Irritable bowel syndrome
| Irritable bowel syndrome | |
|---|---|
| Classification and external resources | |
| Specialty | Gastroenterology |
| ICD-10 | K58 |
| ICD-9-CM | 564.1 |
| DiseasesDB | 30638 |
| MedlinePlus | 000246 |
| eMedicine | med/1190 |
| Patient UK | Irritable bowel syndrome |
| MeSH | D043183 |
Irritable bowel syndrome (IBS) or spastic colon is a symptom-based diagnosis. It is characterized by chronic abdominal pain, discomfort, bloating, and alteration of bowel habits. Diarrhea or constipation may predominate, or they may alternate (classified as IBS-D, IBS-C, or IBS-A, respectively).
As a functional gastrointestinal disorder (FGID), IBS has no known organic cause; however, excessive mast cell activation has a central pathophysiological role in the disorder.[1][2] IBS is a disorder of the gut–brain axis.[1][3] Onset of IBS is more likely to occur after infections (postinfectious IBS-PI),[1][4] or a stressful life event,[5] but varies little with age.[6] For at least some individuals, abnormalities in the gut flora occur, and it has been theorised that these abnormalities result in inflammation and altered bowel function.[7]
A diagnosis of IBS may be made on the basis of symptoms, in the absence of worrisome features such as age of onset greater than 50 years, weight loss, bloody stool, signs of infection or colitis, or family history of inflammatory bowel disease.[8][9] Routine testing yields no abnormalities, although the bowels may be more sensitive to certain stimuli, such as balloon insufflation testing. Several conditions may present similarly, including coeliac disease,[10] non-celiac gluten sensitivity,[11][12][13] fructose malabsorption,[14] mast cell activation disorders,[1][15] parasitic infections,[16] inflammatory bowel disease, bile acid malabsorption, functional chronic constipation, small intestinal bacterial overgrowth, and chronic functional abdominal pain.
Although no cure for IBS is known, treatments to relieve symptoms exist. This including dietary adjustments, medication, and psychological interventions. Patient education and good doctor–patient relationships are also important.[17] Dietary measures that have been found to be effective include increasing soluble fiber intake.[18] IBS has no direct effect on life expectancy. IBS also does not harm intestines.[19] It is, however, a source of chronic pain, fatigue, and other symptoms, and contributes to work absenteeism.[20][21] It is common[22][23][24] and its effects on quality of life make it a disease with a high social cost.[25][26] Psychiatric disorders such as anxiety and major depression are common in IBS.[27]
Classification
IBS can be classified as either diarrhea-predominant (IBS-D), constipation-predominant (IBS-C), or with alternating stool pattern (IBS-A) or pain-predominant.[28] In some individuals, IBS may have an acute onset and develop after an infectious illness characterized by two or more of: fever, vomiting, diarrhea, or positive stool culture. This postinfective syndrome has consequently been termed "postinfectious IBS" (IBS-PI).
Signs and symptoms
The primary symptoms of IBS are abdominal pain or discomfort in association with frequent diarrhea or constipation and a change in bowel habits.[29] There may also be urgency for bowel movements, a feeling of incomplete evacuation (tenesmus), bloating, or abdominal distension.[30] In some cases, the symptoms are relieved by bowel movements.[17] People with IBS, more commonly than others, have gastroesophageal reflux, symptoms relating to the genitourinary system, chronic fatigue syndrome, fibromyalgia, headache, backache, and psychiatric symptoms such as depression and anxiety.[27][30] About a third of men and women who have IBS also report sexual dysfunction typically in the form of a reduction in libido.[31] Some studies indicate up to 60% of people with IBS also have a psychological disorder, typically anxiety or depression.[32]
Causes
While the causes of IBS are still unknown, it is believed that the entire gut–brain axis is affected.[1][33] Recent evidence indicates that there are abnormal levels of mast cell expression and activation in specific parts of the gastrointestinal tract which are unique to each subtype of IBS.[1]
The risk of developing IBS increases six-fold after acute gastrointestinal infection. Postinfection, further risk factors are young age, prolonged fever, anxiety, and depression.[34] Antibiotic use also appears to increase the risk of developing IBS.[35] Research has found that genetic defects in innate immunity and epithelial homeostasis increase the risk of developing both post-infectious as well as other forms of IBS.[36]
Post-infectious
Approximately 10 percent of IBS cases are triggered by an acute gastroenteritis infection. Genetic defects relating to the innate immune system and epithelial barrier as well as high stress and anxiety levels appear from evidence to increase the risk of developing post-infectious IBS. Post-infectious IBS usually manifests itself as the diarrhea predominant subtype. Evidence has demonstrated that the release of high levels of proinflammatory cytokines during acute enteric infection causes increased gut permeability leading to translocation of the commensal bacteria across the epithelial barrier resulting in significant damage to local tissues which is likely to result in chronic gut abnormalities in sensitive individuals. However, increased gut permeability is strongly associated with IBS regardless of whether IBS was initiated by an infection or not.[36]
Stress
Publications suggesting the role of brain-gut "axis" appeared in the 1990s[37] and childhood physical and psychological abuse is often associated with the development of IBS.[38]
Given the high levels of anxiety seen in IBS patients and the overlap with conditions such as fibromyalgia and chronic fatigue syndrome, a potential model of IBS involves a disruption of the stress system. The stress response in the body involves the HPA axis and the sympathetic nervous system, both of which have been shown to operate abnormally in IBS patients. Psychiatric illness or anxiety precedes IBS symptoms in two-thirds of patients, and psychological traits predispose previously healthy people to developing IBS after gastroenteritis.[39][40]
Small intestinal bacterial overgrowth
Small intestinal bacterial overgrowth occurs with greater frequency in patients who have been diagnosed with IBS compared to healthy controls. SIBO is most common in diarrhea predominate IBS but also occurs in constipation predominant IBS more frequently than healthy controls. Symptoms of SIBO include bloating, abdominal pain, diarrhea or constipation among others. IBS may be the result of the immune system interacting abnormally with gut microbiota resulting in an abnormal cytokine signalling profile.[41]
Fungal dysbiosis
There is growing evidence that alterations of gut microbiota (dysbiosis) is associated with the intestinal manifestations of IBS, but also with the psychiatric morbidity that coexists in up to 80% of patients with IBS.[42] The role of the gut mycobiota, and especially of the abnormal proliferation of the yeast Candida albicans in some patients with IBS, is under investigation.[43]
Protozoa

Protozoal infections can cause symptoms that mirror specific IBS subtypes,[3] e.g., infection by certain substypes of blastocystis hominis (blastocystosis) has a significant (possibly causal) relationship with IBS-D;[46][47] certain protozoal infections also occur more frequently in IBS patients.[48][49] Dientamoeba fragilis has also been considered a possible organism to study, though it is also found in people without IBS.[50]
Mechanism
There is evidence that abnormalities occur in the gut flora of individuals who suffer from IBS such a loss of diversity with a decrease in Bacteroidetes.[7] The changes in gut flora are most profound in individuals who have diarrhoea predominant IBS. Antibodies against common components (namely flagellin) of the commensal gut flora are a common occurrence in IBS affected individuals.[51] Chronic low-grade inflammation commonly occurs in IBS affected individuals with abnormalities found including increased enterochromaffin cells, intraepithelial lymphocytes, and mast cells resulting in chronic immune mediated inflammation of the gut mucosa.[52] Genetic, environmental, and psychological factors seem to be important in the development of IBS. Studies have shown that IBS has a genetic component even though there is a predominant influence of environmental factors.[53] IBS has been reported in greater quantities in multigenerational families with IBS than in the regular population.[54] This suggests a heritability factor. This factor does not follow classic Mendelian but is of the complex/multifactorial variety. 286 genes have been identified that are variably expressed in IBS-D patients.[55] Some research suggests the consumption of spicy foods is directly associated with IBS, especially in women.[56] Changes in serotonin metabolisms are thought to play a role in IBS development. One study found increased levels of serotonin transporter in the ileum of patients suffering from IBS.[57] Another study suggested that an increased expression of apoptotic genes in IBS can lead to an increase in mast cells in the intestine. This may lead to internalization of cellular adhesion proteins such as ZO-1 and occludin.[55]
Diagnosis
No specific laboratory or imaging test can be performed to diagnose irritable bowel syndrome. Diagnosis involves excluding conditions that produce IBS-like symptoms, and then following a procedure to categorize the patient's symptoms. Ruling out parasitic infections, lactose intolerance, small intestinal bacterial overgrowth, and celiac disease is recommended for all patients before a diagnosis of irritable bowel syndrome is made. In patients over 50 years old, they are recommended to undergo a screening colonoscopy.[58] IBS sufferers are at increased risk of being given inappropriate surgeries such as appendectomy, cholecystectomy, and hysterectomy due to their IBS symptoms being misdiagnosed as other medical conditions.[59]
Differential diagnosis
Colon cancer, inflammatory bowel disease, thyroid disorders, and giardiasis can all feature abnormal defecation and abdominal pain. Less common causes of this symptom profile are carcinoid syndrome, microscopic colitis, bacterial overgrowth, and eosinophilic gastroenteritis; IBS is, however, a common presentation, and testing for these conditions would yield low numbers of positive results, so it is considered difficult to justify the expense.[60]
Many patients, managed for years for IBS, may have indeed non-celiac gluten sensitivity (NCGS).[10] Gastrointestinal symptoms of IBS are clinically indistinguishable from those of NCGS, but the presence of any of the following non-intestinal manifestations suggest a possible NCGS: headache or migraine, “foggy mind”, chronic fatigue,[11] fibromyalgia,[12][61][62] joint and muscle pain,[11][12][13] leg or arm numbness,[11][12][13] tingling of the extremities,[11][13] dermatitis (eczema or skin rash),[11][13] atopic disorders,[11] allergy to one or more inhalants, foods or metals[11][12] (such as mites, graminaceae, parietaria, cat or dog hair, shellfish, or nickel[12]), depression,[11][12][13] anxiety,[12] anemia,[11][13] iron-deficiency anemia, folate deficiency, asthma, rhinitis, eating disorders,[12] neuropsychiatric disorders (such as schizophrenia,[13][63] autism,[12][13][63] peripheral neuropathy,[13][63] ataxia,[63] attention deficit hyperactivity disorder[11]) or autoimmune diseases.[11] An improvement with a gluten-free diet of immune-mediated symptoms, including autoimmune diseases, once reasonably ruled out coeliac disease and wheat allergy, is another way to realize a differential diagnosis.[11]
Because many causes of diarrhea give IBS-like symptoms, the American Gastroenterological Association published a set of guidelines for tests to be performed to rule out other causes for these symptoms. These include gastrointestinal infections, lactose intolerance, and coeliac disease. Research has suggested these guidelines are not always followed.[58] Once other causes have been excluded, the diagnosis of IBS is performed using a diagnostic algorithm. Well-known algorithms include the Manning criteria, the obsolete Rome I and II criteria, and the Kruis criteria, and studies have compared their reliability.[64] The more recent Rome III process was published in 2006. Physicians may choose to use one of these guidelines or may simply choose to rely on their own anecdotal experience with past patients. The algorithm may include additional tests to guard against misdiagnosis of other diseases as IBS. Such "red flag" symptoms may include weight loss, gastrointestinal bleeding, anemia, or nocturnal symptoms. However, red flag conditions may not always contribute to accuracy in diagnosis; for instance, as many as 31% of IBS patients have blood in their stool, many possibly from hemorrhoidal bleeding.[64]
The diagnostic algorithm identifies a name that can be applied to the patient's condition based on the combination of the patient's symptoms of diarrhea, abdominal pain, and constipation. For example, the statement "50% of returning travelers had developed functional diarrhea while 25% had developed IBS" would mean half the travelers had diarrhea while a quarter had diarrhea with abdominal pain. While some researchers believe this categorization system will help physicians understand IBS, others have questioned the value of the system and suggested all IBS patients have the same underlying disease but with different symptoms.[65]
Investigations
Investigations are performed to exclude other conditions:
- Stool microscopy and culture (to exclude infectious conditions)
- Blood tests: Full blood examination, liver function tests, erythrocyte sedimentation rate, and serological testing for coeliac disease
- Abdominal ultrasound (to exclude gallstones and other biliary tract diseases)
- Endoscopy and biopsies (to exclude peptic ulcer disease, coeliac disease, inflammatory bowel disease, and malignancies)
- Hydrogen breath testing (to exclude fructose and lactose malabsorption)
Misdiagnosis
Some common examples of misdiagnosis include infectious diseases, coeliac disease,[66] Helicobacter pylori,[67][68] parasites (non-protozoal).[3][69][70]
Coeliac disease in particular is often misdiagnosed as IBS. The American College of Gastroenterology recommends all patients with symptoms of IBS be tested for coeliac disease.[71]
Bile acid malabsorption is also sometimes missed in patients with diarrhea-predominant IBS. SeHCAT tests suggest around 30% of D-IBS patients have this condition, and most respond to bile acid sequestrants.[72]
Chronic use of certain sedative-hypnotic drugs, especially the benzodiazepines, may cause irritable bowel-like symptoms that can lead to a misdiagnosis of irritable bowel syndrome.[73]
Comorbidities
Several medical conditions, or comorbidities, appear with greater frequency in patients diagnosed with IBS.
