Hyperbaric medicine
| Hyperbaric medicine | |
|---|---|
| Intervention | |
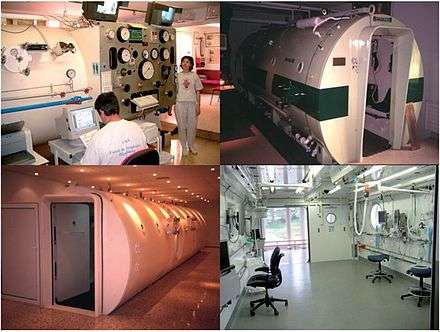
 A Sechrist Monoplace hyperbaric chamber at the Moose Jaw Union Hospital, Saskatchewan, Canada | |
| ICD-9-CM | 93.95 |
| MeSH | D006931 |
| OPS-301 code | 8-721 |
| MedlinePlus | 002375 |
Hyperbaric medicine, also known as hyperbaric oxygen therapy (HBOT), is the medical use of oxygen at a level higher than atmospheric pressure. The equipment required consists of a pressure chamber, which may be of rigid or flexible construction, and a means of delivering 100% oxygen. Operation is performed to a predetermined schedule by trained personnel who monitor the patient and may adjust the schedule as required. HBOT found early use in the treatment of decompression sickness, and has also shown great effectiveness in treating conditions such as gas gangrene and carbon monoxide poisoning. More recent research has examined the possibility that it may also have value for other conditions such as cerebral palsy and multiple sclerosis, but no significant evidence has been found.
Scope
Hyperbaric medicine includes:
- Hyperbaric oxygen treatment
- Therapeutic recompression
Medical uses
In the United States the Undersea and Hyperbaric Medical Society, known as UHMS, lists approvals for reimbursement for certain diagnoses in hospitals and clinics. The following indications are approved (for reimbursement) uses of hyperbaric oxygen therapy as defined by the UHMS Hyperbaric Oxygen Therapy Committee:[1][2]
- Air or gas embolism;[3]
- Carbon monoxide poisoning;[4][5]
- Central retinal artery occlusion;[9]
- Clostridal myositis and myonecrosis (gas gangrene);[10][11][12]
- Crush injury, compartment syndrome, and other acute traumatic ischemias;[13][14]
- Decompression sickness;[15][16][17]
- Enhancement of healing in selected problem wounds;[18][19][20]
- Diabetically derived illness, such as diabetic foot,[21][22] diabetic retinopathy,[23][24] diabetic nephropathy;[25]
- Exceptional blood loss (anemia);[26][27]
- Idiopathic sudden sensorineural hearing loss;[28]
- Intracranial abscess;[29][30]
- Necrotizing soft tissue infections (necrotizing fasciitis);[31][32]
- Osteomyelitis (refractory);[33][34][35]
- Delayed radiation injury (soft tissue and bony necrosis);[36][37][38]
- Skin grafts and flaps (compromised);[39]
- Thermal burns.[40][41]
Evidence is insufficient as of 2013 to support its use in autism, cancer, diabetes, HIV/AIDS, Alzheimer's disease, asthma, Bell's palsy, cerebral palsy, depression, heart disease, migraines, multiple sclerosis, Parkinson's disease, spinal cord injury, sports injuries, or stroke.[42][43] Despite the lack of evidence, in 2015, the number people utilizing this therapy has continued to rise.[44]
Hearing issues
Recent studies have indicated that HBO therapy is recommended and warranted in those patients with idiopathic sudden deafness, acoustic trauma or noise-induced hearing loss within 3 months after onset of disorder.[45]
Chronic ulcers
HBOT in diabetic foot ulcers increased the rate of early ulcer healing but does not appear to provide any benefit in wound healing at long term follow-up. In particular, there was no difference in major amputation rate. For venous, arterial and pressure ulcers, no evidence was apparent that HBOT provides an improvement over standard treatment.[46]
Radiation injury
There is some evidence that HBOT is effective for late radiation tissue injury of bone and soft tissues of the head and neck. Some people with radiation injuries of the head, neck or bowel show an improvement in quality of life. Importantly, no such effect has been found in neurological tissues. The use of HBOT may be justified to selected patients and tissues, but further research is required to establish the best people to treat and timing of any HBO therapy.[47]
Neuro-rehabilitation
There is tentative evidence for HBOT in traumatic brain injury.[48] As of 2012 there is insufficient evidence to support its general use in TBI.[48] In stroke HBOT does not show benefit.[49][50] HBOT in multiple sclerosis has not shown benefit and routine use is not recommended.[43][51]
A 2007 review of HBOT in cerebral palsy found no difference compared to the control group.[52][53] Neuropsychological tests also showed no difference between HBOT and room air and based on caregiver report, those who received room air had significantly better mobility and social functioning.[52][53] Children receiving HBOT were reported to experience seizures and the need for tympanostomy tubes to equalize ear pressure, though the incidence was not clear.[52]
Cancer
In alternative medicine, hyperbaric medicine has been promoted as a treatment for cancer, but there is no evidence it is effective for this purpose.[54]
Contraindications
The toxicology of the treatment has recently been reviewed by Ustundag et al.[55] and its risk management is discussed by Christian R. Mortensen, in light of the fact that most hyperbaric facilities are managed by departments of anaesthesiology and some of their patients are critically ill.[56]
The only absolute contraindication to hyperbaric oxygen therapy is untreated tension pneumothorax.[57] The reason is concern that it can progress to tension pneumothorax, especially during the decompression phase of therapy. The COPD patient with a large bleb represents a relative contraindication for similar reasons.[58] Also, the treatment may raise the issue of Occupational health and safety (OHS), which has been encountered by the therapist.[59]
Patients should not undergo HBO therapy if they are taking or have recently taken the following drugs:
- Doxorubicin (Adriamycin) – A chemotherapeutic drug. This drug has been shown to potentiate cytotoxicity during HBO therapy.
