Digoxin
 | |
 | |
| Systematic (IUPAC) name | |
|---|---|
|
4-[(3S,5R,8R,9S,10S,12R,13S,14S)-3-[(2S,4S,5R,6R)-5-[(2S,4S,5R,6R)-5-[(2S,4S,5R,6R)-4,5-dihydroxy-6-methyl-oxan-2-yl]oxy-4-hydroxy-6-methyl-oxan-2-yl]oxy-4-hydroxy-6-methyl-oxan-2-yl]oxy-12,14-dihydroxy-10,13-dimethyl-1,2,3,4,5,6,7,8,9,11,12,15,16,17-tetradecahydrocyclopenta[a]phenanthren-17-yl]-5H-furan-2-one | |
| Clinical data | |
| Pronunciation | /dᵻˈdʒɒksᵻn/, with a soft gee[1] |
| Trade names | Lanoxin |
| AHFS/Drugs.com | monograph |
| MedlinePlus | a682301 |
| Pregnancy category | |
| Legal status |
|
| Routes of administration | Oral, Intravenous |
| Pharmacokinetic data | |
| Bioavailability | 60 to 80% (Oral) |
| Protein binding | 25% |
| Metabolism | Hepatic (16%) |
| Biological half-life |
36 to 48 hours (patients with normal renal function) 3.5 to 5 days (patients with impaired renal function) |
| Excretion | Renal |
| Identifiers | |
| CAS Number |
20830-75-5 |
| ATC code | C01AA05 |
| PubChem | CID 2724385 |
| IUPHAR/BPS | 4726 |
| DrugBank |
DB00390 |
| ChemSpider |
2006532 |
| UNII |
73K4184T59 |
| KEGG |
D00298 |
| ChEBI |
CHEBI:4551 |
| ChEMBL |
CHEMBL1751 |
| Chemical data | |
| Formula | C41H64O14 |
| Molar mass | 780.938 g/mol |
| |
| |
| Physical data | |
| Melting point | 249.3 °C (480.7 °F) |
| Solubility in water | 0.0648 mg/mL (20 °C) |
| (verify) | |
Digoxin is a purified cardiac glycoside similar to digitoxin extracted from the foxglove plant, Digitalis lanata.[2] Digoxin is occasionally used in the treatment of various heart conditions, namely atrial fibrillation, atrial flutter and sometimes heart failure that cannot be controlled by other medication.
There are concerns that its general use may increase the risk of death.[3]
Digoxin was discovered by physician William Withering, a graduate of the University of Edinburgh Medical School. It is on the World Health Organization's List of Essential Medicines, a list of the most important medications needed in a basic health system.[4]
Medical use
Irregular heart beat
The most common indications for digoxin are atrial fibrillation and atrial flutter with rapid ventricular response, though beta blockers and/or calcium channel blockers are a better first choice.[5][6] There is tentative evidence that digoxin may increase the risk of death.[3] In just the trials with better methods and lower risk of bias there however is no change in mortality.[7] High ventricular rate leads to insufficient diastolic filling time. By slowing down the conduction in the AV node and increasing its refractory period, digoxin can reduce the ventricular rate. The arrhythmia itself is not affected, but the pumping function of the heart improves, owing to improved filling.
Heart failure
Digoxin is no longer the first choice for heart failure, but can still be useful in people who remain symptomatic despite proper diuretic and ACE inhibitor treatment.
Digoxin has fallen out of favor in people with heart failure because it may increase the risk of death.[3] Because other therapies have shown a mortality benefit in congestive heart failure, maximizing other therapies (e.g., beta blockers) first is recommended before using digoxin.
Other
Digoxin is also used in late term abortions to prevent a live birth. (See: Use during legal abortion.)
Adverse effects
The occurrence of adverse drug reactions is common, owing to its narrow therapeutic index (the margin between effectiveness and toxicity). Adverse effects are concentration-dependent, and are rare when plasma digoxin concentration is <0.8 nanograms/l.[8] They are also more common in patients with low potassium levels (hypokalemia), since digoxin normally competes with K+ ions for the same binding site on the Na+/K+ ATPase pump.
