulin-resistance in particular are thought to be key contributors to the development of NAFLD.[39][40][41][42][43] Because obesity is becoming an increasingly common problem worldwide, the prevalence of NAFLD has been increasing concurrently.[44] Moreover, boys are more likely to be diagnosed with NAFLD than girls with a ratio of 2:1.[45][46] Studies have suggested that progression toward a more advance stage of disease among children is dependent on age and presence of obesity.[41] This finding is consistent with previous studies in adults demonstrating the same association between age and obesity, and liver fibrosis.[47][48] Early diagnosis of NAFLD in children may help prevent the development of liver disease during adulthood.[41][49] This is challenging as most children with NAFLD are asymptomatic with few showing abdominal pain.[49] Currently, liver biopsy is considered the gold standard for diagnosing NAFLD.[38] However, this method is invasive, costly and bears greater risk for children, and noninvasive screening and diagnosing methods would have significant public health implications for children with NAFLD.[38] The only treatment shown to be truly effective in childhood NAFLD is weight loss.[50][51]
See also
- Fatty liver (includes both non-alcoholic and alcoholic liver disease)
- Alcoholic liver disease
References
- ↑ Shaker, Mina, et al. "Liver transplantation for nonalcoholic fatty liver disease: New challenges and new opportunities." World journal of gastroenterology: WJG 20.18 (2014): 5320.
- ↑ Rinella ME (June 2015). "Nonalcoholic fatty liver disease: a systematic review". JAMA (Systematic review) 313 (22): 2263–73. doi:10.1001/jama.2015.5370. PMID 26057287.
- ↑ Ruhl, C. E., and J. E. Everhart. "Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey." Alimentary pharmacology & therapeutics 41.1 (2015): 65-76.
- 1 2 3 4 5 6 7 8 Adams LA, Angulo P (2006). "Treatment of non‐alcoholic fatty liver disease". Postgrad Med J 82 (967): 315–22. doi:10.1136/pgmj.2005.042200. PMC 2563793. PMID 16679470.
- ↑ Sanyal, A J (2002). "AGA Technical Review on Nonalcoholic Fatty Liver Disease.". Bethesda, MD: American Gastroenterological Association.
- 1 2 Clark JM, Diehl AM (2003). "Nonalcoholic fatty liver disease: an underrecognized cause of cryptogenic cirrhosis". JAMA 289 (22): 3000–4. doi:10.1001/jama.289.22.3000. PMID 12799409.
- ↑ "Nonalcoholic Fatty Liver Disease".
- ↑ Nseir, W.; Nassar, F.; Assy, N. (2010). "Soft drinks consumption and nonalcoholic fatty liver disease". World Journal of Gastroenterology 16 (21): 2579–2588. doi:10.3748/wjg.v16.i21.2579. PMC 2880768. PMID 20518077.
- ↑ Allocca, M; Selmi C (2010). "Emerging nutritional treatments for nonalcoholic fatty liver disease". In Preedy VR; Lakshman R; Rajaskanthan RS. Nutrition, diet therapy, and the liver. CRC Press. pp. 131–146. ISBN 1420085492.
- ↑ Petersen KF, Dufour S, Hariri A, et al. (2010). "Apolipoprotein C3 Gene Variants in Nonalcoholic Fatty Liver Disease". N. Engl. J. Med. 362 (12): 1082–9. doi:10.1056/NEJMoa0907295. PMC 2976042. PMID 20335584.
- ↑ McCulough, Arthur J (Aug 2004). "The clinical features, diagnosis and natural history of nonalcoholic fatty liver disease". Clinics in Liver Disease 8 (3): 521–33. doi:10.1016/j.cld.2004.04.004. PMID 15331061.
- ↑ Halfon P, Munteanu M, Poynard T (2008). "FibroTest-ActiTest as a non-invasive marker of liver fibrosis". Gastroenterol Clin Biol 32 (6): 22–39. doi:10.1016/S0399-8320(08)73991-5. PMID 18973844.