- Neurological/Psychiatric: A study of 97,593 individuals with IBS identified comorbidities such as headache, fibromyalgia, and depression.[74] IBS occurs in 51% of chronic fatigue syndrome patients and 49% of fibromyalgia patients, and psychiatric disorders occur in 94% of IBS patients.[27]
- Inflammatory bowel disease: IBS may be a type of low-grade inflammatory bowel disease.[75] Researchers have suggested IBS and IBD are interrelated diseases,[76] noting that patients with IBD experience IBS-like symptoms when their IBD is in remission.[77][78] A three-year study found that patients diagnosed with IBS were 16.3 times more likely to be diagnosed with IBD during the study period.[79] Serum markers associated with inflammation have also been found in patients with IBS.
- Abdominal surgery: IBS patients were at increased risk of having unnecessary gall bladder removal surgery not due to an increased risk of gallstones, but rather to abdominal pain, awareness of having gallstones, and inappropriate surgical indications.[80] These patients also are 87% more likely to undergo abdominal and pelvic surgery and three times more likely to undergo gallbladder surgery.[81] Also, IBS patients were twice as likely to undergo hysterectomy.[82]
- Endometriosis: One study reported a statistically significant link between migraine headaches, IBS, and endometriosis.[83]
- Other chronic disorders: Interstitial cystitis may be associated with other chronic pain syndromes, such as irritable bowel syndrome and fibromyalgia. The connection between these syndromes is unknown.[84]
Management
A number of treatments have been found to be effective including: fiber, talk therapy, antispasmodic and antidepressant medication, and peppermint oil.[85][86][87]
Diet
Studies have shown that up to 70% of IBS patients benefited from eating a low FODMAP diet. Symptoms most likely to improve from such a diet include urgency, flatulence, bloating, abdominal pain, and altered stool output. One national guideline advises a low FODMAP diet for managing IBS when other dietary and lifestyle measures have been unsuccessful.[88] This diet restricts various carbohydrates which are poorly absorbed in the small intestine, as well as fructose and lactose, which are similarly poorly absorbed in those with intolerances to them. Reduction of fructose and fructan has been shown to reduce IBS symptoms in a dose-dependent manner in patients with fructose malabsorption and IBS.[89]
Some IBS patients believe they have some form of dietary intolerance; however, tests attempting to predict food sensitivity in IBS have proven disappointing. A small study reported that an IgG antibody test was somewhat effective in determining food sensitivity in IBS patients, with patients on the elimination diet experiencing 10% greater symptom-reduction than those on a sham diet.[90] However, more research is necessary before IgG testing can be recommended.[91]
FODMAPs diet
A diet restricted in fermentable oligo- di- and monosaccharides and polyols (FODMAPs) now has an evidence base sufficiently strong to recommend its widespread application in conditions such as IBS and IBD.[92] They also state the restriction of FODMAPs globally, rather than individually, controls the symptoms of functional gut disorders (e.g., IBS), and the majority of IBD patients respond just as well. It is more successful than restricting only fructose and fructans, which are also FODMAPs, as is recommended for those with fructose malabsorption. Longer-term compliance with the diet was high.
Fiber
Some evidence suggests soluble fiber supplementation (e.g., psyllium/ispagula husk) is effective.[18] It acts as a bulking agent, and for many IBS-D patients, allows for a more consistent stool. For IBS-C patients, it seems to allow for a softer, moister, more easily passable stool.
However, insoluble fiber (e.g., bran) has not been found to be effective for IBS.[93][94] In some people, insoluble fiber supplementation may aggravate symptoms.[95][96]
Fiber might be beneficial in those who have a predominance of constipation. In people who have IBS-C, soluble fiber can reduce overall symptoms, but will not reduce pain. The research supporting dietary fiber contains conflicting, small studies complicated by the heterogeneity of types of fiber and doses used.[97]
One meta-analysis found only soluble fiber improved global symptoms of irritable bowel, but neither type of fiber reduced pain.[97] An updated meta-analysis by the same authors also found soluble fiber reduced symptoms, while insoluble fiber worsened symptoms in some cases.[98] Positive studies have used 10–30 grams per day of psyllium.[99][100] One study specifically examined the effect of dose, and found 20 g of ispaghula husk were better than 10 g and equivalent to 30 g per day.[101]
Medication
Medications may consist of stool softeners and laxatives in IBS-C and antidiarrheals (e.g., opiate, opioid, or opioid analogs such as loperamide, codeine, diphenoxylate) in IBS-D for mild symptoms and stronger opiates such as morphine and oxycodone for severe cases.[102][103][104]
Drugs affecting serotonin (5-HT) in the intestines can help reduce symptoms.[105] On the other hand, many IBS-D patients report that SSRI type medications exacerbate spasms and diarrhea. This is thought to be due to the large number of serotonin receptors in the gut. 5HT3 antagonists such as ondansetron are effective in postinfectious IBS and diarrhoea-dominant IBS due to their blockade of serotonin on 5HT3 receptors in the gut; the reason for their benefit is believed to be that excessive serotonin in the gut is thought to play a role in the pathogenesis of some subtypes of IBS. Certain atypical antipsychotic medications, such as clozapine and olanzapine, may also provide relief due to serotonergic properties these agents possess, acting on the same receptors as other medications in this specific category.[106] Benefits may include reduced diarrhoea, reduced abdominal cramps, and improved general well-being. Any nausea present may also respond to 5HT3 antagonists owing to their antiemetic properties.[107] Serotonin stimulates the gut motility and so agonists can help constipation-predominate irritable bowel, while antagonists can help diarrhea-predominant irritable bowel. Selective serotonin reuptake inhibitors, SSRIs, frequently prescribed for panic and/or anxiety disorder and depression, affect serotonin in the gut, as well as the brain. The bowels are highly dependent on serotonin for neural communication. "Selective serotonin reuptake inhibitor antidepressants seem to promote global well-being in some patients with irritable bowel syndrome and, possibly, some improvement in abdominal pain and bowel symptoms, but this effect appears to be independent of improved depression. Further research is required."[108]
Mast cells and the compound that they secrete are central to the pathophysiology and implicated in the treatment of IBS;[1] some of the secreted mast cell mediators (and associated receptors) which have been implicated in symptoms of IBS or specific subtypes include: histamine (HRH1, HRH2, HRH3), tryptase and chymase (PAR2), serotonin (5-HT3), PGD2 (DP1).[1] Histamine also causes epithelial secretion of chloride ions and water (associated with secretory diarrhea) by signaling through a receptor or ligand-gated ion channel that has not been identified as of 2015.[1] A 2015 review noted that both H1-antihistamines and mast cell stabilizers have shown efficacy in reducing pain associated with visceral hypersensitivity in IBS;[1] other lower quality studies have also suggested the benefit of these agents for IBS.[1] In a related review on idiopathic mast cell activation syndromes (including IBS), a combined treatment approach using antileukotrienes, H1/H2-antihistamines, and a mast cell stabilizer are suggested.[15]
Laxatives
For patients who do not adequately respond to dietary fiber, osmotic laxatives such as polyethylene glycol, sorbitol, and lactulose can help avoid "cathartic colon" which has been associated with stimulant laxatives.[109] Among the osmotic laxatives, doses of 17–26 g/d of polyethylene glycol have been well studied. Lubiprostone (Amitiza) is a gastrointestinal agent used for the treatment of idiopathic chronic constipation and constipation-predominant IBS. It is well tolerated in adults, including elderly patients. As of July 20, 2006, lubiprostone had not been studied in pediatric patients. Lubiprostone is a bicyclic fatty acid (prostaglandin E1 derivative) that acts by specifically activating ClC-2 chloride channels on the apical aspect of gastrointestinal epithelial cells, producing a chloride-rich fluid secretion. These secretions soften the stool, increase motility, and promote spontaneous bowel movements. Unlike many laxative products, lubiprostone does not show signs of tolerance, dependency, or altered serum electrolyte concentration.
Antispasmodics
The use of antispasmodic drugs (e.g., anticholinergics such as hyoscyamine or dicyclomine) may help patients, especially those with cramps or diarrhea. A meta-analysis by the Cochrane Collaboration concludes if seven patients are treated with antispasmodics, one patient will benefit.[102] Antispasmodics can be divided in two groups: neurotropics and musculotropics.
- Neurotropics — for example, phenobarbitals such as Donnatal or atropine — act at the nerve fibre of the parasympathicus, but also affect other nerves, causing side effects in many patients.
- Musculotropics, such as mebeverine, act directly at the smooth muscle of the gastrointestinal tract, relieving spasm without affecting normal gut motility. Since this action is not mediated by the autonomic nervous system, the usual anticholinergic side effects are absent.