Common adverse effects (≥1% of patients) include loss of appetite, nausea, vomiting, and diarrhea as gastrointestinal motility increases. Other common effects are blurred vision, visual disturbances (yellow-green halos and problems with color perception), confusion, drowsiness, dizziness, insomnia, nightmares, agitation, and depression, as well as a higher acute sense of sensual activities.[9] Less frequent adverse effects (0.1%–1%) include: acute psychosis, delirium, amnesia, convulsions, shortened QRS complex, atrial or ventricular extrasystoles, paroxysmal atrial tachycardia with AV block, ventricular tachycardia or fibrillation, and heart block.[8] Rarely, digoxin has been shown to cause thrombocytopenia. Gynaecomastia (enlargement of breast tissue) is mentioned in many textbooks as a side effect, thought to be due to the estrogen-like steroid moiety of the digoxin molecule,[10] but when systematically sought, the evidence for this is equivocal.[11] The pharmacological actions of digoxin usually result in electrocardiogram changes, including ST depression or T wave inversion, which do not indicate toxicity. PR interval prolongation, however, may be a sign of digoxin toxicity. Additionally, increased intracellular Ca2+ may cause a type of arrhythmia called bigeminy (coupled beats), eventually ventricular tachycardia or fibrillation. The combination of increased (atrial) arrhythmogenesis and inhibited atrioventricular conduction (for example paroxysmal atrial tachycardia with A-V block - so-called "PAT with block") is said to be pathognomonic (i.e. diagnostic) of digoxin toxicity.[12]
An often described, but rarely seen, adverse effect of digoxin is a disturbance of color vision (mostly yellow and green) called xanthopsia. Vincent van Gogh's "Yellow Period" may have somehow been influenced by concurrent digitalis therapy. Other oculotoxic effects of digoxin include generalized blurry vision, as well as seeing a "halo" around each point of light.[13] The latter effect can also be seen in van Gogh's Starry Night. Evidence of van Gogh's digoxin use is supported by multiple self-portraits that include the foxglove plant, from which digoxin is obtained. (e.g. Portrait of Dr. Gachet)
Digoxin plasma concentrations may increase while on antimalarial medication hydroxychloroquine (based on two case reports from 1982).[14]
In overdose, the usual supportive measures are needed. If arrhythmias prove troublesome, or malignant hyperkalaemia occurs (inexorably rising potassium level due to paralysis of the cell membrane-bound, ATPase-dependent Na/K pumps), the specific antidote is antidigoxin (antibody fragments against digoxin, trade names Digibind and Digifab).[15] Digoxin is not removed by hemodialysis or peritoneal dialysis with enough effectiveness to treat toxicity.
Digoxin has potentially dangerous interactions with verapamil,[16] amiodarone, erythromycin, and epinephrine (as would be injected with a local anesthetic).
Patients taking digoxin should avoid taking hawthorn.[17][18]
Pharmacokinetic properties
Digoxin is usually given orally, but can also be given by IV injection in urgent situations (the IV injection should be slow, and heart rhythm should be monitored). While IV therapy may be better tolerated (less nausea), digoxin has a very long distribution half-life into the cardiac tissue, which will delay its onset of action by a number of hours. The half-life is about 36 hours for patients with normal renal function, digoxin is given once daily, usually in 125-μg or 250-μg doses.
In patients with decreased kidney function, the half-life is considerably longer, along with decrease in Vd, calling for a reduction in dose or a switch to a different glycoside, such as digitoxin (not available in the United States), which has a much longer elimination half-life of around seven days, elimination is mainly by renal excretion and involves P-glycoprotein which leads to significant clinical interactions with other drugs commonly used in patients with heart problems. These include: spironolactone, verapamil and amiodarone. ( Inhibit P-glycoprotein that is mainly responsible for Digoxin Clearance )
Effective plasma levels vary depending on the medical indication. For congestive heart failure, levels between 0.5 and 1.0 ng/ml are recommended.[19] This recommendation is based on post hoc analysis of prospective trials, suggesting higher levels may be associated with increased mortality rates. For heart rate control (atrial fibrillation), plasma levels are less defined and are generally titrated to a goal heart rate. Typically, digoxin levels are considered therapeutic for heart rate control between 0.5 and 2.0 ng/ml (or 0.6 and 2.6 nmol/l).[20] In suspected toxicity or ineffectiveness, digoxin levels should be monitored. Plasma potassium levels also need to be closely controlled (see side effects below).