- ↑ Ratziu; Massard, J; Charlotte, F; Messous, D; Imbert-Bismut, F; Bonyhay, L; Tahiri, M; Munteanu, M; Thabut, D; Cadranel, Jean; Le Bail, Brigitte; De Ledinghen, Victor; Poynard, Thierry; et al. (2006). "Diagnostic value of biochemical markers (FibroTest-FibroSURE) for the prediction of liver fibrosis in patients with non-alcoholic fatty liver disease". BMC Gastroenterology 6: 6. doi:10.1186/1471-230X-6-6. PMC 1386692. PMID 16503961.
- ↑ Vuppalanchi R, Chalasani N (2009). "Non-alcoholic fatty liver disease and non-alcoholic steatohepatitis: Selected practical issues in their evaluation and management". Hepatology 49 (1): 306–317. doi:10.1002/hep.22603. PMC 2766096. PMID 19065650.
- ↑ Feldstein AE; Wieckowska, Anna; Lopez, A. Rocio; Liu, Yao-Chang; Zein, Nizar N.; McCullough, Arthur J.; et al. (2009). "Cytokeratin-18 fragment levels as noninvasive biomarker for nonalcoholic steatohepatitis: A multicenter validation study". Hepatology 50 (4): 1072–8. doi:10.1002/hep.23050. PMC 2757511. PMID 19585618.
- ↑ Musso G; Gambino, Roberto; Cassader, Maurizio; Pagano, Gianfranco; et al. (2010). "Meta-analysis: Natural history of non-alcoholic fatty liver disease (NAFLD) and diagnostic accuracy of non-invasive tests for liver disease severity". Annals of Medicine 43 (8): 1–33. doi:10.3109/07853890.2010.518623. PMID 21039302.
- ↑ Liangpunsakul S, Chalasani N (2003). "Is hypothyroidism a risk factor for non-alcoholic steatohepatitis?". J Clin Gastroenterol 37 (4): 340–3. doi:10.1097/00004836-200310000-00014. PMID 14506393.
- ↑ Cassiman D, Jaeken J (2008). "NASH may be trash". Gut 57 (2): 141–4. doi:10.1136/gut.2007.123240. PMID 18192446.
- ↑ Ratziu, V; Goodman, Z; Sanyal, A (April 2015). "Current efforts and trends in the treatment of NASH.". Journal of Hepatology 62 (1 Suppl): S65–75. doi:10.1016/j.jhep.2015.02.041. PMID 25920092.
- ↑ Veena J, Muragundla A, Sidgiddi S, Subramaniam S (2014). "Non-alcoholic fatty liver disease: need for a balanced nutritional source". Br. J. Nutr. 112 (11): 1858–72. doi:10.1017/S0007114514002591. PMID 25274101.
- ↑ Huang MA, Greenson JK, Chao C, et al. (2005). "One-year intense nutritional counseling results in histological improvement in patients with non-alcoholic steatohepatitis: a pilot study". Am. J. Gastroenterol. 100 (5): 1072–81. doi:10.1111/j.1572-0241.2005.41334.x. PMID 15842581.
- 1 2 Ashutosh S. Naniwadekar. "Nutritional Recommendations for Patients with Non-Alcoholic Fatty Liver Disease: An Evidence Based Review". NUTRITION ISSUES IN GASTROENTEROLOGY, SERIES. www.practicalgastro.com. Archived from the original (PDF) on 29 August 2012. Retrieved 29 August 2012.
- 1 2 3 4 5 6 7 Gupta V, Mah XJ, Garcia MC, Antonypillai C, van der Poorten D (October 2015). "Oily fish, coffee and walnuts: Dietary treatment for nonalcoholic fatty liver disease". World J Gastroenterol (Review) 21 (37): 10621–35. doi:10.3748/wjg.v21.i37.10621. PMC 4588084. PMID 26457022.
- ↑ Parker HM, Johnson NA, Burdon CA, Cohn JS, O'Connor HT, George J (April 2012). "Omega-3 supplementation and non-alcoholic fatty liver disease: a systematic review and meta-analysis". J Hepatol (Systematic review and meta-analysis) 56 (4): 944–51. doi:10.1016/j.jhep.2011.08.018. PMID 22023985.