Discontinuation of proton pump inhibitors
Proton pump inhibitors (PPIs) used to suppress stomach acid production may cause bacterial overgrowth leading to IBS symptoms. Discontinuation of PPIs in selected individuals has been recommended as it may lead to an improvement or resolution of IBS symptoms.[110]
Tricyclic antidepressants
Strong evidence indicates low doses of tricyclic antidepressants can be effective for IBS. However, the evidence is less robust as to the effectiveness of other antidepressant classes such as SSRIs.[94][96]
Serotonin agonists
- Tegaserod (Zelnorm), a selective 5-HT4 agonist for IBS-C, is available for relieving IBS constipation in women and chronic idiopathic constipation in men and women. On March 30, 2007, the FDA requested Novartis Pharmaceuticals to voluntarily discontinue marketing of tegaserod based on the recently identified finding of an increased risk of serious cardiovascular adverse events (heart problems) associated with use of the drug. Novartis agreed to voluntarily suspend marketing of the drug in the United States and in many other countries. On July 27, 2007, the FDA approved a limited-treatment IND program for tegaserod in the US to allow restricted access to the medication for patients in need if no comparable alternative drug or therapy is available to treat the disease. The FDA had issued two previous warnings about the serious consequences of tegaserod. In 2005, it was rejected as an IBS medication by the European Union. Tegaserod, marketed as Zelnorm in the United States, was the only agent approved to treat the multiple symptoms of IBS (in women only), including constipation, abdominal pain, and bloating.
- Selective serotonin reuptake inhibitor antidepressants (SSRIs), because of their serotonergic effect, would seem to help IBS, especially patients who are constipation predominant. Initial crossover studies[111] and randomized controlled trials[112][113][114] support this role.
Serotonin antagonists
Alosetron, a selective 5-HT3 antagonist for IBS-D and cilansetron (also a selective 5-HT3 antagonist) were trialed for IBS. Due to severe adverse effects, namely ischemic colitis and severe constipation, they are not available or recommended.[96]
Other agents
Magnesium aluminum silicates and alverine citrate drugs can be effective for IBS.[96]
Evidence is conflicting about the benefit of antidepressants in IBS. Some meta-analyses have found a benefit, while others have not.[115] A meta-analysis of randomized controlled trials of mainly TCAs found three patients have to be treated with TCAs for one patient to improve.[116] A separate randomized controlled trial found TCAs are best for patients with IBS-D.[117]
Rifaximin can be used as an effective treatment for abdominal bloating and flatulence,[118][119] giving more credibility to the potential role of bacterial overgrowth in some patients with IBS.[120]
Domperidone, a dopamine receptor blocker and a parasympathomimetic, has been shown to reduce bloating and abdominal pain as a result of an accelerated colon transit time and reduced faecal load, that is, a relief from 'hidden constipation'; defecation was similarly improved.[121]
The use of opioids is controversial due to the potential risk of tolerance, physical dependence, and addiction, but can be the only relief for some diarrhea-predominant cases when other treatment has been ineffective.[122]
SIBO therapy
Statistically significant reduction in IBS symptoms occurs following antibiotic therapy for small intestinal bacterial overgrowth.[123] However, recent research has shown that the lactulose hydrogen breath test does not actually measure SIBO, and that SIBO is unlikely to be the cause of IBS.[124]
Psychological therapies
The mind-body or brain-gut interactions has been proposed for IBS, and is gaining increasing research attention.[94] Hypnosis can improve mental well-being, and cognitive behavioural therapy can provide psychological coping strategies for dealing with distressing symptoms, as well as help suppress thoughts and behaviours that increase the symptoms of IBS,[94][96] although the evidence base for effectiveness of psychotherapy and hypnosis is weak and such therapies are in general not recommended.[59] However, in treatment resistant cases where pharmacological therapies over a period of at least 12 months have failed to give relief, NICE clinical guidelines recommend that consideration should be given to psychological treatment strategies such as cognitive behavioural therapy [CBT], hypnotherapy and/or psychological therapy.[125]
Stress relief
Reducing stress may reduce the frequency and severity of IBS symptoms. Techniques that may be helpful include:
- Relaxation techniques such as meditation
- Physical activities such as yoga or tai chi
- Regular exercise such as swimming, walking, or running[126]
Probiotics
Probiotics can be beneficial in the treatment of IBS; taking 10 billion to 100 billion beneficial bacteria per day is recommended for beneficial results. However, further research is needed on individual strains of beneficial bacteria for more refined recommendations.[94][127] Probiotics have positive effects such as enhancing the intestinal mucosal barrier, providing a physical barrier, bacteriocin production (resulting in reduced numbers of pathogenic and gas-producing bacteria), reducing intestinal permeability and bacterial translocation, and regulating the immune system both locally and systemically among other beneficial effects.[59] Probiotics may also have positive effects on the gut-brain axis by their positive effects countering the effects of stress on gut immunity and gut function.[128]
A number of probiotics have been found to be effective, including Lactobacillus plantarum,[59] and Bifidobacteria infantis;[129] but one review found only Bifidobacteria infantis showed efficacy.[130] B. infantis may have effects beyond the gut via it causing a reduction of proinflammatory cytokine activity and elevation of blood tryptophan levels, which may cause an improvement in symptoms of depression.[131] Some yogurt is made using probiotics that may help ease symptoms of IBS.[132] A probiotic yeast called Saccharomyces boulardii has some evidence of effectiveness in the treatment of irritable bowel syndrome.[133]
Certain probiotics have different effects on certain symptoms of IBS. For example, Bifidobacterium breve, B. longum, and Lactobacillus acidophilus have been found to alleviate abdominal pain. B. breve, B. infantis, L. casei, or L. plantarum species alleviated distension symptoms. B. breve, B. infantis, L. casei, L. plantarum, B. longum, L. acidophilus, L. bulgaricus, and Streptococcus salivarius ssp. thermophilus have all been found to affect flatulence levels. Most clinical studies show probiotics do not improve straining, sense of incomplete evacuation, stool consistency, fecal urgency, or stool frequency, although a few clinical studies did find some benefit of probiotic therapy. The evidence is conflicting for whether probiotics improve overall quality of life scores.[134]
Probiotics may exert their beneficial effects on IBS symptoms via preserving the gut microbiota, normalisation of cytokine blood levels, improving the intestinal transit time, decreasing small intestine permeability, and by treating small intestinal bacterial overgrowth of fermenting bacteria.[134]
Herbal remedies
Peppermint oil appears useful.[135] Safety during pregnancy has not been established, however, and caution is required not to chew or break the enteric coating; otherwise, gastroesophageal reflux may occur as a result of lower esophageal sphincter relaxation. Occasionally, nausea and perianal burning occur as side effects.[94] Iberogast, a multi-herbal extract, was found to be superior in efficacy to placebo.[136] Commiphora mukul and Plantago ovata[137]
Only limited evidence exists for the effectiveness of other herbal remedies for IBS. As with all herbs, it is wise to be aware of possible drug interactions and adverse effects.[94]
Yoga
Yoga may be effective for some IBS patients, especially poses which exercise the lower abdomen.[96]
Acupuncture
A meta-analysis found no benefits of acupuncture relative to placebo for IBS symptom severity or IBS-related quality of life.[138] Acupuncture might be beneficial for some patients with IBS, but current evidence does not support its use.[94]
Epidemiology
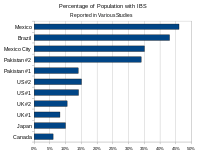
The prevalence of IBS varies by country and by age range examined. The bar graph at right shows the percentage of the population reporting symptoms of IBS in studies from various geographic regions (see table below for references). The following table contains a list of studies performed in different countries that measured the prevalence of IBS and IBS-like symptoms:
| Percentage of population reporting symptoms of IBS in various studies from various geographic areas | |||
|---|---|---|---|
| Country | Prevalence | Author/year | Notes |
| Canada | 6%[22] | Boivin, 2001 | |
| Japan | 10%[139] | Quigley, 2006 | Study measured prevalence of GI abdominal pain/cramping |
| United Kingdom | 8.2%[140]
10.5%[23] |
Ehlin, 2003 Wilson, 2004 |
Prevalence increased substantially 1970–2004 |
| United States | 14.1%[141] | Hungin, 2005 | Most undiagnosed |
| United States | 15%[22] | Boivin, 2001 | Estimate |
| Pakistan | 14%[142] | Jafri, 2007 | Much more common in 16–30 age range. Of IBS patients, 56% male, 44% female |
| Pakistan | 34%[143] | Jafri, 2005 | College students |
| Mexico City | 35%[24] | Schmulson, 2006 | n=324. Also measured functional diarrhea and functional vomiting. High rates attributed to "stress of living in a populated city." |
| Brazil | 43%[139] | Quigley, 2006 | Study measured prevalence of GI abdominal pain/cramping |
| Mexico | 46%[139] | Quigley, 2006 | Study measured prevalence of GI abdominal pain/cramping |
Gender
Women are around two to three times more likely to be diagnosed with IBS and four to five times more likely to seek specialty care for it than men.[144] These differences likely reflect a combination of both biological (sex) and social (gender) factors. People diagnosed with IBS are usually younger than 45 years old.[19] Studies of female patients with IBS show symptom severity often fluctuates with the menstrual cycle, suggesting hormonal differences may play a role.[145] Endorsement of gender-related traits has been associated with quality of life and psychological adjustment in IBS.[146] Gender differences in healthcare-seeking may also play a role.[147] Gender differences in trait anxiety may contribute to lower pain thresholds in women, putting them at greater risk for a number of chronic pain disorders.[148] Finally, sexual trauma is a major risk factor for IBS, with as many as 33% of all patients reporting such abuse. Because women are at higher risk of sexual abuse than men, gender-related risk of abuse may contribute to the higher prevalence of IBS in women.[149]
History
One of the first references to the concept of an "irritable bowel" appeared in the Rocky Mountain Medical Journal in 1950.[150] The term was used to categorize patients who developed symptoms of diarrhea, abdominal pain, and constipation, but where no well-recognized infective cause could be found. Early theories suggested the irritable bowel was caused by a psychosomatic or mental disorder.