- Cisplatin – Also a chemotherapeutic drug.
- Disulfiram (Antabuse) – Used in the treatment of alcoholism.
- Mafenide acetate (Sulfamylon) – Suppresses bacterial infections in burn wounds
The following are relative contraindications -- meaning that special consideration must be made by specialist physicians before HBO treatments begin:
- Cardiac disease
- COPD with air trapping - can lead to pneumothorax during treatment.
- Upper respiratory infections – These conditions can make it difficult for the patient to equalise their ears or sinuses, which can result in what is termed ear or sinus squeeze.
- High fevers – In most cases the fever should be lowered before HBO treatment begins.
- Emphysema with CO2 retention – This condition can lead to pneumothorax during HBO treatment.
- History of thoracic (chest) surgery – This is rarely a problem and usually not considered a contraindication. However, there is concern that air may be trapped in lesions that were created by surgical scarring. These conditions need to be evaluated prior to considering HBO therapy.
- Malignant disease: Cancers thrive in blood-rich environments but may be suppressed by high oxygen levels. HBO treatment of individuals who have cancer presents a problem, since HBO both increases blood flow via angiogenesis and also raises oxygen levels. Taking an anti-angiogenic supplement may provide a solution.[60][61] A study by Feldemier, et al. and recent NIH funded study on Stem Cells by Thom, et al., indicate that HBO is actually beneficial in producing stem/progenitor cells and the malignant process is not accelerated.[62]
- Middle ear barotrauma is always a consideration in treating both children and adults in a hyperbaric environment because of the necessity to equalise pressure in the ears.
Pregnancy is not a relative contraindication to hyperbaric oxygen treatments,[58] although it may be for SCUBA diving. In cases where a pregnant woman has carbon monoxide poisoning there is evidence that lower pressure (2.0 ATA) HBOT treatments are not harmful to the fetus, and that the risk involved is outweighed by the greater risk of the untreated effects of CO on the fetus (neurologic abnormalities or death.)[63][64] In pregnant patients, HBO therapy has been shown to be safe for the fetus when given at appropriate levels and “doses” (durations). In fact, pregnancy lowers the threshold for HBO treatment of carbon monoxide-exposed pregnant patients. This is due to the high affinity of fetal hemoglobin for CO.[58]
Therapeutic principles
Several therapeutic principles are made use of in HBOT:[1]
- The increased overall pressure is of therapeutic value when HBOT is used in the treatment of decompression sickness and air embolism as it provides a physical means of reducing the volume of inert gas bubbles within the body;[65]
- For many other conditions, the therapeutic principle of HBOT lies in its ability to drastically increase partial pressure of oxygen in the tissues of the body. The oxygen partial pressures achievable using HBOT are much higher than those achievable while breathing pure oxygen at normobaric conditions (i.e. at normal atmospheric pressure);
- A related effect is the increased oxygen transport capacity of the blood. Under normal atmospheric pressure, oxygen transport is limited by the oxygen binding capacity of hemoglobin in red blood cells and very little oxygen is transported by blood plasma. Because the hemoglobin of the red blood cells is almost saturated with oxygen under atmospheric pressure, this route of transport cannot be exploited any further. Oxygen transport by plasma, however is significantly increased using HBOT as the stimulus.
- Recent evidence notes that exposure to hyperbaric oxygen (HBOT) mobilizes stem/progenitor cells from the bone marrow by a nitric oxide (NO) -dependent mechanism.[66] This mechanism may account for the patient cases that suggest recovery of damaged organs and tissues with HBOT.
Hyperbaric chambers
Construction
The traditional type of hyperbaric chamber used for HBOT is a hard shelled pressure vessel. Such chambers can be run at absolute pressures as much as 6 bars (87 psi), 600,000 Pa. Navies, diving organizations, hospitals, and dedicated recompression facilities typically operate these. They range in size from semi-portable, one-patient units to room-sized units that can treat eight or more patients. Recent advances in materials technology have resulted in the manufacture of portable, "soft" chambers that can operate at between 0.3 and 0.5 bars (4.4 and 7.3 psi) above atmospheric pressure.[67] Hard chambers and soft chambers should not be considered equivalent in regards to efficacy and safety as they are different in many aspects.
A hard chamber may consist of
- a pressure vessel that is generally made of steel, aluminium with the view ports (windows) made of acrylic;
- one or more human entry hatches—small and circular or wheel-in type hatches for patients on gurneys;
- the airlock that allows human entry—a separate chamber with two hatches, one to the outside and one to the main chamber, which can be independently pressurized to allow patients to enter or exit the main chamber while it is still pressurized and a small airlock for medicines, instruments, and food;
- glass ports or closed-circuit television that allows technicians and medical staff outside the chamber to monitor the patient inside the chamber;
- an intercom or walkie-talkie allowing two-way communication;
- a carbon dioxide scrubber—consisting of a fan that passes the gas inside the chamber through a soda lime canister;
- a control panel outside the chamber to open and close valves that control air flow to and from the chamber, and regulate oxygen to helmets or masks.
A soft chamber may consist of
- a urethane-coated, nylon-bonded flexible acrylic pressure vessel with steel-weld technology;
- a full-length dual zipper-sealed opening;
- an over-pressure valve, if oxygen is fed into a small mask and expired gas has to be circulated toward the end of the chamber and out through the pressure regulators.