Quinidine, verapamil, and amiodarone increases plasma levels of digoxin (by displacing tissue binding sites and depressing renal digoxin clearance), so plasma digoxin must be monitored carefully.
Researchers at Yale University looked at data from an earlier study to see if digoxin affected men and women differently. That study determined digoxin, which has been used for centuries and makes the heart contract more forcefully, did not reduce deaths overall, but did result in less hospitalization. Researcher Dr. Harlan Krumholz said they were surprised to find women in the study who took digoxin died "more frequently" (33%) than women who took a placebo pill (29%). They calculated digoxin increased the risk of death in women by 23%. There was no difference in the death rate for men in the study.
Digoxin is also used as a standard control substance to test for p-glycoprotein inhibition.
Mechanisms of action
Digoxin’s primary mechanism of action involves inhibition of the Na+/K+ ATPase, mainly in the myocardium. This inhibition causes an increase in intracellular sodium levels, resulting in a reversal of the action of the sodium-calcium exchanger, which normally imports three extracellular sodium ions into the cell and transports one intracellular calcium ion out of the cell. The reversal of this exchange causes an increase in the intracellular calcium concentration that is available to the contractile proteins. Increased intracellular calcium lengthens phase 4 and phase 0 of the cardiac action potential, which leads to a decrease in heart rate.[21] Increased amounts of Ca2+ also leads to increased storage of calcium in the sarcoplasmic reticulum, causing a corresponding increase in the release of calcium during each action potential. This leads to increased contractility (the force of contraction) of the heart without increasing heart energy expenditure.
The inhibition of the sodium pump may also improve baroreceptor sensitivity in HF and may explain some of the neurohormonal effects of digoxin.[22] Digoxin also has important parasympathetic effects, particularly on the atrioventricular node.[23]
The main pharmacological effects of digoxin are on the heart. Extracardiac effects are responsible for some of the therapeutic and many of the adverse effects (see above). It exerts a mechanical effect as it increases myocardial contractility; however, the duration of the contractile response is only slightly increased.
Overall, the heart rate is decreased while blood pressure is increased, resulting in a net increase in stroke volume, leading to increased tissue perfusion. This causes the myocardium to work more efficiently, with optimized hemodynamics and an improved ventricular function curve.
Other electrical effects include a brief initial increase in action potential, followed by a decrease as the K+ conductance increases due to increased intracellular amounts of Ca2+ ions. The refractory period of the atria and ventricles is decreased, while it increases in the sinoatrial and AV nodes. A less negative resting membrane potential is made, leading to increased irritability.
There is also evidence that digoxin increases vagal activity, thereby decreasing heart rate by slowing depolarization of pacemaker cells in the AV node.[24] This negative chronotropic effect would therefore be synergistic with the direct effect on cardiac pacemaker cells. Digoxin is used widely in the treatment of various arrhythmias.
The conduction velocity increases in the atria, but decreases in the AV node. The effect upon Purkinje fibers and ventricles is negligible. Automaticity is also increased in the atria, AV node, Purkinje fibers, and ventricles.
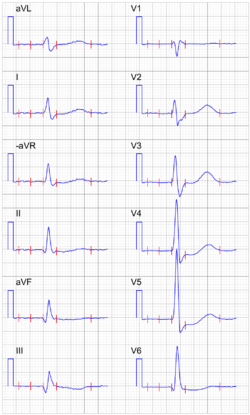
ECG changes seen in patient taking digoxin include increased PR interval (due to decreased AV conduction) and a shortened QT interval. Also, the T wave may be inverted and accompanied by ST depression. It may cause AV junctional rhythm and ectopic beats (bigeminy) resulting in ventricular tachycardia and fibrillation.