Economics
In the US
The aggregate cost of irritable bowel syndrome in the United States has been estimated at $1.7–10 billion in direct medical costs, with an additional $20 billion in indirect costs, for a total of $21.7–30 billion.[26] A study by a managed care company comparing medical costs of IBS patients to non-IBS controls identified a 49% annual increase in medical costs associated with a diagnosis of IBS.[151] IBS patients incurred average annual direct costs of $5,049 and $406 in out-of-pocket expenses in 2007.[152] A study of workers with IBS found that they reported a 34.6% loss in productivity, corresponding to 13.8 hours lost per 40 hour week.[20] A study of employer-related health costs from a Fortune 100 company conducted with data from the 1990s found IBS patients incurred US $4527 in claims costs vs. $3276 for controls.[153] A study on Medicaid costs conducted in 2003 by the University of Georgia's College of Pharmacy and Novartis found IBS was associated in an increase of $962 in Medicaid costs in California, and $2191 in North Carolina. IBS patients had higher costs for physician visits, outpatients visits, and prescription drugs. The study suggested the costs associated with IBS were comparable to those found in asthma patients.[154]
Research
Individuals with IBS have been found to have decreased diversity and numbers of bacteroidetes microbiota. Preliminary research into the effectiveness of fecal microbiota transplant in the treatment of IBS has been very favourable with a 'cure' rate of between 36 percent and 60 percent with remission of core IBS symptoms persisting at 9 and 19 months follow up.[155][156]
There is increasing evidence for the effectiveness of mesalazine an aminosalicylate drug in the treatment of IBS.[157] Mesalazine is a drug with anti-inflammatory properties that has been reported to significantly reduce immune mediated inflammation in the gut of IBS affected individuals with mesalazine therapy resulting in improved IBS symptoms as well as feelings of general wellness in IBS affected people. It has also been observed that mesalazine therapy helps to normalise the gut flora which is often abnormal in people who have IBS. The therapeutic benefits of mesalazine may be the result of improvements to the epithelial barrier function.[158]
An IgG-mediated food intolerance diet led to a 24% greater deterioration in symptoms compared to those on the elimination diet and food elimination based on IgG antibodies may be effective in reducing IBS symptoms and is worthy of further biomedical research.[90] The main problem with this study was that the differences in symptoms were only observed in exclusion diets is limited, treatment based on “abnormally” high IgG antibodies cannot be recommended.[159]
Differences in visceral sensitivity and intestinal physiology have been noted in IBS. Mucosal barrier reinforcement in response to oral 5-HTP was absent in IBS compared to controls.[160] IBS/IBD individuals are less often HLA DQ2/8 positive than in upper functional gastrointestinal disease and healthy populations.[161]
A questionnaire in 2006 designed to identify patients’ perceptions about IBS, their preferences on the type of information they need, and educational media and expectations from health care providers revealed misperceptions about IBS developing into other conditions, including colitis, malnutrition, and cancer. The survey found IBS patients were most interested in learning about foods to avoid (60%), causes of IBS (55%), medications (58%), coping strategies (56%), and psychological factors related to IBS (55%). The respondents indicated they wanted their physicians to be available by phone or e-mail following a visit (80%), have the ability to listen (80%), and provide hope (73%) and support (63%).[162]
See also
References
- 1 2 3 4 5 6 7 8 9 10 11 Wouters MM, Vicario M, Santos J (2015). "The role of mast cells in functional GI disorders". Gut 65: 155–168. doi:10.1136/gutjnl-2015-309151. PMID 26194403.
Functional gastrointestinal disorders (FGIDs) are characterized by chronic complaints arising from disorganized brain-gut interactions leading to dysmotility and hypersensitivity. The two most prevalent FGIDs, affecting up to 16–26% of worldwide population, are functional dyspepsia and irritable bowel syndrome. ... It is well established that mast cell activation can generate epithelial and neuro-muscular dysfunction and promote visceral hypersensitivity and altered motility patterns in FGIDs, postoperative ileus, food allergy and inflammatory bowel disease.
▸ Mast cells play a central pathophysiological role in IBS and possibly in functional dyspepsia, although not well defined.
▸ Increased mast cell activation is a common finding in the mucosa of patients with functional GI disorders. ...
▸ Treatment with mast cell stabilisers offers a reasonably safe and promising option for the management of those patients with IBS non-responding to conventional approaches, though future studies are warranted to evaluate efficacy and indications. - ↑ "irritable bowel syndrome" at Dorland's Medical Dictionary
- 1 2 3 Stark D, van Hal S, Marriott D, Ellis J, Harkness J; Van Hal; Marriott; Ellis; Harkness (2007). "Irritable bowel syndrome: a review on the role of intestinal protozoa and the importance of their detection and diagnosis". Int. J. Parasitol. 37 (1): 11–20. doi:10.1016/j.ijpara.2006.09.009. PMID 17070814.
- ↑ Spiller R, Garsed K; Garsed (May 2009). "Postinfectious irritable bowel syndrome". Gastroenterology 136 (6): 1979–88. doi:10.1053/j.gastro.2009.02.074. PMID 19457422.
- ↑ Chang L (March 2011). "The role of stress on physiologic responses and clinical symptoms in irritable bowel syndrome". Gastroenterology 140 (3): 761–5. doi:10.1053/j.gastro.2011.01.032. PMC 3039211. PMID 21256129.
- ↑ Saito YA, Schoenfeld P, Locke GR; Schoenfeld; Locke Gr (August 2002). "The epidemiology of irritable bowel syndrome in North America: a systematic review". Am. J. Gastroenterol. 97 (8): 1910–5. doi:10.1111/j.1572-0241.2002.05913.x. PMID 12190153.
- 1 2 Khanna S, Tosh PK; Tosh (January 2014). "A clinician's primer on the role of the microbiome in human health and disease". Mayo Clin. Proc. 89 (1): 107–14. doi:10.1016/j.mayocp.2013.10.011. PMID 24388028.
- ↑ Malagelada JR (2006). "A symptom-based approach to making a positive diagnosis of irritable bowel syndrome with constipation". International journal of clinical practice 60 (1): 57–63. doi:10.1111/j.1368-5031.2005.00744.x. PMID 16409429.
- ↑ Cash BD, Schoenfeld P, Chey WD; Schoenfeld; Chey (2002). "The utility of diagnostic tests in irritable bowel syndrome patients: A systematic review". The American journal of gastroenterology 97 (11): 2812–9. doi:10.1111/j.1572-0241.2002.07027.x. PMID 12425553.
- 1 2 Levy J, Bernstein L, Silber N (Dec 2014). "Celiac disease: an immune dysregulation syndrome". Curr Probl Pediatr Adolesc Health Care 44 (11): 324–7. doi:10.1016/j.cppeds.2014.10.002. PMID 25499458.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Fasano A, Sapone A, Zevallos V, Schuppan D (May 2015). "Nonceliac gluten sensitivity". Gastroenterology (Review) 148 (6): 1195–204. doi:10.1053/j.gastro.2014.12.049. PMID 25583468.
IBS-like symptoms, such as abdominal pain, gas, distension, and irregular bowel movements, frequently are reported and therefore make it difficult to distinguish NCGS from IBS induced by other causes. The differential diagnosis is facilitated for patients who also experience extraintestinal symptoms, including headache or frank migraine, foggy mind, chronic fatigue, joint and muscle pain, tingling of the extremities, leg or arm numbness, eczema, anemia, depression, or for patients who report a reduction in immune-mediated (including autoimmune) symptoms on a GFD. (...) Therefore, it is possible to consider some subjects with NCGS to be typical IBS patients and vice versa: a subgroup of IBS patients may have NCGS. This last scenario was highlighted in subjects affected by the diarrheapredominant variant of IBS —particularly those with HLA-DQ2 and/or DQ8 genotypes (associated with celiac disease).
- 1 2 3 4 5 6 7 8 9 10 Volta U, Caio G, De Giorgio R, Henriksen C, Skodje G, Lundin KE (Jun 2015). "Non-celiac gluten sensitivity: a work-in-progress entity in the spectrum of wheat-related disorders". Best Pract Res Clin Gastroenterol 29 (3): 477–91. doi:10.1016/j.bpg.2015.04.006. PMID 26060112.
- 1 2 3 4 5 6 7 8 9 10 Catassi C, Bai J, Bonaz B, Bouma G, Calabrò A, Carroccio A, Castillejo G, Ciacci C, Cristofori F, Dolinsek J, Francavilla R, Elli L, Green P, Holtmeier W, Koehler P, Koletzko S, Meinhold C, Sanders D, Schumann M, Schuppan D, Ullrich R, Vécsei A, Volta U, Zevallos V, Sapone A, Fasano A (2013). "Non-celiac gluten sensitivity: the new frontier of gluten related disorders". Nutrients (Review) 5 (10): 3839–3853. doi:10.3390/nu5103839. ISSN 2072-6643. PMC 3820047. PMID 24077239.
- ↑ "Fruktosemalabsorption" (PDF). Retrieved 2012-10-21.
- 1 2 Frieri M (2015). "Mast Cell Activation Syndrome". Clin Rev Allergy Immunol. doi:10.1007/s12016-015-8487-6. PMID 25944644.
- ↑ Larry S. Roberts; Gerald Dee Schmidt; John Janovy (2005). Foundations of Parasitology. McGraw-Hill Higher Education. ISBN 978-0-07-111271-0.
- 1 2 Mayer EA (April 2008). "Clinical practice. Irritable bowel syndrome". N. Engl. J. Med. 358 (16): 1692–9. doi:10.1056/NEJMcp0801447. PMC 3816529. PMID 18420501.
- 1 2 Moayyedi, P; Quigley, EM; Lacy, BE; Lembo, AJ; Saito, YA; Schiller, LR; Soffer, EE; Spiegel, BM; Ford, AC (September 2014). "The effect of fiber supplementation on irritable bowel syndrome: a systematic review and meta-analysis.". The American journal of gastroenterology 109 (9): 1367–74. doi:10.1038/ajg.2014.195. PMID 25070054.
- 1 2 "Irritable Bowel Syndrome: MedlinePlus". www.nlm.nih.gov. Retrieved 2015-12-11.
- 1 2 Paré P, Gray J, Lam S, Balshaw R, Khorasheh S, Barbeau M, Kelly S, McBurney CR; Gray; Lam; Balshaw; Khorasheh; Barbeau; Kelly; McBurney (2006). "Health-related quality of life, work productivity, and health care resource utilization of subjects with irritable bowel syndrome: baseline results from LOGIC (Longitudinal Outcomes Study of Gastrointestinal Symptoms in Canada), a naturalistic study". Clinical therapeutics 28 (10): 1726–35; discussion 1710–1. doi:10.1016/j.clinthera.2006.10.010. PMID 17157129.
- ↑ Maxion-Bergemann S, Thielecke F, Abel F, Bergemann R; Thielecke; Abel; Bergemann (2006). "Costs of irritable bowel syndrome in the UK and US". PharmacoEconomics 24 (1): 21–37. doi:10.2165/00019053-200624010-00002. PMID 16445300.
- 1 2 3 Boivin M (October 2001). "Socioeconomic impact of irritable bowel syndrome in Canada". Can. J. Gastroenterol. 15 (Suppl B): 8B–11B. PMID 11694908.
- 1 2 Wilson S, Roberts L, Roalfe A, Bridge P, Singh S; Roberts; Roalfe; Bridge; Singh (July 2004). "Prevalence of irritable bowel syndrome: a community survey". Br J Gen Pract 54 (504): 495–502. PMC 1324800. PMID 15239910.
- 1 2 Schmulson M, Ortíz O, Santiago-Lomeli M, Gutiérrez-Reyes G, Gutiérrez-Ruiz MC, Robles-Díaz G, Morgan D; Ortíz; Santiago-Lomeli; Gutiérrez-Reyes; Gutiérrez-Ruiz; Robles-Díaz; Morgan (2006). "Frequency of functional bowel disorders among healthy volunteers in Mexico City" (PDF). Dig Dis. 24 (3–4): 342–7. doi:10.1159/000092887. PMID 16849861.
- ↑ Richard Lea & Peter J. Whorwell. "ref name="LEA-WHORWELL-2001"". Ideas.repec.org. Retrieved 2012-10-21.
- 1 2 Hulisz D (2004). "The burden of illness of irritable bowel syndrome: current challenges and hope for the future". J Manag Care Pharm. 10 (4): 299–309. PMID 15298528.
- 1 2 3 Whitehead WE, Palsson O, Jones KR; Palsson; Jones (2002). "Systematic review of the comorbidity of irritable bowel syndrome with other disorders: what are the causes and implications?". Gastroenterology 122 (4): 1140–56. doi:10.1053/gast.2002.32392. PMID 11910364.
- ↑ Holten KB, Wetherington A, Bankston L; Wetherington; Bankston (2003). "Diagnosing the patient with abdominal pain and altered bowel habits: is it irritable bowel syndrome?". Am Fam Physician 67 (10): 2157–62. PMID 12776965.