Oxygen supply

In today's larger multiplace chambers, both patients and medical staff inside the chamber breathe from either "oxygen hoods" – flexible, transparent soft plastic hoods with a seal around the neck similar to a space suit helmet – or tightly fitting oxygen masks, which supply pure oxygen and may be designed to directly exhaust the exhaled gas from the chamber. During treatment patients breathe 100% oxygen most of the time to maximise the effectiveness of their treatment, but have periodic "air breaks" during which they breathe room air (21% oxygen) to minimize the risk of oxygen toxicity. The exhaled gas must be removed from the chamber to prevent the buildup of oxygen, which could present a fire risk. Attendants may also breathe oxygen to reduce their risk of decompression sickness. The pressure inside a hard chamber is increased by opening valves allowing high-pressure air to enter from storage cylinders, which are filled by an air compressor. A soft chamber may be pressurised directly from a compressor.
Smaller "monoplace" chambers can only accommodate the patient, and no medical staff can enter. The chamber may be pressurised with pure oxygen or compressed air. If pure oxygen is used, no oxygen breathing mask or helmet is needed, but the cost of using pure oxygen is much higher than that of using compressed air. If compressed air is used, then an oxygen mask or hood is needed as in a multiplace hard chamber. In monoplace chambers that are compressed with pure oxygen, a mask is needed to provide the patient with "air breaks", or periods of breathing normal air (21% oxygen). This is in order to reduce the risk of hyperoxic seizures. In soft chambers, using compressed air and a mask supplying 96% oxygen, no air breaks are necessary, because the risk of oxygen toxicity is negligible because of the lower oxygen partial pressures used (usually 1.3 ATA), and short durations of treatment.
Treatments
Initially, HBOT was developed as a treatment for diving disorders involving bubbles of gas in the tissues, such as decompression sickness and gas embolism. The chamber cures decompression sickness and gas embolism by increasing pressure, reducing the size of the gas bubbles and improving the transport of blood to downstream tissues. The high concentrations of oxygen in the tissues are beneficial in keeping oxygen-starved tissues alive, and have the effect of removing the nitrogen from the bubble, making it smaller until it consists only of oxygen, which is re-absorbed into the body. After elimination of bubbles, the pressure is gradually reduced back to atmospheric levels. Hyperbaric chambers are also used for animals, especially race horses where a recovery is worth a great deal to their owners. It is also used to treat dogs and cats in pre- and post-surgery treatment to strengthen their systems prior to surgery and then accelerate healing post surgery.
Protocol
The slang term, at some facilities, for a cycle of pressurization inside the HBOT chamber is "a dive". An HBOT treatment for longer-term conditions is often a series of 20 to 40 dives, or compressions. These dives last for about an hour and can be administered via a hard, high-pressure chamber or a soft, low-pressure chamber—the major difference being per-dive "dose" of oxygen. Many conditions do quite well with the lower dose, lower cost-per-hour, soft chambers.
Emergency HBOT for decompression illness follows treatment schedules laid out in treatment tables. Most cases employ a recompression to 2.8 bars (41 psi) absolute, the equivalent of 18 metres (60 ft) of water, for 4.5 to 5.5 hours with the casualty breathing pure oxygen, but taking air breaks every 20 minutes to reduce oxygen toxicity. For extremely serious cases resulting from very deep dives, the treatment may require a chamber capable of a maximum pressure of 8 bars (120 psi), the equivalent of 70 metres (230 ft) of water, and the ability to supply heliox as a breathing gas.[68]
U.S. Navy treatment charts are used in Canada and the United States to determine the duration, pressure, and breathing gas of the therapy. The most frequently used tables are Table 5 and Table 6. In the UK the Royal Navy 62 and 67 tables are used.
The Undersea and Hyperbaric Medical Society (UHMS) publishes a report that compiles the latest research findings and contains information regarding the recommended duration and pressure of the longer-term conditions.[69]
Home and out-patient clinic treatment

There are several sizes of portable chambers, which are used for home treatment. These are usually referred to as "mild personal hyperbaric chambers", which is a reference to the lower pressure (compared to hard chambers) of soft-sided chambers. Food and Drug Administration (FDA) approved chambers for use with room air are available in the USA and may go up to 4.4 pounds per square inch (psi) above atmospheric pressure, which equals 1.3 atmospheres absolute (ATA), equivalent to a depth of 10 feet of sea water. In the US, these "mild personal hyperbaric chambers" are categorized by the FDA as CLASS II medical devices and requires a prescription in order to purchase one or take treatments.[70] Personal hyperbaric chambers are only FDA approved to reach 1.3 ATA. While hyperbaric chamber distributors and manufacturers cannot supply a chamber in the US with any form of elevated oxygen delivery system, a physician can write a prescription to combine the two modalities, as long as there is a prescription for both hyperbarics and oxygen. The most common option (but not approved by FDA) some patients choose is to acquire an oxygen concentrator which typically delivers 85–96% oxygen as the breathing gas. Because of the high circulation of air through the chamber, the total concentration of oxygen in the chamber never exceeds 25% as this can increase the risk of fire. Oxygen is never fed directly into soft chambers but is rather introduced via a line and mask directly to the patient. FDA approved oxygen concentrators for human consumption in confined areas used for HBOT are regularly monitored for purity (+/- 1%) and flow (10 to 15 liters per minute outflow pressure). An audible alarm will sound if the purity ever drops below 80%. Personal hyperbaric chambers use 120 volt or 220 volt outlets. Ranging in size from 21 inches up to 40 inches in diameter these chambers measure between 84 in (7 ft) to 120 in (10 ft) in length. The soft chambers are approved by the FDA for the treatment of altitude sickness, but are commonly used for other "off-label" purposes.