Slight vasodilation is seen in heart failure. This effect is contrary to effects that should be seen as a result of increased intracellular calcium levels, but this occurs since digoxin improves hemodynamics, which leads to restored angiotensin levels and decreased sympathetic discharge, causing indirect vasodilation.
Digoxin also affects the kidney by increased renal blood flow and increased glomerular filtration rate. A mild diuretic effect is seen only in heart failure.
History
Derivatives of plants of genus Digitalis have a long history of medical use. The English physician William Withering is credited with the first published description of the use of digitalis derivatives in his 1785 book "An Account of the Foxglove and some of its Medical Uses With Practical Remarks on Dropsy and Other Diseases".[25]
Society and culture
Charles Cullen admitted in 2003 to killing as many as 40 hospital patients with overdoses of heart medication—usually digoxin—at hospitals in New Jersey and Pennsylvania over his 16-year career as a nurse. On March 10, 2006, he was sentenced to 18 consecutive life sentences and is not eligible for parole.[26]
On April 25, 2008, the FDA issued a press release[27] alerting the public to a Class I recall of Digitek, a brand of digoxin produced by Mylan.[28] Some tablets had been released at double thickness and therefore double strength, causing some patients to experience digoxin toxicity. A class-action lawsuit against the Icelandic generic drug maker Actavis was announced two weeks later.[29]
On March 31, 2009, the FDA announced another generic digoxin pill recall by posting this company press release on the agency's web site: "Caraco Pharmaceutical Laboratories, Ltd. Announces a Nationwide Voluntary Recall of All Lots of Digoxin Tablets Due to Size Variability".
This March 31 press release from Caraco, a generic pharmaceutical company, states:
[All] tablets of Caraco brand Digoxin, USP, 0.125 mg, and Digoxin, USP, 0.25 mg, distributed prior to March 31, 2009, which are not expired and are within the expiration date of September, 2011, are being voluntarily recalled to the consumer level. The tablets are being recalled because they may differ in size and therefore could have more or less of the active ingredient, digoxin.
A 2008 study suggested digoxin has beneficial effects not only for the heart, but also in reducing the risk of certain kinds of cancer.[30] However, comments on this study suggested that digoxin is not effective at reducing cancer risk at therapeutic concentrations of the drug,[31] so the results need further investigation.[32]
In the Turkish film Once Upon a Time in Anatolia the prosecutor tells the doctor a story of a woman who died on the date she predicted she would die, well after delivering the baby. The doctor speculates that she may have taken high doses of digoxin to die of heart attack. There are hints that she may have been the prosecutor's wife who committed suicide because she couldn't take his one time affair.
Trade names
Digoxin preparations are marketed under the trade names Cardigox; Cardiogoxin; Cardioxin; Cardoxin; Coragoxine; Digacin; Digicor; Digomal; Digon; Digosin; Digoxine Navtivelle; Digoxina-Sandoz; Digoxin-Sandoz; Digoxin-Zori; Dilanacin; Eudigox; Fargoxin; Grexin; Lanacordin; Lanacrist; Lanicor; Lanikor; Lanorale; Lanoxicaps; Lanoxin; Lanoxin PG; Lenoxicaps; Lenoxin; Lifusin; Mapluxin; Natigoxin; Novodigal; Purgoxin; Sigmaxin; Sigmaxin-PG; Toloxin.
Spelling
Digoxin is orthographically interesting for being one of relatively few words in English in which a g followed by a/o/u is soft (usually e/i signal soft g and a/o/u signal hard g).
See also
References
- ↑ OED
- ↑ Hollman A (1996). "Digoxin comes from Digitalis lanata". British Medical Journal 312 (7035): 912. doi:10.1136/bmj.312.7035.912.
- 1 2 3 Vamos, M; Erath, JW; Hohnloser, SH (4 May 2015). "Digoxin-associated mortality: a systematic review and meta-analysis of the literature". European Heart Journal 36 (28): 1831–8. doi:10.1093/eurheartj/ehv143. PMID 25939649.