- ↑ Schmulson MW, Chang L; Chang (1999). "Diagnostic approach to the patient with irritable bowel syndrome". Am. J. Med. 107 (5A): 20S–26S. doi:10.1016/S0002-9343(99)00278-8. PMID 10588169.
- 1 2 Talley NJ (2006). "Irritable bowel syndrome". Intern Med J 36 (11): 724–8. doi:10.1111/j.1445-5994.2006.01217.x. PMC 1761148. PMID 17040359.
- ↑ Sperber AD, Dekel R; Dekel (Apr 2010). "Irritable Bowel Syndrome and Co-morbid Gastrointestinal and Extra-gastrointestinal Functional Syndromes" (PDF). J Neurogastroenterol Motil 16 (2): 113–9. doi:10.5056/jnm.2010.16.2.113. PMC 2879857. PMID 20535341.
- ↑ "IBS and Depression Connection and Treatments". Webmd.com. Retrieved 2012-10-21.
- ↑ Ohman L, Simrén M; Simrén (2010). "Pathogenesis of IBS: Role of inflammation, immunity and neuroimmune interactions". Nature Reviews Gastroenterology & Hepatology 7 (3): 163–73. doi:10.1038/nrgastro.2010.4. PMID 20101257.
- ↑ Thabane M, Kottachchi DT, Marshall JK; Kottachchi; Marshall (2007). "Systematic review and meta-analysis: The incidence and prognosis of post-infectious irritable bowel syndrome". Aliment Pharmacol Ther 26 (4): 535–44. doi:10.1111/j.1365-2036.2007.03399.x. PMID 17661757.
- ↑ Shanahan F, Quigley EM; Quigley (May 2014). "Manipulation of the microbiota for treatment of IBS and IBD-challenges and controversies". Gastroenterology 146 (6): 1554–63. doi:10.1053/j.gastro.2014.01.050. PMID 24486051.
- 1 2 Beatty JK, Bhargava A, Buret AG (2014). "Post-infectious irritable bowel syndrome: mechanistic insights into chronic disturbances following enteric infection". World J. Gastroenterol. 20 (14): 3976–85. doi:10.3748/wjg.v20.i14.3976. PMC 3983453. PMID 24744587.
- ↑ Fukudo S, Nomura T, Muranaka M, Taguchi F; Nomura; Muranaka; Taguchi (1993). "Brain-gut response to stress and cholinergic stimulation in irritable bowel syndrome. A preliminary study". J. Clin. Gastroenterol. 17 (2): 133–41. doi:10.1097/00004836-199309000-00009. PMID 8031340.
- ↑ Barreau F, Ferrier L, Fioramonti J, Bueno L; Ferrier; Fioramonti; Bueno (September 2007). "New Insights in the Etiology and Pathophysiology of Irritable Bowel Syndrome: Contribution of Neonatal Stress Models". Pediatric Research 62 (3): 240–245. doi:10.1203/PDR.0b013e3180db2949. PMID 17622962.
- ↑ Spiller, R; Aziz, Q; Creed, F; Emmanuel, A; Houghton, L; Hungin, P; Jones, R; Kumar, D; Rubin, G; Trudgill, N; Whorwell, P (1 December 2007). "Guidelines on the irritable bowel syndrome: mechanisms and practical management". Gut 56 (12): 1770–1798. doi:10.1136/gut.2007.119446.
- ↑ Fukudo, Shin (19 January 2007). "Role of corticotropin-releasing hormone in irritable bowel syndrome and intestinal inflammation". Journal of Gastroenterology 42 (S17): 48–51. doi:10.1007/s00535-006-1942-7.
- ↑ Ghoshal, UC.; Srivastava, D. (Mar 2014). "Irritable bowel syndrome and small intestinal bacterial overgrowth: meaningful association or unnecessary hype.". World J Gastroenterol 20 (10): 2482–91. doi:10.3748/wjg.v20.i10.2482. PMID 24627585.
- ↑ Collins, SM (August 2014). "A role for the gut microbiota in IBS.". Nature reviews. Gastroenterology & hepatology 11 (8): 497–505. doi:10.1038/nrgastro.2014.40. PMID 24751910.
- ↑ Santelmann, H; Howard, JM (January 2005). "Yeast metabolic products, yeast antigens and yeasts as possible triggers for irritable bowel syndrome.". European journal of gastroenterology & hepatology 17 (1): 21–6. doi:10.1097/00042737-200501000-00005. PMID 15647635.
- ↑ Lagacé-Wiens PR, VanCaeseele PG, Koschik C; Vancaeseele; Koschik (2006). "Dientamoeba fragilis: an emerging role in intestinal disease". Canadian Medical Association Journal 175 (5): 468–9. doi:10.1503/cmaj.060265. PMC 1550747. PMID 16940260.
- ↑ Amin OM (2002). "Seasonal prevalence of intestinal parasites in the United States during 2000". Am. J. Trop. Med. Hyg. 66 (6): 799–803. PMID 12224595.
- ↑ Wawrzyniak I, Poirier P, Viscogliosi E, Dionigia M, Texier C, Delbac F, Alaoui HE (2013). "Blastocystis, an unrecognized parasite: an overview of pathogenesis and diagnosis". Ther Adv Infect Dis 1 (5): 167–78. doi:10.1177/2049936113504754. PMC 4040727. PMID 25165551.
Recent in vitro and in vivo studies have shed new light on the pathogenic power of this parasite, suggesting that Blastocystis sp. infection is associated with a variety of gastrointestinal disorders, may play a significant role in irritable bowel syndrome, and may be linked with cutaneous lesions (urticaria).
- ↑ Roberts T, Stark D, Harkness J, Ellis J (2014). "Update on the pathogenic potential and treatment options for Blastocystis sp". Gut Pathog 6: 17. doi:10.1186/1757-4749-6-17. PMC 4039988. PMID 24883113.
- ↑ Yakoob J, Jafri W, Jafri N, Khan R, Islam M, Beg MA, Zaman V; Jafri; Jafri; Khan; Islam; Beg; Zaman (2004). "Irritable bowel syndrome: in search of an etiology: role of Blastocystis hominis". Am. J. Trop. Med. Hyg. 70 (4): 383–5. PMID 15100450.
- ↑ Giacometti A, Cirioni O, Fiorentini A, Fortuna M, Scalise G; Cirioni; Fiorentini; Fortuna; Scalise (1999). "Irritable bowel syndrome in patients with Blastocystis hominis infection". Eur. J. Clin. Microbiol. Infect. Dis. 18 (6): 436–9. doi:10.1007/s100960050314. PMID 10442423.
- ↑ Windsor JJ, Macfarlane L; MacFarlane (May 2005). "Irritable bowel syndrome: the need to exclude Dientamoeba fragilis". Am. J. Trop. Med. Hyg. 72 (5): 501; author reply 501–2. PMID 15891119. Retrieved November 4, 2009.
- ↑ Cremon C, Carini G, De Giorgio R, Stanghellini V, Corinaldesi R, Barbara G; Carini; De Giorgio; Stanghellini; Corinaldesi; Barbara (May 2010). "Intestinal dysbiosis in irritable bowel syndrome: etiological factor or epiphenomenon?". Expert Rev. Mol. Diagn. 10 (4): 389–93. doi:10.1586/erm.10.33. PMID 20465494.
- ↑ Schmulson M, Bielsa MV, Carmona-Sánchez R; et al. (2014). "[Microbiota, gastrointestinal infections, low-grade inflammation, and antibiotic therapy in irritable bowel syndrome: an evidence-based review]". Rev Gastroenterol Mex (in Spanish) 79 (2): 96–134. doi:10.1016/j.rgmx.2014.01.004. PMID 24857420.
- ↑ Tally, N J (Dec 2006). "Genes and environment in irritable bowel syndrome: one step forward". GUT 55 (12): 1694–1696. doi:10.1136/gut.2006.108837. PMC 1856457. PMID 17124153. Retrieved 6 December 2014.
- ↑ Saito, Yuri A. (Mar 2011). "The Role of Genetics in IBS". Gastroenterology Clinics of North America 40 (1): 45–67. doi:10.1016/j.gtc.2010.12.011. PMC 3056499. PMID 21333900. Retrieved 6 December 2014.
- 1 2 Martínez, Cristina; Vicario, María; Ramos, Laura; Lobo, Beatriz; Mosquera, Jose Luis; Alonso, Carmen; Sánchez, Alex; Guilarte, Mar; Antolín, María; Torres, Inés de; González-Castro, Ana M.; Pigrau, Marc; Saperas, Esteban; Azpiroz, Fernando; Santos, Javier (May 2012). "The Jejunum of Diarrhea-Predominant Irritable Bowel Syndrome Shows Molecular Alterations in the Tight Junction Signaling Pathway That Are Associated With Mucosal Pathobiology and Clinical Manifestations". The American Journal of Gastroenterology 107 (5): 736–746. doi:10.1038/ajg.2011.472. PMID 22415197.
- ↑ Esmaillzadeh A, Keshteli AH, Hajishafiee M, Feizi A, Feinle-Bisset C, Adibi P; Keshteli; Hajishafiee; Feizi; Feinle-Bisset; Adibi (2013). "Consumption of spicy foods and the prevalence of irritable bowel syndrome". World Journal of Gastroenterology 19 (38): 6465–71. doi:10.3748/wjg.v19.i38.6465. PMC 3801318. PMID 24151366.
- ↑ Wendelbo I; Mazzawi; El-Salhy (Jan 2014). "A Increased serotonin transporter immunoreactivity intensity in the ileum of patients with irritable bowel disease". J Mol Med Rep 9 (1): 180–4. doi:10.3892/mmr.2013.1784. PMID 24213511.
- 1 2 Yawn BP, Lydick E, Locke GR, Wollan PC, Bertram SL, Kurland MJ; Lydick; Locke; Wollan; Bertram; Kurland (2001). "Do published guidelines for evaluation of Irritable Bowel Syndrome reflect practice?". BMC gastroenterology 1: 11. doi:10.1186/1471-230X-1-11. PMC 59674. PMID 11701092.
- 1 2 3 4 Bixquert Jiménez M (Aug 2009). "Treatment of irritable bowel syndrome with probiotics. An etiopathogenic approach at last?". Rev Esp Enferm Dig 101 (8): 553–64. doi:10.4321/s1130-01082009000800006. PMID 19785495.
- ↑ C. Hauser (August 29, 2005). Mayo Clinic Gastroenterology and Hepatology Board Review. CRC Press. p. 225–. ISBN 978-0-203-50274-7. Retrieved October 24, 2010.
- ↑ Rossi A, Di Lollo AC, Guzzo MP, Giacomelli C, Atzeni F, Bazzichi L, Di Franco M (2015). "Fibromyalgia and nutrition: what news?". Clin Exp Rheumatol 33 (1 Suppl 88): S117–25. PMID 25786053.
- ↑ San Mauro Martín I, Garicano Vilar E, Collado Yurrutia L, Ciudad Cabañas MJ (Dec 2014). "[Is gluten the great etiopathogenic agent of disease in the XXI century?] [Article in Spanish]" (PDF). Nutr Hosp 30 (6): 1203–10. doi:10.3305/nh.2014.30.6.7866. PMID 25433099.