Possible complications and concerns
There are risks associated with HBOT, similar to some diving disorders. Pressure changes can cause a "squeeze" or barotrauma in the tissues surrounding trapped air inside the body, such as the lungs,[57] behind the eardrum,[71][72] inside paranasal sinuses,[71] or trapped underneath dental fillings.[73] Breathing high-pressure oxygen may cause oxygen toxicity.[74] Temporarily blurred vision can be caused by swelling of the lens, which usually resolves in two to four weeks.[75][76]
There are reports that cataract may progress following HBOT.[77] Also a rare side effect has been blindness secondary to optic neuritis (inflammation of the optic nerve).
Effects of pressure
Patients inside the chamber may notice discomfort inside their ears as a pressure difference develops between their middle ear and the chamber atmosphere.[78] This can be relieved by the Valsalva maneuver or by "jaw wiggling". As the pressure increases further, mist may form in the air inside the chamber and the air may become warm. Increased pressure may also cause ear drums to rupture, resulting in severe pain.
To reduce the pressure, a valve is opened to allow air out of the chamber. As the pressure falls, the patient’s ears may "squeak" as the pressure inside the ear equalizes with the chamber. The temperature in the chamber will fall. The speed of pressurization and de-pressurization can be adjusted to each patient's needs.
Costs
HBOT is recognized by Medicare in the United States as a reimbursable treatment for 14 UHMS "approved" conditions. A 1-hour HBOT session may cost between $165 and $250 in private clinics, and over $2,000 in hospitals. U.S. physicians (either M.D., D.C. or D.O.) may lawfully prescribe HBOT for "off-label" conditions such as stroke,[79][80][81] and migraine.[82][83][84] Such patients are treated in outpatient clinics. In the United Kingdom most chambers are financed by the National Health Service, although some, such as those run by Multiple Sclerosis Therapy Centres, are non-profit. In Australia, HBOT is not covered by Medicare as a treatment for multiple sclerosis.[85] The average U.S. hospital charge is $1,800.00 per 90 minute HBOT treatment. China and Russia treat more than 80 maladies, conditions and trauma with HBOT.[86]
Research
Aspects under research include:
- Radiation-induced hemorrhagic cystitis;[87]
- Inflammatory bowel disease.[88]
Neurological
Tentative evidence shows a possible benefit in cerebrovascular diseases.[89] The clinical experience and results so far published has promoted the use of HBO therapy in patients with cerebrovascular injury and focal cerebrovascular injuries.[89][90] However, the power of clinical research is limited because of the shortage of randomized controlled trials.
Radiation wounds
Many studies indicate a positive share of HBOT after radiation injury, and HBOT is prescribed for treating chronic wounds associated with radiation exposure. However, no significant evidence was found on HBOT having either a positive or negative effect on radiation wounds. This might be explained due to the lack of experimental and clinical studies.[91]
History
Hyperbaric air
The use of air at raised ambient pressure for the treatment of illness is recorded from 1662 for afflictions of the lung, by Henshaw. It is unlikely to have had any significant effect.
Junod built a chamber in France in 1834 to treat pulmonary conditions at pressures between 2 and 4 atmospheres absolute.
During the following century “pneumatic centres” were established in Europe and the USA which used hyperbaric air to treat a variety of conditions.[92]
Orval J Cunningham, a professor of anaesthesia at the University of Kansas in the early 1900s observed that people suffering from circulatory disorders did better at sea level than at altitude and this formed the basis for his use of hyperbaric air. In 1918 he successfully treated patients suffering from the Spanish flu with hyperbaric air. In 1930 the American Medical Association forced him to stop such hyperbaric treatment, since he did not provide acceptable evidence that the treatments were effective.[92]
Hyperbaric oxygen
The English scientist, Joseph Priestley discovered oxygen in 1775. Shortly after its discovery, there were reports of toxic effects of hyperbaric oxygen on the central nervous system and lungs, which delayed therapeutic applications until 1937, when Behnke and Shaw first used it in the treatment of decompression sickness.[92]
In 1955 and 1956 Churchill-Davidson, in the UK, used hyperbaric oxygen to enhance the radiosensitivity of tumours, while Ite Boerema, at the University of Amsterdam, successfully used it in cardiac surgery.[92]
In 1961 WH Brummelkamp et al. published on the use of hyperbaric oxygen in the treatment of clostridial gas gangrene.
In 1962 Smith and Sharp reported successful treatment of carbon monoxide poisoning with hyperbaric oxygen.
The Undersea Medical Society (now Undersea and Hyperbaric Medical Society) formed a Committee on Hyperbaric Oxygenation which has become recognized as the authority on indications for hyperbaric oxygen treatment.[92]
See also
- Undersea and Hyperbaric Medical Society
- South Pacific Underwater Medicine Society
- Decompression chamber
- Hyperbaric treatment schedules
References
- 1 2 Gesell, Laurie B. (Chair and editor) (2008). Hyperbaric Oxygen Therapy Indications. The Hyperbaric Oxygen Therapy Committee Report (12 ed.). Durham, NC: Undersea and Hyperbaric Medical Society. ISBN 0-930406-23-0.
- ↑ "Indications for hyperbaric oxygen therapy". Undersea & Hyperbaric Medical Society. 2011. Retrieved 21 August 2011.
- ↑ Undersea and Hyperbaric Medical Society. "Air or Gas Embolism". Retrieved 2011-08-21.
- ↑ Undersea and Hyperbaric Medical Society. "Carbon Monoxide". Retrieved 2011-08-21.
- ↑ Piantadosi CA (2004). "Carbon monoxide poisoning". Undersea & Hyperbaric Medicine 31 (1): 167–77. PMID 15233173.
- ↑ Undersea and Hyperbaric Medical Society. "Cyanide Poisoning". Retrieved 2011-08-21.
- ↑ Hall AH, Rumack BH (Sep 1986). "Clinical toxicology of cyanide". Annals of Emergency Medicine 15 (9): 1067–1074. doi:10.1016/S0196-0644(86)80131-7. PMID 3526995.