- ↑ Nila Rafiq; Zobair M. Younossi. "Effects of Weight Loss on Nonalcoholic Fatty Liver Disease". SEMINARS IN LIVER DISEASE/VOLUME 28, NUMBER 4 2008. The Permanente Medical Group, Inc. Archived from the original (PDF) on 29 August 2012. Retrieved 29 August 2012.
- 1 2 Raziel A, Sakran N, Szold A, Goitein D (April 2015). "Current solutions for obesity-related liver disorders: non-alcoholic fatty liver disease and non-alcoholic steatohepatitis" (PDF). Isr Med Assoc J 17 (4): 234–8. PMID 26040050.
- ↑ Chalasani N, Younossi Z, Lavine JE, et al. (2012). "The Diagnosis and Management of Non-alcoholic Fatty Liver Disease: Practice Guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology". Gastroenterology 142 (7): 1592–1609. doi:10.1002/hep.25762. PMID 22488764.
- ↑ Neil Osterweil. "AASLD: After Weight Loss Surgery, Liver Signs Improve". MedPage Today. Retrieved 29 August 2012.
- ↑ Omagari K, Kadokawa Y, Masuda J, Egawa I, Sawa T, Hazama H, et al. (2002). "Fatty liver in non-alcoholic non overweight Japanese adults: incidence and clinical characteristics". J Gastroenterol Hepatol: 1098–1105.
- ↑ Hilden M, Christoffersen P, Juhl E, Dalgaard JB (1977). "Liver histology in a 'normal' population—examinations of 503 consecutive fatal traffi c casualties". Scand J Gastroenterol 12 (5): 593–7. doi:10.3109/00365527709181339. PMID 918553.
- ↑ Shen L, Fan JG, Shao Y, Zeng MD, Wang JR, Luo GH, et al. (2003). "Prevalence of nonalcoholic fatty liver among administrative officers in Shanghai: an epidemiological survey". World J Gastroenterol 9:: 1106–10.
- ↑ Lazo M, Hernaez R, Bonekamp S, Kamel IR, Brancati FL, Guallar E, Clark JM (2011). "Non-alcoholic fatty liver disease and mortality among US adults: prospective cohort study". BMJ 343 (Nov 18): d6891. doi:10.1136/bmj.d6891. PMC 3220620. PMID 22102439.
- ↑ Rinella, ME (9 June 2015). "Nonalcoholic fatty liver disease: a systematic review.". JAMA 313 (22): 2263–73. doi:10.1001/jama.2015.5370. PMID 26057287.
- ↑ Flegal KM, Carroll MD, Ogden CL, Johnson CL (2002). "Prevalence and trends in obesity among US adults, 1999-2000". JAMA 288 (14): 1723–7. doi:10.1001/jama.288.14.1723. PMID 12365955.
- ↑ Lobanova YS, Scherbakov AM, Shatskaya VA, Evteev VA, Krasil’nikov MA (2009). "NF- kappaB suppression provokes the sensitization of hormone-resistant breast cancer cells to estrogen apoptosis". Mol Cell Biochem 324.
- ↑ Pacifico, L; Poggiogalle, E; Cantisani, V; Menichini, G; Ricci, P; Ferraro, F; Chiesa, C (2010). "Pediatric nonalcoholic fatty liver disease: a clinical and laboratory challenge". World J Hepatol (2 ed.) 7: 275–288.
- ↑ Moran JR, Ghishan FK, Halter SA, Greene HI. (1983). "Steatohepatitis in obese children: a cause of chronic liver dysfunction". American Journal of Gastroenterology 78 (6): 374–7. PMID 6859017.
- 1 2 3 Papandreou D, Rousso I, Mavromichalis I (2007). "Update on non-alcoholic fatty liver disease in children". Clinical Nutrition 16: 409–415.
- ↑ Cortez-Pinto H, Camilo ME, Baptista A, et al. (1999). "Nonalcoholic fatty liver: another feature of the metabolic syndrome?". Clinical Nutrition 18 (6): 353–8. doi:10.1016/S0261-5614(99)80015-6.