- 1 2 3 4 Lebwohl B, Ludvigsson JF, Green PH (Oct 2015). "Celiac disease and non-celiac gluten sensitivity". BMJ (Review) 5: 351:h4347. doi:10.1136/bmj.h4347. PMC 4596973. PMID 26438584.
- 1 2 Fass R, Longstreth GF, Pimentel M, Fullerton S, Russak SM, Chiou CF, Reyes E, Crane P, Eisen G, McCarberg B, Ofman J; Longstreth; Pimentel; Fullerton; Russak; Chiou; Reyes; Crane; Eisen; McCarberg; Ofman (2001). "Evidence- and consensus-based practice guidelines for the diagnosis of irritable bowel syndrome". Arch. Intern. Med. 161 (17): 2081–8. doi:10.1001/archinte.161.17.2081. PMID 11570936.
- ↑ Talley NJ (2006). "A unifying hypothesis for the functional gastrointestinal disorders: really multiple diseases or one irritable gut?". Reviews in gastroenterological disorders 6 (2): 72–8. PMID 16699476.
- ↑ Spiegel BM, DeRosa VP, Gralnek IM, Wang V, Dulai GS; Derosa; Gralnek; Wang; Dulai (2004). "Testing for celiac sprue in irritable bowel syndrome with predominant diarrhea: a cost-effectiveness analysis". Gastroenterology 126 (7): 1721–32. doi:10.1053/j.gastro.2004.03.012. PMID 15188167.
- ↑ Su YC, Wang WM, Wang SY, Lu SN, Chen LT, Wu DC, Chen CY, Jan CM, Horowitz M; Wang; Wang; Lu; Chen; Wu; Chen; Jan; Horowitz (August 2000). "The association between Helicobacter pylori infection and functional dyspepsia in patients with irritable bowel syndrome". Am. J. Gastroenterol. 95 (8): 1900–5. doi:10.1111/j.1572-0241.2000.02252.x. PMID 10950033.
- ↑ Gerards C, Leodolter A, Glasbrenner B, Malfertheiner P; Leodolter; Glasbrenner; Malfertheiner (2001). "H. pylori infection and visceral hypersensitivity in patients with irritable bowel syndrome". Dig Dis 19 (2): 170–3. doi:10.1159/000050673. PMID 11549828.
- ↑ Grazioli B, Matera G, Laratta C, Schipani G, Guarnieri G, Spiniello E, Imeneo M, Amorosi A, Focà A, Luzza F; Matera; Laratta; Schipani; Guarnieri; Spiniello; Imeneo; Amorosi; Focà; Luzza (March 2006). "Giardia lamblia infection in patients with irritable bowel syndrome and dyspepsia: a prospective study". World J. Gastroenterol. 12 (12): 1941–4. PMC 4087522. PMID 16610003.
- ↑ Vernia P, Ricciardi MR, Frandina C, Bilotta T, Frieri G; Ricciardi; Frandina; Bilotta; Frieri (1995). "Lactose malabsorption and irritable bowel syndrome. Effect of a long-term lactose-free diet". The Italian journal of gastroenterology 27 (3): 117–21. PMID 7548919.
- ↑ Brandt LJ, Chey WD, Foxx-Orenstein AE, Schiller LR, Schoenfeld PS, Spiegel BM, Talley NJ, Quigley EM; Brandt; Chey; Foxx-Orenstein; Schiller; Schoenfeld; Spiegel; Talley; Quigley (January 2009). "An Evidence-Based Systematic Review on the Management of Irritable Bowel Syndrome" (PDF). Am J Gastroenterology 104 (Supplement 1): S1–S35. doi:10.1038/ajg.2008.122. PMID 19521341.
- ↑ Wedlake L, A'Hern R, Russell D, Thomas K, Walters JR, Andreyev HJ; a'Hern; Russell; Thomas; Walters; Andreyev (2009). "Systematic review: the prevalence of idiopathic bile acid malabsorption as diagnosed by SeHCAT scanning in patients with diarrhoea-predominant irritable bowel syndrome". Alimentary pharmacology & therapeutics 30 (7): 707–17. doi:10.1111/j.1365-2036.2009.04081.x. PMID 19570102.
- ↑ Professor C Heather Ashton (1987). "Benzodiazepine Withdrawal: Outcome in 50 Patients". British Journal of Addiction 82: 655–671.
- ↑ Cole JA, Rothman KJ, Cabral HJ, Zhang Y, Farraye FA; Rothman; Cabral; Zhang; Farraye (2006). "Migraine, fibromyalgia, and depression among people with IBS: a prevalence study". BMC gastroenterology 6: 26. doi:10.1186/1471-230X-6-26. PMC 1592499. PMID 17007634.
- ↑ Bercik P, Verdu EF, Collins SM; Verdu; Collins (2005). "Is irritable bowel syndrome a low-grade inflammatory bowel disease?". Gastroenterol. Clin. North Am. 34 (2): 235–45, vi–vii. doi:10.1016/j.gtc.2005.02.007. PMID 15862932.
- ↑ Quigley EM (2005). "Irritable bowel syndrome and inflammatory bowel disease: interrelated diseases?". Chinese journal of digestive diseases 6 (3): 122–32. doi:10.1111/j.1443-9573.2005.00202.x. PMID 16045602.
- ↑ Simrén M, Axelsson J, Gillberg R, Abrahamsson H, Svedlund J, Björnsson ES; Axelsson; Gillberg; Abrahamsson; Svedlund; Björnsson (2002). "Quality of life in inflammatory bowel disease in remission: the impact of IBS-like symptoms and associated psychological factors". Am. J. Gastroenterol. 97 (2): 389–96. doi:10.1111/j.1572-0241.2002.05475.x. PMID 11866278.
- ↑ Minderhoud IM, Oldenburg B, Wismeijer JA, van Berge Henegouwen GP, Smout AJ; Oldenburg; Wismeijer; Van Berge Henegouwen; Smout (2004). "IBS-like symptoms in patients with inflammatory bowel disease in remission; relationships with quality of life and coping behavior". Dig. Dis. Sci. 49 (3): 469–74. doi:10.1023/B:DDAS.0000020506.84248.f9. PMID 15139501.
- ↑ García Rodríguez LA, Ruigómez A, Wallander MA, Johansson S, Olbe L; Ruigómez; Wallander; Johansson; Olbe (2000). "Detection of colorectal tumor and inflammatory bowel disease during follow-up of patients with initial diagnosis of irritable bowel syndrome". Scand. J. Gastroenterol. 35 (3): 306–11. doi:10.1080/003655200750024191. PMID 10766326.
- ↑ Corazziari E, Attili AF, Angeletti C, De Santis A; Attili, AF; Angeletti, C; De Santis, A (2008). "Gallstones, cholecystectomy and irritable bowel syndrome (IBS) MICOL population-based study". Dig Liver Dis. 40 (12): 944–50. doi:10.1016/j.dld.2008.02.013. PMID 18406218.
- ↑ Cole JA, Yeaw JM, Cutone JA, Kuo B, Huang Z, Earnest DL, Walker AM; Yeaw; Cutone; Kuo; Huang; Earnest; Walker (2005). "The incidence of abdominal and pelvic surgery among patients with irritable bowel syndrome". Dig. Dis. Sci. 50 (12): 2268–75. doi:10.1007/s10620-005-3047-1. PMID 16416174.
- ↑ Longstreth GF, Yao JF; Yao (2004). "Irritable bowel syndrome and surgery: a multivariable analysis". Gastroenterology 126 (7): 1665–73. doi:10.1053/j.gastro.2004.02.020. PMID 15188159.
- ↑ Tietjen GE, Bushnell CD, Herial NA, Utley C, White L, Hafeez F; Bushnell; Herial; Utley; White; Hafeez (2007). "Endometriosis is associated with prevalence of comorbid conditions in migraine". Headache 47 (7): 1069–78. doi:10.1111/j.1526-4610.2007.00784.x. PMID 17635599.
- ↑ "Interstitial cystitis: Risk factors". Mayo Clinic. January 20, 2009.
- ↑ Ford AC, Talley NJ, Spiegel BM, Foxx-Orenstein AE, Schiller L, Quigley EM, Moayyedi P; Talley; Spiegel; Foxx-Orenstein; Schiller; Quigley; Moayyedi (2008). "Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: systematic review and meta-analysis". BMJ 337: a2313. doi:10.1136/bmj.a2313. PMC 2583392. PMID 19008265.
- ↑ Ford, AC; Quigley, EM; Lacy, BE; Lembo, AJ; Saito, YA; Schiller, LR; Soffer, EE; Spiegel, BM; Moayyedi, P (September 2014). "Effect of antidepressants and psychological therapies, including hypnotherapy, in irritable bowel syndrome: systematic review and meta-analysis". The American journal of gastroenterology 109 (9): 1350–65; quiz 1366. doi:10.1038/ajg.2014.148. PMID 24935275.
- ↑ Khanna, Reena; MacDonald, John K.; Levesque, Barrett G. (2014-07-01). "Peppermint oil for the treatment of irritable bowel syndrome: a systematic review and meta-analysis". Journal of Clinical Gastroenterology 48 (6): 505–512. doi:10.1097/MCG.0b013e3182a88357. ISSN 1539-2031. PMID 24100754.
- ↑ Staudacher HM, Irving PM, Lomer MC, Whelan K (April 2014). "Mechanisms and efficacy of dietary FODMAP restriction in IBS". Nat Rev Gastroenterol Hepatol (Review) 11 (4): 256–66. doi:10.1038/nrgastro.2013.259. PMID 24445613.
- ↑ Fedewa A, Rao SS (2014). "Dietary fructose intolerance, fructan intolerance and FODMAPs". Curr Gastroenterol Rep 16 (1): 370. doi:10.1007/s11894-013-0370-0. PMC 3934501. PMID 24357350.
- 1 2 Atkinson W, Sheldon TA, Shaath N, Whorwell PJ; Sheldon; Shaath; Whorwell (2004). "Food elimination based on IgG antibodies in irritable bowel syndrome: a randomised controlled trial". Gut 53 (10): 1459–64. doi:10.1136/gut.2003.037697. PMC 1774223. PMID 15361495.
- ↑ Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC (2006). "Functional bowel disorders". Gastroenterology 131 (2): 688. doi:10.1053/j.gastro.2006.06.027.
- ↑ Gibson PR, Shepherd SJ; Shepherd (Feb 2010). "Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach". J Gastroenterol Hepatol. 25 (2): 252–8. doi:10.1111/j.1440-1746.2009.06149.x. PMID 20136989.
- ↑ Francis CY, Whorwell PJ; Whorwell (Jul 2, 1994). "[Bran and irritable bowel syndrome: time for reappraisal]". Lancet 344 (8914): 39–40. doi:10.1016/S0140-6736(94)91055-3. PMID 7912305.
- 1 2 3 4 5 6 7 8 Shen YH, Nahas R; Nahas (Feb 2009). "Complementary and alternative medicine for treatment of irritable bowel syndrome". Can Fam Physician 55 (2): 143–8. PMC 2642499. PMID 19221071.