- ↑ Takano T, Miyazaki Y, Nashimoto I, Kobayashi K (Sep 1980). "Effect of hyperbaric oxygen on cyanide intoxication: in situ changes in intracellular oxidation reduction". Undersea Biomedical Research 7 (3): 191–7. PMID 7423657.
- ↑ Undersea and Hyperbaric Medical Society. "Central Retinal Artery Occlusion". Retrieved 2014-05-30.
- ↑ Undersea and Hyperbaric Medical Society. "Clostridal Myositis and Myonecrosis (Gas gangrene)". Retrieved 2011-08-21.
- ↑ Hart GB, Strauss MB (1990). "Gas Gangrene - Clostridial Myonecrosis: A Review". J. Hyperbaric Med 5 (2): 125–144.
- ↑ Zamboni WA, Riseman JA, Kucan JO (1990). "Management of Fournier's Gangrene and the role of Hyperbaric Oxygen". J. Hyperbaric Med 5 (3): 177–186.
- ↑ Undersea and Hyperbaric Medical Society. "Crush Injury, Compartment syndrome, and other Acute Traumatic Ischemias". Retrieved 2011-08-21.
- ↑ Bouachour G, Cronier P, Gouello JP, Toulemonde JL, Talha A, Alquier P (Aug 1996). "Hyperbaric oxygen therapy in the management of crush injuries: a randomized double-blind placebo-controlled clinical trial". The Journal of Trauma 41 (2): 333–9. doi:10.1097/00005373-199608000-00023. PMID 8760546.
- ↑ Undersea and Hyperbaric Medical Society. "Decompression Sickness or Illness and Arterial Gas Embolism". Retrieved 2011-08-21.
- ↑ Brubakk, A. O.; T. S. Neuman (2003). Bennett and Elliott's physiology and medicine of diving, 5th Rev ed. United States: Saunders Ltd. p. 800. ISBN 0-7020-2571-2.
- ↑ Acott, C. (1999). "A brief history of diving and decompression illness". South Pacific Underwater Medicine Society Journal 29 (2). ISSN 0813-1988. OCLC 16986801. Retrieved 2008-03-18.
- ↑ Undersea and Hyperbaric Medical Society. "Enhancement of Healing in Selected Problem Wounds". Retrieved 2011-08-21.
- ↑ Zamboni WA, Wong HP, Stephenson LL, Pfeifer MA (Sep 1997). "Evaluation of hyperbaric oxygen for diabetic wounds: a prospective study". Undersea & Hyperbaric Medicine 24 (3): 175–9. PMID 9308140.
- ↑ Kranke P, Bennett M, Roeckl-Wiedmann I, Debus S (2004). Kranke, Peter, ed. "Hyperbaric oxygen therapy for chronic wounds". The Cochrane Database of Systematic Reviews (2): CD004123. doi:10.1002/14651858.CD004123.pub2. PMID 15106239.
- ↑ Abidia A, Laden G, Kuhan G, Johnson BF, Wilkinson AR, Renwick PM, Masson EA, McCollum PT (Jun 2003). "The role of hyperbaric oxygen therapy in ischaemic diabetic lower extremity ulcers: a double-blind randomised-controlled trial". European Journal of Vascular and Endovascular Surgery 25 (6): 513–518. doi:10.1053/ejvs.2002.1911. PMID 12787692.
- ↑ Kalani M, Jörneskog G, Naderi N, Lind F, Brismar K (2002). "Hyperbaric oxygen (HBO) therapy in treatment of diabetic foot ulcers. Long-term follow-up". Journal of Diabetes and its Complications 16 (2): 153–158. doi:10.1016/S1056-8727(01)00182-9. PMID 12039398.
- ↑ Chen, J (2003). "The Effects of Hyperbaric Oxygen Therapy on Diabetic Retinopathy". Investigative Ophthalmology & Visual Science 44 (5): 4017–B720.
- ↑ Chang YH, Chen PL, Tai MC, Chen CH, Lu DW, Chen JT (Aug 2006). "Hyperbaric oxygen therapy ameliorates the blood-retinal barrier breakdown in diabetic retinopathy". Clinical & Experimental Ophthalmology 34 (6): 584–589. doi:10.1111/j.1442-9071.2006.01280.x. PMID 16925707.
- ↑ Basile C, Montanaro A, Masi M, Pati G, De Maio P, Gismondi A (2002). "Hyperbaric oxygen therapy for calcific uremic arteriolopathy: a case series". Journal of Nephrology 15 (6): 676–80. PMID 12495283.
- ↑ Undersea and Hyperbaric Medical Society. "Severe Anemia".
- ↑ Hart GB, Lennon PA, Strauss MB. (1987). "Hyperbaric oxygen in exceptional acute blood-loss anemia". J. Hyperbaric Med 2 (4): 205–210. Retrieved 2008-05-19.
- ↑ Undersea and Hyperbaric Medical Society. "Idiopathic Sudden Sensorineural Hearing Loss". Retrieved 2014-05-30.
- ↑ Undersea and Hyperbaric Medical Society. "Intracranial Abscess". Retrieved 2011-08-21.
- ↑ Lampl LA, Frey G, Dietze T, Trauschel M. (1989). "Hyperbaric Oxygen in Intracranial Abscesses". J. Hyperbaric Med 4 (3): 111–126. Retrieved 2008-05-19.
- ↑ Undersea and Hyperbaric Medical Society. "Necrotizing Soft Tissue Infections". Retrieved 2011-08-21.
