Musculocutaneous nerve
| Musculocutaneous nerve | |
|---|---|
 Nerves of the left upper extremity. (Musculocutaneous labeled at upper right.) | |
| Details | |
| From | lateral cord (C5-C7) |
| To | lateral cutaneous nerve of forearm |
| Innervates | anterior compartment of the arm |
| Identifiers | |
| Latin | nervus musculocutaneus |
| Dorlands /Elsevier | n_05/12566256 |
| TA | A14.2.03.024 |
| FMA | 37064 |
The musculocutaneous nerve arises from the lateral cord of the brachial plexus, opposite the lower border of the pectoralis major, its fibers being derived from C5, C6 and C7.
Structure
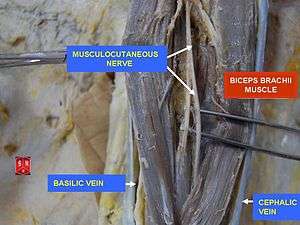
It penetrates the coracobrachialis muscle and passes obliquely between the biceps brachii and the brachialis, to the lateral side of the arm; a little above the elbow it pierces the deep fascia lateral to the tendon of the biceps brachii and is continued into the forearm as the lateral cutaneous nerve of the forearm.
In its course through the arm it innervates the coracobrachialis, biceps brachii, and the greater part of the brachialis.
- The branch to the coracobrachialis is given off from the nerve close to its origin, and in some instances as a separate filament from the lateral cord of the plexus; it is derived from the seventh, cervical nerve.
- The branches to the biceps brachii and brachialis are given off after the musculocutaneous has pierced the coracobrachialis; that supplying the brachialis gives a filament to the elbow-joint.
- The nerve also sends a small branch to the bone, which enters the nutrient foramen with the accompanying artery.
Variations
The musculocutaneous nerve presents frequent variations.
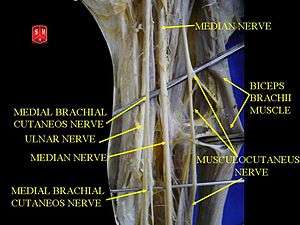
- It may adhere for some distance to the median and then pass outward, beneath the biceps brachii, instead of through the coracobrachialis.
- Some of the fibers of the median may run for some distance in the musculocutaneous and then leave it to join their proper trunk; less frequently the reverse is the case, and the median sends a branch to join the musculocutaneous.[1]
- The nerve may pass under the coracobrachialis or through the biceps brachii.
- Occasionally it gives a filament to the pronator teres, and it supplies the dorsal surface of the thumb when the superficial branch of the radial nerve is absent.
Clinical significance
Although rare, the musculocutaneous nerve can be affected through compression due to hypertrophy or entrapment between the biceps aponeurosis and brachialis fascia or it may be injured through stretch as occurs in dislocations and sometimes in surgery.
Isolated injury causes weakness of elbow flexion and supination of the forearm.
A discrete sensory disturbance is present on the radial side of the forearm. The biceps reflex is also affected.
The nerve is usually involved in an upper brachial plexus palsy.
Injury can occur before entering the coracobrachialis due to dislocation or apparently due to stretch due to throwing injury
Heavy backpacks can cause damage to the upper trunk of the brachial plexus – dysfunction can be severe and prolonged with similar injury as occurs with Erb's palsy from breech deliveries. Early detection is important – the combination of time, avoidance of wearing a backpack, and strengthening of the shoulder muscles will probably be effective.
Distal to the coracobrachialis, the most common cause appears to be weight lifting – either through compression due to hypertrophy or entrapment between the biceps and brachialis, the nerve may lead to a painless loss of muscle strength in flexion and supination of the forearm. Initial treatment should include avoidance of biceps curls or other biceps exercises.
References
This article incorporates text in the public domain from the 20th edition of Gray's Anatomy (1918)
- ↑ Guerri-Guttenberg, Roberto A.; Ingolotti, Mariana (2009). "Classifying musculocutaneous nerve variations". Clinical Anatomy 22 (6): 671. doi:10.1002/ca.20828. PMID 19637305.
External links
- Musculocutaneous_nerve at the Duke University Health System's Orthopedics program
- Hand kinesiology at the University of Kansas Medical Center
| ||||||||||||||||||||||||