- ↑ Bijkerk CJ, de Wit NJ, Muris JW, Whorwell PJ, Knottnerus JA, Hoes AW; De Wit; Muris; Whorwell; Knottnerus; Hoes (Aug 27, 2009). "[Soluble or insoluble fibre in irritable bowel syndrome in primary care? Randomised placebo controlled trial]". BMJ 339 (b3154): b3154. doi:10.1136/bmj.b3154. PMC 3272664. PMID 19713235.
- 1 2 3 4 5 6 Ducrotté P (Nov 2007). "[Irritable bowel syndrome: current treatment options]". Presse Med 36 (11 Pt 2): 1619–26. doi:10.1016/j.lpm.2007.03.008. PMID 17490849.
- 1 2 Bijkerk CJ, Muris JW, Knottnerus JA, Hoes AW, de Wit NJ; Muris; Knottnerus; Hoes; De Wit (2004). "Systematic review: the role of different types of fiber in the treatment of irritable bowel syndrome". Aliment Pharmacol Ther 19 (3): 245–51. doi:10.1111/j.0269-2813.2004.01862.x. PMID 14984370.
- ↑ Bijkerk CJ, de Wit NJ, Muris JW, Whorwell PJ, Knottnerus JA, Hoes AW; De Wit; Muris; Whorwell; Knottnerus; Hoes (2009). "Systematic Soluble or insoluble fiber in irritable bowel syndrome in primary care? Randomised placebo controlled trial". BMJ 339 (b): 3154–. doi:10.1136/bmj.b3154. PMC 3272664. PMID 19713235.
- ↑ Prior A, Whorwell PJ; Whorwell (1987). "Double blind study of ispaghula in irritable bowel syndrome". Gut 28 (11): 1510–3. doi:10.1136/gut.28.11.1510. PMC 1433676. PMID 3322956.
- ↑ Jalihal A, Kurian G; Kurian (1990). "Ispaghula therapy in irritable bowel syndrome: improvement in overall well-being is related to reduction in bowel dissatisfaction". J Gastroenterol Hepatol 5 (5): 507–13. doi:10.1111/j.1440-1746.1990.tb01432.x. PMID 2129822.
- ↑ Kumar A, Kumar N, Vij JC, Sarin SK, Anand BS; Kumar; Vij; Sarin; Anand (1987). "Optimum dosage of ispaghula husk in patients with irritable bowel syndrome: correlation of symptom relief with whole gut transit time and stool weight". Gut 28 (2): 150–5. doi:10.1136/gut.28.2.150. PMC 1432983. PMID 3030900.
- 1 2 Ruepert L, Quartero AO, de Wit NJ, van der Heijden GJ, Rubin G, Muris JW; Quartero; De Wit; Van Der Heijden; Rubin; Muris (2011). "Bulking agents, antispasmodics and antidepressants for the treatment of irritable bowel syndrome". Cochrane Database Syst Rev (8): CD003460. doi:10.1002/14651858.CD003460.pub3. PMID 21833945.
- ↑ Lesbros-Pantoflickova D, Michetti P, Fried M, Beglinger C, Blum AL; Michetti; Fried; Beglinger; Blum (2004). "Meta-analysis: The treatment of irritable bowel syndrome". Aliment Pharmacol Ther 20 (11–12): 1253–69. doi:10.1111/j.1365-2036.2004.02267.x. PMID 15606387.
- ↑ Jailwala J, Imperiale TF, Kroenke K; Imperiale; Kroenke (2000). "Pharmacologic treatment of the irritable bowel syndrome: a systematic review of randomized, controlled trials". Annals of Internal Medicine 133 (2): 136–47. doi:10.7326/0003-4819-133-2-200007180-00013. PMID 10896640.
- ↑ Talley NJ (2001). "Serotoninergic neuroenteric modulators". Lancet 358 (9298): 2061–8. doi:10.1016/S0140-6736(01)07103-3. PMID 11755632.
- ↑ Pae CU1, Lee SJ, Han C, Patkar AA, Masand PS; Lee; Han; Patkar; Masand (May 2013). "Atypical antipsychotics as a possible treatment option for irritable bowel syndrome". Expert Opin Investig Drugs 22 (5): 565–72. doi:10.1517/13543784.2013.782392. PMID 23506326.
- ↑ Spiller R, Lam C; Lam (July 2012). "An Update on Post-infectious Irritable Bowel Syndrome: Role of Genetics, Immune Activation, Serotonin and Altered Microbiome". J Neurogastroenterol Motil 18 (3): 258–68. doi:10.5056/jnm.2012.18.3.258. PMC 3400813. PMID 22837873.
- ↑ Creed F (2005). "How do SSRIs help patients with irritable bowel syndrome?". Gut 55 (8): 1065–1067. doi:10.1136/gut.2005.086348. PMC 1856284. PMID 16849340.
- ↑ Joo JS, Ehrenpreis ED, Gonzalez L, Kaye M, Breno S, Wexner SD, Zaitman D, Secrest K; Ehrenpreis; Gonzalez; Kaye; Breno; Wexner; Zaitman; Secrest (1998). "Alterations in colonic anatomy induced by chronic stimulant laxatives: the cathartic colon revisited". J Clin Gastroenterol 26 (4): 283–6. doi:10.1097/00004836-199806000-00014. PMID 9649012.
- ↑ Simrén M, Barbara G, Flint HJ, Spiegel BM, Spiller RC, Vanner S, Verdu EF, Whorwell PJ, Zoetendal EG; Barbara; Flint; Spiegel; Spiller; Vanner; Verdu; Whorwell; et al. (Jan 2013). "Intestinal microbiota in functional bowel disorders: a Rome foundation report". Gut 62 (1): 159–76. doi:10.1136/gutjnl-2012-302167. PMC 3551212. PMID 22730468.
- ↑ Tack J, Broekaert D, Fischler B, Van Oudenhove L, Gevers AM, Janssens J; Broekaert; Fischler; Van Oudenhove; Gevers; Janssens (2006). "A controlled crossover study of the selective serotonin reuptake inhibitor citalopram in irritable bowel syndrome". Gut 55 (8): 1095–103. doi:10.1136/gut.2005.077503. PMC 1856276. PMID 16401691.
- ↑ Vahedi H, Merat S, Rashidioon A, Ghoddoosi A, Malekzadeh R; Merat; Rashidioon; Ghoddoosi; Malekzadeh (2005). "The effect of fluoxetine in patients with pain and constipation-predominant irritable bowel syndrome: a double-blind randomized-controlled study". Aliment Pharmacol Ther 22 (5): 381–5. doi:10.1111/j.1365-2036.2005.02566.x. PMID 16128675.
- ↑ Creed F, Fernandes L, Guthrie E, Palmer S, Ratcliffe J, Read N, Rigby C, Thompson D, Tomenson B; Fernandes; Guthrie; Palmer; Ratcliffe; Read; Rigby; Thompson; Tomenson; North of England IBS Research Group (2003). "The cost-effectiveness of psychotherapy and paroxetine for severe irritable bowel syndrome". Gastroenterology 124 (2): 303–17. doi:10.1053/gast.2003.50055. PMID 12557136.
- ↑ Tabas G, Beaves M, Wang J, Friday P, Mardini H, Arnold G; Beaves; Wang; Friday; Mardini; Arnold (2004). "Paroxetine to treat irritable bowel syndrome not responding to high-fiber diet: a double-blind, placebo-controlled trial". Am J Gastroenterol 99 (5): 914–20. doi:10.1111/j.1572-0241.2004.04127.x. PMID 15128360.
- ↑ "UpToDate Inc.". (subscription required (help)).
- ↑ Jackson JL, O'Malley PG, Tomkins G, Balden E, Santoro J, Kroenke K; O'Malley; Tomkins; Balden; Santoro; Kroenke (2000). "Treatment of functional gastrointestinal disorders with antidepressant medications: a meta-analysis". Am J Med 108 (1): 65–72. doi:10.1016/S0002-9343(99)00299-5. PMID 11059442.
- ↑ Drossman DA, Toner BB, Whitehead WE, Diamant NE, Dalton CB, Duncan S, Emmott S, Proffitt V, Akman D, Frusciante K, Le T, Meyer K, Bradshaw B, Mikula K, Morris CB, Blackman CJ, Hu Y, Jia H, Li JZ, Koch GG, Bangdiwala SI; Toner; Whitehead; Diamant; Dalton; Duncan; Emmott; Proffitt; Akman; Frusciante; Le; Meyer; Bradshaw; Mikula; Morris; Blackman; Hu; Jia; Li; Koch; Bangdiwala (2003). "Cognitive-behavioral therapy versus education and desipramine versus placebo for moderate to severe functional bowel disorders". Gastroenterology 125 (1): 19–31. doi:10.1016/S0016-5085(03)00669-3. PMID 12851867.
- ↑ Pimentel M, Park S, Mirocha J, Kane SV, Kong Y; Park; Mirocha; Kane; Kong (2006). "The effect of a nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel syndrome: a randomized trial". Annals of Internal Medicine 145 (8): 557–63. doi:10.7326/0003-4819-145-8-200610170-00004. PMID 17043337.
- ↑ Sharara AI, Aoun E, Abdul-Baki H, Mounzer R, Sidani S, Elhajj I; Aoun; Abdul-Baki; Mounzer; Sidani; Elhajj (2006). "A randomized double-blind placebo-controlled trial of rifaximin in patients with abdominal bloating and flatulence". Am J Gastroenterol 101 (2): 326–33. doi:10.1111/j.1572-0241.2006.00458.x. PMID 16454838.
- ↑ Quigley EM (2006). "Germs, gas and the gut; the evolving role of the enteric flora in IBS". Am J Gastroenterol 101 (2): 334–5. doi:10.1111/j.1572-0241.2006.00445.x. PMID 16454839.
- ↑ Raahave D, Christensen E, Loud FB, Knudsen LL. Correlation of bowel symptoms with colonic transit, length, and faecal load in functional faecal retention 2009;56:83–8
- ↑ Warfield, Carol A.; Zahid H. Bajwa (2003). Principles and Practice of Pain Medicine. McGraw-Hill Professional. ISBN 0-07-144349-5.
- ↑ Lin HC (Aug 18, 2004). "Small intestinal bacterial overgrowth: a framework for understanding irritable bowel syndrome.". JAMA: the Journal of the American Medical Association 292 (7): 852–8. doi:10.1001/jama.292.7.852. PMID 15316000.
- ↑ Spiegel, Brennan M.R. (June 2011). "Questioning the Bacterial Overgrowth Hypothesis of Irritable Bowel Syndrome: An Epidemiologic and Evolutionary Perspective". Clinical Gastroenterology and Hepatology 9 (6): 461–469. doi:10.1016/j.cgh.2011.02.030.
- ↑ Irritable Bowel Syndrome in Adults: Diagnosis and management of irritable bowel syndrome in primary care; NICE clinical guideline 61, Issue Feb 2008
- ↑ "Irritable Bowel Syndrome (IBS) - Treatment - NHS Choices". Nhs.uk. Retrieved 2012-10-21.
- ↑ Nikfar S, Rahimi R, Rahimi F, Derakhshani S, Abdollahi M; Rahimi; Rahimi; Derakhshani; Abdollahi (December 2008). "Efficacy of probiotics in irritable bowel syndrome: a meta-analysis of randomized, controlled trials". Dis. Colon Rectum 51 (12): 1775–80. doi:10.1007/s10350-008-9335-z. PMID 18465170.