- ↑ Escobar SJ, Slade JB, Hunt TK, Cianci P (2005). "Adjuvant hyperbaric oxygen therapy (HBO2)for treatment of necrotizing fasciitis reduces mortality and amputation rate". Undersea & Hyperbaric Medicine 32 (6): 437–43. PMID 16509286.
- ↑ Undersea and Hyperbaric Medical Society. "Refractory Osteomyelitis". Retrieved 2011-08-21.
- ↑ Mader JT, Adams KR, Sutton TE (1987). "Infectious diseases: pathophysiology and mechanisms of hyperbaric oxygen". J. Hyperbaric Med 2 (3): 133–140. Retrieved 2008-05-16.
- ↑ Kawashima M, Tamura H, Nagayoshi I, Takao K, Yoshida K, Yamaguchi T (2004). "Hyperbaric oxygen therapy in orthopedic conditions". Undersea & Hyperbaric Medicine 31 (1): 155–62. PMID 15233171.
- ↑ Undersea and Hyperbaric Medical Society. "Hyperbaric Oxygen Treatments for Complications of radiation Therapy". Retrieved 2011-08-21.
- ↑ Zhang LD, Kang JF, Xue HL (Jul 1990). "Distribution of lesions in the head and neck of the humerus and the femur in dysbaric osteonecrosis". Undersea Biomedical Research 17 (4): 353–8. OCLC 2068005. PMID 2396333.
- ↑ Lafforgue P (Oct 2006). "Pathophysiology and natural history of avascular necrosis of bone". Joint, Bone, Spine : Revue du Rhumatisme 73 (5): 500–7. doi:10.1016/j.jbspin.2006.01.025. PMID 16931094.
- ↑ Undersea and Hyperbaric Medical Society. "Skin Grafts and Flaps Compromised". Retrieved 2011-08-21.
- ↑ Undersea and Hyperbaric Medical Society. "Thermal Burns". Retrieved 2011-08-21.
- ↑ Cianci P, Lueders H, Lee H, Shapiro R, Sexton J, Williams C, Green B (1988). "Adjunctive Hyperbaric Oxygen Reduces the Need for Surgery in 40–80% Burns". J. Hyperbaric Med 3 (2): 97–101. Retrieved 2008-05-16.
- ↑ "Hyperbaric Oxygen Therapy: Don't Be Misled". Food and Drug Administration. August 22, 2013.
- 1 2 Bennett M, Heard R (2004). Bennett, Michael H, ed. "Hyperbaric oxygen therapy for multiple sclerosis". The Cochrane Database of Systematic Reviews (1): CD003057. doi:10.1002/14651858.CD003057.pub2. PMID 14974004.
- ↑ Walker, Joseph. "Hyperbaric Oxygen Therapy Gets More Popular as Unapproved Treatment". Wall Street Journal. Retrieved 2015-03-14.
- ↑ Lamm K, Lamm H, Arnold W (1998). "Effect of hyperbaric oxygen therapy in comparison to conventional or placebo therapy or no treatment in idiopathic sudden hearing loss, acoustic trauma, noise-induced hearing loss and tinnitus. A literature survey". Advances in Oto-rhino-laryngology 54: 86–99. doi:10.1159/000059055. ISBN 3-8055-6541-0. PMID 9547879.
- ↑ Kranke P, Bennett MH, Martyn-St James M, Schnabel A, Debus SE (Apr 2012). "Hyperbaric oxygen therapy for chronic wounds". The Cochrane Database of Systematic Reviews 4 (4): CD004123. doi:10.1002/14651858.CD004123.pub3. PMID 22513920.
- ↑ Bennett MH, Feldmeier J, Hampson N, Smee R, Milross C (2012). "Hyperbaric oxygen therapy for late radiation tissue injury". The Cochrane Database of Systematic Reviews 5 (5): CD005005. doi:10.1002/14651858.CD005005.pub3. PMID 22592699.
- 1 2 Bennett, MH; Trytko, B; Jonker, B (12 December 2012). "Hyperbaric oxygen therapy for the adjunctive treatment of traumatic brain injury.". The Cochrane database of systematic reviews 12: CD004609. doi:10.1002/14651858.CD004609.pub3. PMID 23235612.
- ↑ Carson S, McDonagh M, Russman B, Helfand M (Dec 2005). "Hyperbaric oxygen therapy for stroke: a systematic review of the evidence". Clinical rehabilitation 19 (8): 819–33. doi:10.1191/0269215505cr907oa. PMID 16323381.
- ↑ Bennett, MH; Weibel, S; Wasiak, J; Schnabel, A; French, C; Kranke, P (12 November 2014). "Hyperbaric oxygen therapy for acute ischaemic stroke.". The Cochrane database of systematic reviews 11: CD004954. doi:10.1002/14651858.CD004954.pub3. PMID 25387992.
- ↑ Bennett M, Heard R (Apr 2010). "Hyperbaric oxygen therapy for multiple sclerosis". CNS neuroscience & therapeutics 16 (2): 115–24. doi:10.1111/j.1755-5949.2009.00129.x. PMID 20415839.
- 1 2 3 McDonagh MS, Morgan D, Carson S, Russman BS (Dec 2007). "Systematic review of hyperbaric oxygen therapy for cerebral palsy: the state of the evidence". Developmental Medicine and Child Neurology 49 (12): 942–7. doi:10.1111/j.1469-8749.2007.00942.x. PMID 18039243.
- 1 2 Collet JP, Vanasse M, Marois P, Amar M, Goldberg J, Lambert J, Lassonde M, Hardy P, Fortin J, Tremblay SD, Montgomery D, Lacroix J, Robinson A, Majnemer A (Feb 2001). "Hyperbaric oxygen for children with cerebral palsy: a randomised multicentre trial. HBO-CP Research Group". Lancet 357 (9256): 582–6. doi:10.1016/S0140-6736(00)04054-X. PMID 11558483.