- ↑ "WHO Model List of EssentialMedicines" (PDF). World Health Organization. October 2013. Retrieved 22 April 2014.
- ↑ Sticherling C, Oral H, Horrocks J; et al. (November 2000). "Effects of digoxin on acute, atrial fibrillation-induced changes in atrial refractoriness" (pdf). Circulation 102 (20): 2503–2508. doi:10.1161/01.CIR.102.20.2503. PMID 11076824.
- ↑ Hallberg P, Lindbäck J, Lindahl B, Stenestrand U, Melhus H (October 2007). "Digoxin and mortality in atrial fibrillation: a prospective cohort study". European Journal of Clinical Pharmacology 63 (10): 959–971. doi:10.1007/s00228-007-0346-9. PMID 17684738.
- ↑ Ziff, Oliver J; Lane, Deirdre A; Samra, Monica; Griffith, Michael; Kirchhof, Paulus; Lip, Gregory Y H; Steeds, Richard P; Townend, Jonathan; Kotecha, Dipak (Aug 30, 2015). "Safety and efficacy of digoxin: systematic review and meta-analysis of observational and controlled trial data". BMJ: h4451. doi:10.1136/bmj.h4451.
- 1 2 Rossi S, ed. (2006). Australian Medicines Handbook 2006. Adelaide. ISBN 0-9757919-2-3.
- ↑ Tripathi KD (ed.). Essentials of Medical Pharmacology (6th ed.). New Delhi: Jaypee Publications. ISBN 81-8448-085-7.
- ↑ Moscovitz T, Aldrighi JM, Abrahanshon PA; et al. (April 2005). "Repercussions of digoxin, digitoxin and estradiol on the endometrial histomorphometry of oophorectomized mice". Gynecology and Endocrinology 20 (4): 213–220. doi:10.1080/09513590400021219. PMID 16019364.
- ↑ Thompson DF, Carter JR (1993). "Drug-induced gynecomastia". Pharmacotherapy 13 (1): 37–45. doi:10.1002/j.1875-9114.1993.tb02688.x. PMID 8094898.
- ↑ Doering W, König E, Sturm W (1977). "(title in German)" [Digitalis intoxication: specificity and significance of cardiac and extracardiac symptoms. part I: Patients with digitalis-induced arrhythmias (author's transl)]. Zeitschrift für Kardiologie (in German) 66 (3): 121–128. PMID 857452.
- ↑ Goldfrank LW (2006). Goldfrank's Toxicologic Emergencies (8th ed.). New York: McGraw-Hill.
- ↑ Leden I (1982). "Digoxin-hydroxychloroquine interaction?". Acta Medica Scandinavica 211 (5): 411–412. doi:10.1111/j.0954-6820.1982.tb01971.x. PMID 7113754.
- ↑ Flanagan RJ, Jones AL (2004). "Fab Antibody Fragments: Some Applications in Clinical Toxicology". Drug Safety 27 (14): 1115–1133. doi:10.2165/00002018-200427140-00004. PMID 15554746.
- ↑ Kaplanski J, Weinhouse E, Topaz M, Genchik G (1983). "Verapamil and digoxin: interactions in the rat". Research Communications in Chemical Pathology and Pharmacology 42 (3): 377–388. PMID 6665298.
- ↑ Dasgupta A, Kidd L, Poindexter BJ, Bick RJ. Interference of hawthorn on serum digoxin measurements by immunoassays and pharmacodynamic interaction with digoxin. Arch Pathol Lab Med. 2010 Aug;134(8):1188-92.
- ↑ Tankenow, Roberta; Tamer, Helen R.; Streetman, Daniel S.; Smith, Scott G.; Welton, Janice L.; Annesley, Thomas; Aaronson, Keith D.; Bleske, Barry E. Interaction Study between Digoxin and a Preparation of Hawthorn (Crataegus oxyacantha), J Clin Pharmacol 2003;43:637-642
- ↑ Hunt SA, Abraham, WT, Chin, MH; et al. (September 2005). "ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society" (pdf). Circulation 112 (12): e154–e235. doi:10.1161/CIRCULATIONAHA.105.167586. PMID 16160202.