- ↑ Marchesini G, Brizi M, Bianchi G, et al. (2001). "Nonalcoholic fatty liver disease: a feature of the metabolic syndrome". Diabetes 50 (8): 1844–50. doi:10.2337/diabetes.50.8.1844. PMID 11473047.
- 1 2 3 Nobili V, Marcellini M, Devito R, et al. (2006). "NAFLD in children: A prospective clinical-pathological study and effect of lifestyle advice". Hepatology 44 (2): 458–465. doi:10.1002/hep.21262. PMID 16871574.
- ↑ Pagano G, Pacini G, Musso G, et al. (2002). "Nonalcoholic steatohepatitis, insulin resistance, and metabolic syndrome: further evidence for an etiologic association". Hepatology 362 (35): 367–372. doi:10.1053/jhep.2002.30690.
- ↑ Schwimmer JB, Pardee PE, Lavine JE, et al. (2008). "Cardiovascular risk factors and the metabolic syndrome in pediatric nonalcoholic fatty liver disease". Circulation 118 (12): 277–283. doi:10.1161/CIRCULATIONAHA.107.739920.
- ↑ Barshop NJ; Sirlin, C. B.; Schwimmer, J. B.; Lavine, J. E.; et al. (2008). "Review article: epidemiology, pathogenesis and potential treatments of pediatric non-alcoholic fatty liver disease". Aliment Pharmacol Ther 28 (1): 13–24. doi:10.1111/j.1365-2036.2008.03703.x. PMID 18397387.
- ↑ Baldridge AD, Perez-Atayde AR, Graeme-Cook F, et al. (1995). "Idiopathic steatohepatitis in childhood: a multicenter retrospective study". Journal of Pediatrics. 127 (5): 700–704. doi:10.1016/S0022-3476(95)70156-7. PMID 7472819.
- ↑ Kinugasa A, Tsunamoto K, Furuawa N, et al. (1984). "Fatty liver and its fibrous changes found in simple obesity of children". Journal of Pediatric Gastroenterology Nutrition 3 (12): 408–414. doi:10.1097/00005176-198406000-00018.
- ↑ Angulo P, Keach JC, Batts KP, Lindor KD (1999). "Independent predictors of liver fibrosis in patients with nonalcoholic steatohepatitis". Hepatology 30 (12): 356–362. doi:10.1002/hep.510300604.
- ↑ Ratziu V, Giral P, Charotte F, et al. (2000). "Liver fibrosis in overweight patients". Gastroenterology 118 (6): 1117–1123. doi:10.1016/S0016-5085(00)70364-7. PMID 10833486.
- 1 2 Roberts EA (2007). "Pediatric nonalcoholic fatty liver disease (NAFLD): A "growing" problem?". Journal of Hepatology 46 (6): 1133–42. doi:10.1016/j.jhep.2007.03.003. PMID 17445934.
- ↑ Guha IN, Parkes J, Roderick P, et al. (2008). "Noninvasive markers of fibrosis in nonalcoholic fatty liver disease: validating the European liver fibrosis panel and exploring simple markers". Hepatology 47 (2): 455–460. doi:10.1002/hep.21984. PMID 18038452.
- ↑ Rashid M, Roberts EA (2000). "Nonalcoholic steatohepatitis in children". Journal of Pediatrics Gastroenterology Nutrition 30: 48–53. doi:10.1097/00005176-200001000-00017.
Further reading
- Hassan K, Bhalla V, Ezz El Regal M, A-Kader HH (September 2014). "Nonalcoholic fatty liver disease: A comprehensive review of a growing epidemic". World Journal of Gastroenterology (review) 20 (34): 12082–12101. doi:10.3748/wjg.v20.i34.12082. PMC 4161796. PMID 25232245.
External links
- Medscape article on NASH.
- MEDICINENET article on Steatosis.
- NIH page on Nonalcoholic Steatohepatitis
- British Medical Journal article on the diagnosis and initial management of non-alcoholic fatty liver disease