- ↑ "Hyperbaric Oxygen Therapy". American Cancer Society. 14 April 2011. Retrieved February 2015.
- ↑ Ustundag A, Duydu Y, Aydin A, Eken A, Dundar K, Uzun G (Oct 2008). "Evaluation of the potential genotoxic effects of hyperbaric oxygen therapy". Toxicology Letters 180: S142. doi:10.1016/j.toxlet.2008.06.792.
- ↑ Mortensen, Christian Risby (2008). "Hyperbaric oxygen therapy". Current Anaesthesia & Critical Care (Elsevier) 19 (5–6): 333–337. doi:10.1016/j.cacc.2008.07.007.
- 1 2 Broome JR, Smith DJ (Nov 1992). "Pneumothorax as a complication of recompression therapy for cerebral arterial gas embolism". Undersea biomedical research 19 (6): 447–55. PMID 1304671.
- 1 2 3 Marx, JA, ed. (2002). "chapter 194". Rosen’s Emergency Medicine: Concepts and Clinical Practice (5th ed.). Mosby. ISBN 978-0323011853.
- ↑ CAMJ (2008). "Fracture of the maxillary bone during hyperbaric oxygen therapy". Retrieved 17 December 2008.
- ↑ Takenaka S, Arimura T, Higashi M, Nagayama T, Ito E (Aug 1980). "Experimental study of bleomycin therapy in combination with hyperbaric oxygenation". Nihon Gan Chiryo Gakkai shi 15 (5): 864–75. PMID 6159432.
- ↑ Stubbs JM, Johnson EG, Thom SR (2005). "Trends Of Treating Patients, That Have Received Bleomycin Therapy In The Past, With Hyperbaric Oxygen Treatment (Hbot) And A Survey Of Considered Absolute Contraindications To Hbot". Undersea Hyperb Med abstract 32 (supplement). Retrieved 2008-05-23.
- ↑ Feldmeier J, Carl U, Hartmann K, Sminia P (Spring 2003). "Hyperbaric oxygen: does it promote growth or recurrence of malignancy?". Undersea & Hyperbaric Medicine 30 (1): 1–18. PMID 12841604.
- ↑ Van Hoesen KB, Camporesi EM, Moon RE, Hage ML, Piantadosi CA (Feb 1989). "Should hyperbaric oxygen be used to treat the pregnant patient for acute carbon monoxide poisoning? A case report and literature review". JAMA 261 (7): 1039–43. doi:10.1001/jama.1989.03420070089037. PMID 2644457.
- ↑ Elkharrat D, Raphael JC, Korach JM, Jars-Guincestre MC, Chastang C, Harboun C, Gajdos P (1991). "Acute carbon monoxide intoxication and hyperbaric oxygen in pregnancy". Intensive Care Medicine 17 (5): 289–92. doi:10.1007/BF01713940. PMID 1939875.
- ↑ Jørgensen TB, Sørensen AM, Jansen EC (Apr 2008). "Iatrogenic systemic air embolism treated with hyperbaric oxygen therapy". Acta Anaesthesiologica Scandinavica 52 (4): 566–568. doi:10.1111/j.1399-6576.2008.01598.x. PMID 18339163.
- ↑ Thom SR, Bhopale VM, Velazquez OC, Goldstein LJ, Thom LH, Buerk DG (Apr 2006). "Stem cell mobilization by hyperbaric oxygen". American Journal of Physiology. Heart and Circulatory Physiology 290 (4): H1378–H1386. doi:10.1152/ajpheart.00888.2005. PMID 16299259.
- ↑ www.oxyhealth.com. "Portable Hyperbaric Chambers | Hyperbaric Oxygen Chamber | Hyperbaric Oxygen". Oxyhealth.com. Retrieved 2010-09-25.
- ↑ U.S. Navy Supervisor of Diving (Apr 2008). "20". U.S. Navy Diving Manual (PDF). SS521-AG-PRO-010, revision 6 5. U.S. Naval Sea Systems Command. pp. 37–49. Archived (PDF) from the original on March 30, 2014. Retrieved 2009-06-29.
- ↑ "Undersea and Hyperbaric Medical Society". Uhms.org. Retrieved 2011-08-21.
- ↑ "Product Classification, Chamber, Hyperbaric". United States Food and Drug Administration. Retrieved 2011-08-22.
- 1 2 Fitzpatrick DT, Franck BA, Mason KT, Shannon SG (1999). "Risk factors for symptomatic otic and sinus barotrauma in a multiplace hyperbaric chamber". Undersea & Hyperbaric Medicine 26 (4): 243–7. PMID 10642071.
- ↑ Fiesseler FW, Silverman ME, Riggs RL, Szucs PA (2006). "Indication for hyperbaric oxygen treatment as a predictor of tympanostomy tube placement". Undersea & Hyperbaric Medicine 33 (4): 231–5. PMID 17004409.
- ↑ Stein, L (2000). "Dental Distress. The 'Diving Dentist' Addresses the Problem of a Diving-Related Toothache" (PDF). Alert Diver (January/ February): 45–48. Retrieved 2008-05-23.
- ↑ Smerz RW (2004). "Incidence of oxygen toxicity during the treatment of dysbarism". Undersea & Hyperbaric Medicine 31 (2): 199–202. PMID 15485081.
- ↑ Butler FK (1995). "Diving and hyperbaric ophthalmology". Survey of Ophthalmology 39 (5): 347–366. doi:10.1016/S0039-6257(05)80091-8. PMID 7604359.
- ↑ Butler FK, White E, Twa M (1999). "Hyperoxic myopia in a closed-circuit mixed-gas scuba diver". Undersea & Hyperbaric Medicine 26 (1): 41–5. PMID 10353183.