- ↑ Page 700 in:
Richard C. Dart. Medical Toxicology. Lippincott Williams & Wilkins=year=2004. ISBN 9780781728454. - ↑ Tripathi KD (ed.). Essentials of Medical Pharmacology (6th ed.). New Delhi: Jaypee Publications. p. 498. ISBN 81-8448-085-7.
- ↑ Wang, W; Chen, JS; Zucker, IH (Jun 1990). "Carotid sinus baroreceptor sensitivity in experimental heart failure.". Circulation 81 (6): 1959–66. doi:10.1161/01.cir.81.6.1959. PMID 2344687.
- ↑ Gheorghiade, M; Adams KF, Jr; Colucci, WS (Jun 22, 2004). "Digoxin in the management of cardiovascular disorders.". Circulation 109 (24): 2959–64. doi:10.1161/01.cir.0000132482.95686.87. PMID 15210613.
- ↑ Goodman DJ; et al. (1975). "Effect of digoxin on atioventricular conduction. Studies in patients with and without cardiac autonomic innervation". Circulation 51 (2): 251–256. doi:10.1161/01.CIR.51.2.251. PMID 1089491.
- ↑ Withering, William (1785). An Account of the Foxglove and some of its Medical Uses With Practical Remarks on Dropsy and Other Diseases.
- ↑ "Victims' families set to confront killer". USA Today. 2006-01-01.
- ↑ "Recalls, Market Withdrawals & Safety Alerts". FDA. 2008-10-15. Retrieved 2011-11-08.
- ↑ "Urgent Digitek Digoxin Recall". U.S. Recall News. 2008-04-28. Retrieved 2009-07-25.
- ↑ "Patients Sue Icelandic Drugmaker Over Recalled Heart Drug". Wall Street Journal. 2008-05-09. Retrieved 2009-07-25.
- ↑ Zhang, H.; Qian, D. Z.; Tan, Y. S.; Lee, K.; Gao, P.; Ren, Y. R.; Rey, S.; Hammers, H.; Chang, D. (2008). "Inaugural Article: Digoxin and other cardiac glycosides inhibit HIF-1 synthesis and block tumor growth". Proceedings of the National Academy of Sciences (re: glycosides) 105 (50): 19579–19586. Bibcode:2008PNAS..10519579Z. doi:10.1073/pnas.0809763105. PMC 2604945. PMID 19020076.
- ↑ Lopez-Lazaro M (March 2009). "Digoxin, HIF-1, and cancer" (pdf). PNAS 106 (9): E26. Bibcode:2009PNAS..106...26L. doi:10.1073/pnas.0813047106. PMC 2651277. PMID 19240208.
- ↑ Zhang, H.; Semenza, G. L. (2009). "Reply to Lopez-Lazaro: Evidence that digoxin inhibits human cancer". Proceedings of the National Academy of Sciences 106 (9): E27. Bibcode:2009PNAS..106...27Z. doi:10.1073/pnas.0900125106.
Further reading
- Rang HP, Dale MM, Ritter JM, Moore PK (2003). Pharmacology (5th ed.). Edinburgh: Churchill Livingstone. ISBN 0-443-07145-4.
- Summary of Product Characteristics, Digoxin 0,125 mg, Zentiva a.s.
- Lüllmann (2003). Pharmakologie und Toxikologie (15th ed.). Georg Thieme Verlag. ISBN 3-13-368515-5.
- Lanatoside C (isolanid, Cedilanid - four glycoside analog), Digoxigenin (aglycone analog)
- Goldberger AD, Alexander GC. "Refitting the Foxglove: Digoxin Use in Contemporary Clinical
Practice". JAMA Internal Medicine. line feed character in |title= at position 61 (help)
External links
- Lanoxin
- U.S. National Library of Medicine: Drug Information Portal — Digoxin
- Commonly used website to calculate empiric digoxin doses for medical purposes for heart problems
- Protein Data Bank entry (useful for computational molecular dynamics): http://www.rcsb.org/pdb/explore.do?structureId=3B0W
| ||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||