- ↑ Konturek PC, Brzozowski T, Konturek SJ; Brzozowski; Konturek (Dec 2011). "Stress and the gut: pathophysiology, clinical consequences, diagnostic approach and treatment options". J Physiol Pharmacol 62 (6): 591–9. PMID 22314561.
- ↑ "New Studies Examine the Evidence on Probiotics in IBS" (PDF) (Press release). American College of Gastroenterology. October 31, 2005.
- ↑ Brenner DM, Moeller MJ, Chey WD, Schoenfeld PS; Moeller; Chey; Schoenfeld (April 2009). "The utility of probiotics in the treatment of irritable bowel syndrome: a systematic review". Am. J. Gastroenterol. 104 (4): 1033–49; quiz 1050. doi:10.1038/ajg.2009.25. PMID 19277023.
- ↑ Aragon G, Graham DB, Borum M, Doman DB; Graham; Borum; Doman (Jan 2010). "Probiotic therapy for irritable bowel syndrome". Gastroenterol Hepatol (N Y) 6 (1): 39–44. PMC 2886445. PMID 20567539.
- ↑ "IBS diet: Can yogurt ease symptoms?". Mayo Clinic. May 21, 2008.
- ↑ McFarland, LV. (May 2010). "Systematic review and meta-analysis of Saccharomyces boulardii in adult patients". World J Gastroenterol 16 (18): 2202–22. doi:10.3748/wjg.v16.i18.2202. PMC 2868213. PMID 20458757.
- 1 2 Ortiz-Lucas M, Tobías A, Saz P, Sebastián JJ; Tobías; Saz; Sebastián (Jan 2013). "Effect of probiotic species on irritable bowel syndrome symptoms: A bring up to date meta-analysis". Rev Esp Enferm Dig 105 (1): 19–36. doi:10.4321/s1130-01082013000100005. PMID 23548007.
- ↑ Wilkins T, Pepitone C, Alex B, Schade RR; Pepitone; Alex; Schade (Sep 1, 2012). "Diagnosis and management of IBS in adults". American family physician 86 (5): 419–26. PMID 22963061.
- ↑ Rösch W, Liebregts T, Gundermann KJ, Vinson B, Holtmann G; Liebregts; Gundermann; Vinson; Holtmann (2006). "Phytotherapy for functional dyspepsia: a review of the clinical evidence for the herbal preparation STW 5". Phytomedicine : international journal of phytotherapy and phytopharmacology. 13 Suppl 5: 114–21. doi:10.1016/j.phymed.2006.03.022. PMID 16978851.
- ↑ Rahimi R, Shams-Ardekani MR, Abdollahi M; Shams-Ardekani; Abdollahi (2010). "A review of the efficacy of traditional Iranian medicine for inflammatory bowel disease". World journal of gastroenterology : WJG 16 (36): 4504–4514. doi:10.3748/wjg.v16.i36.4504. PMC 2945480. PMID 20857519.
- ↑ Manheimer E, Cheng K, Wieland LS, Min LS, Shen X, Berman BM, Lao L; Cheng; Wieland; Min; Shen; Berman; Lao (2012). "Acupuncture for treatment of irritable bowel syndrome". Cochrane Database Syst Rev 5 (5): CD005111. doi:10.1002/14651858.CD005111.pub3. PMC 3718572. PMID 22592702.
- 1 2 3 Quigley EM, Locke GR, Mueller-Lissner S, Paulo LG, Tytgat GN, Helfrich I, Schaefer E; Locke; Mueller-Lissner; Paulo; Tytgat; Helfrich; Schaefer (July 2006). "Prevalence and management of abdominal cramping and pain: a multinational survey". Aliment. Pharmacol. Ther. 24 (2): 411–9. doi:10.1111/j.1365-2036.2006.02989.x. PMID 16842469.
- ↑ Ehlin AG, Montgomery SM, Ekbom A, Pounder RE, Wakefield AJ; Montgomery; Ekbom; Pounder; Wakefield (August 2003). "Prevalence of gastrointestinal diseases in two British national birth cohorts". Gut 52 (8): 1117–21. doi:10.1136/gut.52.8.1117. PMC 1773740. PMID 12865268.
- ↑ Hungin AP, Chang L, Locke GR, Dennis EH, Barghout V; Chang; Locke; Dennis; Barghout (June 2005). "Irritable bowel syndrome in the United States: prevalence, symptom patterns and impact". Aliment. Pharmacol. Ther. 21 (11): 1365–75. doi:10.1111/j.1365-2036.2005.02463.x. PMID 15932367.
- ↑ Jafri W, Yakoob J, Jafri N, Islam M, Ali QM; Yakoob; Jafri; Islam; Ali (June 2007). "Irritable bowel syndrome and health seeking behaviour in different communities of Pakistan". J Pak Med Assoc 57 (6): 285–7. PMID 17629228.
- ↑ Jafri W, Yakoob J, Jafri N, Islam M, Ali QM; Yakoob; Jafri; Islam; Ali (2005). "Frequency of irritable bowel syndrome in college students". J Ayub Med Coll Abbottabad. 4 (17): 9–11. PMID 16599025.
- ↑ Payne S (2004). "Sex, gender, and irritable bowel syndrome: Making the connections". Gender medicine 1 (1): 18–28. doi:10.1016/S1550-8579(04)80007-X. PMID 16115580.
- ↑ Jackson NA, Houghton LA, Whorwell PJ, Currer B; Houghton; Whorwell; Currer (1994). "Does the menstrual cycle affect anorectal physiology?". Digestive diseases and sciences 39 (12): 2607–11. doi:10.1007/bf02087697. PMID 7995186.
- ↑ Voci SC, Cramer KM; Cramer (2009). "Gender-related traits, quality of life, and psychological adjustment among women with irritable bowel syndrome". Quality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation 18 (9): 1169–76. doi:10.1007/s11136-009-9532-9. PMID 19728159.
- ↑ Drossman DA, Li Z, Andruzzi E, Temple RD, Talley NJ, Thompson WG, Whitehead WE, Janssens J, Funch-Jensen P, Corazziari E; Li; Andruzzi; Temple; Talley; Thompson; Whitehead; Janssens; et al. (1993). "U.S. Householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact". Digestive diseases and sciences 38 (9): 1569–80. doi:10.1007/bf01303162. PMID 8359066.
- ↑ Goffaux P, Michaud K, Gaudreau J, Chalaye P, Rainville P, Marchand S; Michaud; Gaudreau; Chalaye; Rainville; Marchand (2011). "Sex differences in perceived pain are affected by an anxious brain". Pain 152 (9): 2065–73. doi:10.1016/j.pain.2011.05.002. PMID 21665365.
- ↑ Walker EA, Katon WJ, Roy-Byrne PP, Jemelka RP, Russo J; Katon; Roy-Byrne; Jemelka; Russo (1993). "Histories of sexual victimization in patients with irritable bowel syndrome or inflammatory bowel disease". The American Journal of Psychiatry 150 (10): 1502–6. doi:10.1176/ajp.150.10.1502. PMID 8379554.
- ↑ Brown PW (1950). "The irritable bowel syndrome". Rocky Mountain Medical Journal 47 (5): 343–6. PMID 15418074.
- ↑ Levy RL, Von Korff M, Whitehead WE, Stang P, Saunders K, Jhingran P, Barghout V, Feld AD; von Korff; Whitehead; Stang; Saunders; Jhingran; Barghout; Feld (2001). "Costs of care for irritable bowel syndrome patients in a health maintenance organization". Am J Gastroenterol 96 (11): 3122–9. doi:10.1111/j.1572-0241.2001.05258.x. PMID 11721759.
- ↑ Nyrop KA, Palsson OS, Levy RL, Korff MV, Feld AD, Turner MJ, Whitehead WE; Palsson; Levy; von Korff; Feld; Turner; Whitehead (2007). "Costs of health care for irritable bowel syndrome, chronic constipation, functional diarrhoea and functional abdominal pain". Aliment Pharmacol Ther 26 (2): 237–48. doi:10.1111/j.1365-2036.2007.03370.x. PMID 17593069.
- ↑ Leong SA, Barghout V, Birnbaum HG, Thibeault CE, Ben-Hamadi R, Frech F, Ofman JJ; Barghout; Birnbaum; Thibeault; Ben-Hamadi; Frech; Ofman (2003). "The economic consequences of irritable bowel syndrome: a US employer perspective". Arch. Intern. Med. 163 (8): 929–35. doi:10.1001/archinte.163.8.929. PMID 12719202.
- ↑ Martin BC, Ganguly R, Pannicker S, Frech F, Barghout V; Ganguly; Pannicker; Frech; Barghout (2003). "Utilization Patterns and Net Direct Medical Costs Medicaid of Irritable Bowel Syndrome". Curr Med Res Opin 19 (8): 771–80. doi:10.1185/030079903125002540. PMID 14687449.
- ↑ Aroniadis OC, Brandt LJ; Brandt (January 2013). "Fecal microbiota transplantation: past, present and future". Curr. Opin. Gastroenterol. 29 (1): 79–84. doi:10.1097/MOG.0b013e32835a4b3e. PMID 23041678.
- ↑ Smits LP, Bouter KE, de Vos WM, Borody TJ, Nieuwdorp M; Bouter; De Vos; Borody; Nieuwdorp (November 2013). "Therapeutic potential of fecal microbiota transplantation". Gastroenterology 145 (5): 946–53. doi:10.1053/j.gastro.2013.08.058. PMID 24018052.
- ↑ Klotz U (February 2012). "The pharmacological profile and clinical use of mesalazine (5-aminosalicylic acid)". Arzneimittelforschung 62 (2): 53–8. doi:10.1055/s-0031-1299685. PMID 22344548.
- ↑ Barbara G, Stanghellini V, Cremon C; et al. (2009). "Aminosalicylates and other anti-inflammatory compounds for irritable bowel syndrome". Dig Dis. 27 Suppl 1: 115–21. doi:10.1159/000268131. PMID 20203507.
- ↑ Philpott H, Nandurkar S, Lubel J, Gibson PR; Nandurkar; Lubel; Gibson (2012). "Alternative investigations for irritable bowel syndrome". Journal of Gastroenterology and Hepatology 28 (1): 73–77. doi:10.1111/j.1440-1746.2012.07291.x. PMID 23033865.
- ↑ "Serotonergic reinforcement of intestinal barrier function is impaired in irritable bowel syndrome.". Aliment Pharmacol Ther. 40: 392–402. Aug 2014. doi:10.1111/apt.12842. PMID 24943480.
- ↑ "Human leukocyte antigen DQ2/8 prevalence in non-celiac patients with gastrointestinal diseases.". World J Gastroenterol. 19: 2507–13. Apr 28, 2013. doi:10.3748/wjg.v19.i16.2507. PMID 23674852.
- ↑ Halpert AD, Thomas AC, Hu Y, Morris CB, Bangdiwala SI, Drossman DA; Thomas; Hu; Morris; Bangdiwala; Drossman (2006). "A survey on patient educational needs in irritable bowel syndrome and attitudes toward participation in clinical research". J Clin Gastroenterol 40 (1): 37–43. doi:10.1097/01.mcg.0000190759.95862.08. PMID 16340632.
External links
|