- ↑ Gesell LB, Adams BS, and Kob DG (2000). "De Novo Cataract Development Following A Standard Course Of Hyperbaric Oxygen Therapy". Undersea Hyperb Med abstract 27 (supplement). Retrieved 2008-06-01.
- ↑ Lehm Jan P, Bennett Michael H (2003). "Predictors of middle ear barotrauma associated with hyperbaric oxygen therapy". South Pacific Underwater Medicine Society Journal 33: 127–133. Retrieved 2009-07-15.
- ↑ Bennett MH, Wasiak J, Schnabel A, Kranke P, French C (2005). Bennett, Michael H, ed. "Hyperbaric oxygen therapy for acute ischaemic stroke". The Cochrane Database of Systematic Reviews (3): CD004954. doi:10.1002/14651858.CD004954.pub2. PMID 16034959.
- ↑ Jain KK (1989). "Effect of Hyperbaric Oxygenation on Spasticity in Stroke Patients". J. Hyperbaric Med 4 (2): 55–61. Retrieved 2008-08-06.
- ↑ Singhal AB, Lo EH (Feb 2008). "Advances in emerging nondrug therapies for acute stroke 2007". Stroke: A Journal of Cerebral Circulation 39 (2): 289–291. doi:10.1161/STROKEAHA.107.511485. PMID 18187678.
- ↑ Bennett MH, French C, Schnabel A, Wasiak J, Kranke P (2008). Bennett, Michael H, ed. "Normobaric and hyperbaric oxygen therapy for migraine and cluster headache". The Cochrane Database of Systematic Reviews (3): CD005219. doi:10.1002/14651858.CD005219.pub2. PMID 18646121.
- ↑ Eftedal OS, Lydersen S, Helde G, White L, Brubakk AO, Stovner LJ (Aug 2004). "A randomized, double blind study of the prophylactic effect of hyperbaric oxygen therapy on migraine". Cephalalgia: An International Journal of Headache 24 (8): 639–644. doi:10.1111/j.1468-2982.2004.00724.x. PMID 15265052.
- ↑ Fife WP, Fife CE (1989). "Treatment of Migraine with Hyperbaric Oxygen". J. Hyperbaric Med 4 (1): 7–15. Retrieved 2008-08-06.
- ↑ IN-DEEP. "Hyperbaric Oxygen Therapy for MS". Making Sense of MS Research. Retrieved 8 November 2012.
- ↑ Textbook of Hyperbaric Medicine KK Jane, 5th Edition, 2010
- ↑ Yoshida T, Kawashima A, Ujike T, Uemura M, Nishimura K, Miyoshi S (Jul 2008). "Hyperbaric oxygen therapy for radiation-induced hemorrhagic cystitis". International Journal of Urology: Official Journal of the Japanese Urological Association 15 (7): 639–641. doi:10.1111/j.1442-2042.2008.02053.x. PMID 18643783.
- ↑ Noyer CM, Brandt LJ (Feb 1999). "Hyperbaric oxygen therapy for perineal Crohn's disease". The American Journal of Gastroenterology 94 (2): 318–321. doi:10.1111/j.1572-0241.1999.00848.x. PMID 10022622. Check date values in:
|year= / |date= mismatch(help) - 1 2 Fischer BR, Palkovic S, Holling M, Wölfer J, Wassmann H (Jan 2010). "Rationale of hyperbaric oxygenation in cerebral vascular insult". Current Vascular Pharmacology 8 (1): 35–43. doi:10.2174/157016110790226598. PMID 19485935.
- ↑ Michalski D, Härtig W, Schneider D, Hobohm C (Feb 2011). "Use of normobaric and hyperbaric oxygen in acute focal cerebral ischemia - a preclinical and clinical review". Acta Neurologica Scandinavica 123 (2): 85–97. doi:10.1111/j.1600-0404.2010.01363.x. PMID 20456243.
- ↑ Spiegelberg L, Djasim UM, van Neck HW, Wolvius EB, van der Wal KG (Aug 2010). "Hyperbaric oxygen therapy in the management of radiation-induced injury in the head and neck region: a review of the literature". Journal of Oral and Maxillofacial Surgery 68 (8): 1732–1739. doi:10.1016/j.joms.2010.02.040. PMID 20493616.
- 1 2 3 4 5 Sharkey, Sarah (April 2000). "Current indications for hyperbaric oxygen therapy". ADF Health (Joint Health Command, Australian Department of Defence) 1 (2). Retrieved 18 December 2013.
Further reading
- Kindwall, Eric P; Whelan, Harry T (2008). Hyperbaric Medicine Practice, 3rd Edition. Flagstaff, AZ: Best Publishing Company. ISBN 978-1-930536-49-4.
- Mathieu, Daniel (2006). Handbook on Hyperbaric Medicine. Berlin: Springer. ISBN 1-4020-4376-7.
- Neubauer, Richard A; Walker, Morton (1998). Hyperbaric Oxygen Therapy. Garden City Park, NY: Avery Publishing Group. ISBN 978-0-89529-759-4.
- Jain, KK; Baydin, SA (2004). Textbook of hyperbaric medicine. Cambridge, MA: Hogrefe & Huber. ISBN 0-88937-277-2.
- Harch, Paul G; McCullough, Virginia (2010). The Oxygen Revolution. Long Island City, NY: Hatherleigh Press. ISBN 1-57826-326-3.
External links
- Hyperbaric Oxygen Therapy from eMedicine
- Duke University Medical Center Archives contains collections of multiple individuals who worked with hyperbaric medicine

| |||||||||||||||||||||||||||||||||||||||||||||||||||||||

| |||||||||||||||||||||||||||||||||

| ||||||||||||||||||||||||||||||||||