Opioid overdose
| Opioid overdose | |
|---|---|
| Classification and external resources | |
| Specialty | emergency medicine |
| ICD-10 | F11.0, T40.0-T40.2 |
| ICD-9-CM | 305.5, 965.0 |
| eMedicine | emerg/330 |
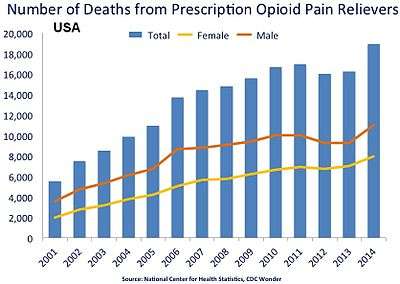
Opioid overdose is an acute condition due to excessive opioids. Examples of opioids are: morphine, heroin, tramadol, oxycodone, and methadone. It differs from opioid dependency. Although opioid overdose doesn't constitute a majority of the overdoses seen in the emergency department it is important to rule out in people given its potential for mortality and the ease of reversal.[1] Dependence on prescription opioids can stem from treatment of chronic pain and in recent years is the cause of the increased number of opioid overdoses.[2]
Initial treatment involves supporting the persons breathing and providing oxygen.[3] Naloxone is then recommended among those who are not breathing.[3]
Opioid use disorders resulted in 51,000 worldwide deaths in 2013 up from 18,000 deaths in 1990.[4] Prescription opioid overdose was responsible for more deaths in the United States from 1999-2008 than heroin and cocaine overdose combined.[5]
Signs and symptoms

Opioids, because of their effect on the part of the brain that regulates breathing, can during overdoses lead to the person not breathing (respiratory depression) and therefore result in death..[2] Opiate overdose symptoms and signs can be referred to as the "Opioid Overdose Triad": decreased level of consciousness, pinpoint pupils and respiratory depression.[6] Other symptoms include seizures and muscle spasms. Sometimes a person experiencing an opiate overdose can lead to such a decreased level of consciousness that he or she won't even wake up to their name being called or being shaken by another person.
Alcohol also causes respiratory depression and therefore when taken with opioids can increase the risk of respiratory depression and death.[2]
Co-ingestion
Opioid overdoses associated with a conjunction of benzodiazepines or alcohol use leads to a contraindicated condition wherein higher instances of general negative overdose traits native to the overdose profile of opioid use alone but to a much greater extent.[7][8] Other CNS depressants, or "downers", muscle relaxers, pain relievers, anti-convulsants, anxiolytics (anti-anxiety drugs), treatment drugs of a psychoactive or epileptic variety or any other such drug with its active function meant to calm or mitigate neuronal signaling (barbiturates, etc.) can additionally cause a worsened condition with less likelihood of recovery cumulative to each added drug of a diverse or disparate hampering effect to the central or peripheral nervous system of the user. This includes drugs less immediately classed to a slowing of the metabolism such as with GABAergics like GHB or glutamatergic antagonists like PCP or ketamine.
Prevention
Although opioid overdose accounts for the leading cause of accidental death, it can be prevented and often in primary care settings.[10][11] Clear protocols for staff at emergency departments and urgent care centers can reduce opioid prescriptions for individuals presenting in these settings who engage in "drug seeking" behaviors or who have a history of substance abuse.[12] Providers should routinely screen patients using tools such as the CAGE-AID and the Drug Abuse Screening Test (DAST-10) to screen adults and the CRAFFT to screen adolescents aged 14–18 years.[10] Other “drug seeking” behaviors and physical indications of drug use should be used as clues to perform formal screenings.[10]
Individuals diagnosed with opioid dependence should be prescribed naloxone to prevent overdose and/or should be directed to one of the many intervention/treatment options available, such as needle exchange programs and treatment centers.[10][11] Brief motivational interviewing can also be performed by the clinician during patient visits and has been shown to improve patient motivation to change their behavior.[10][13] Despite these opportunities, the dissemination of prevention interventions in the US has been hampered by the lack of coordination and sluggish federal government response.[11]
Treatment
Death can be prevented in opioid overdoses if patients receive basic life support and the administration of Naloxone soon after opioid overdose is suspected. Naloxone is effective at reversing the cause, rather than just the symptoms, of an opioid overdose.[14] A longer-acting variant is naltrexone. Naltrexone is primarily meant to treat opioid and alcohol dependence.
Programs to provide drug users and their caregivers with naloxone are recommended.[15] In the United States its use is estimated to have prevented 10,000 opioid overdose deaths.[16][17] Healthcare institution-based naloxone prescription programs have also helped reduce rates of opioid overdose in the US state of North Carolina, and have been replicated in the US military.[18][19] Nevertheless, scale-up of healthcare-based opioid overdose interventions are limited by providers’ insufficient knowledge and negative attitudes towards prescribing take-home naloxone to prevent opioid overdose.[20] Programs training police and fire personnel in opioid overdose response using naloxone have also shown promise.[21][22]
References
- ↑ Dart RC, Surratt HL, Cicero TJ, Parrino MW, Severtson SG, Bucher-Bartelson B, et al. Trends in opioid analgesic abuse and mortality in the United States. N Engl J Med. 2015 Jan 15. 372(3):241-8.
- 1 2 3 "WHO | Information sheet on opioid overdose". www.who.int. Retrieved 2015-11-13.
- 1 2 de Caen, AR; Berg, MD; Chameides, L; Gooden, CK; Hickey, RW; Scott, HF; Sutton, RM; Tijssen, JA; Topjian, A; van der Jagt, ÉW; Schexnayder, SM; Samson, RA (3 November 2015). "Part 12: Pediatric Advanced Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care.". Circulation 132 (18 Suppl 2): S526–42. PMID 26473000.
- ↑ GBD 2013 Mortality and Causes of Death, Collaborators (17 December 2014). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013.". Lancet 385: 117–171. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
- ↑ Debono, DJ; Hoeksema, LJ; Hobbs, RD (August 2013). "Caring for Patients with Chronic Pain: Pearls and Pitfalls". Journal of the American Osteopathic Association 113 (8): 620–627. doi:10.7556/jaoa.2013.023. PMID 23918913.
- ↑ Chandler, Stephanie. "Symptoms of an opiate overdose". Live Strong. Retrieved 17 May 2012.
- ↑ "BestBets: Concomitant use of benzodiazepines in opiate overdose and the association with a poorer outcome.".
- ↑ "BestBets: Concomitant use of alcohol in opiate overdose and the association with a poorer outcome.".
- ↑ Overdose Death Rates. By National Institute on Drug Abuse (NIDA).
- 1 2 3 4 5 Bowman S, Eiserman J, Beletsky L, Stancliff S, Bruce RD. (2013). "Reducing the health consequences of opioid addiction in primary care". Am J Med 126 (7): 565–71. doi:10.1016/j.amjmed.2012.11.031. PMID 23664112.In press
- 1 2 3 Beletsky L, Rich JD, Walley AY. (2012). "Prevention of Fatal Opioid Overdose". JAMA 308 (18): 1863–1864. doi:10.1001/jama.2012.14205. PMC 3551246. PMID 23150005.
- ↑ "Emergency Department and Urgent Care Clinicians Use Protocol To Reduce Opioid Prescriptions for Patients Suspected of Abusing Controlled Substances". Agency for Healthcare Research and Quality. 2014-03-12. Retrieved 2014-03-14.
- ↑ Zahradnik A, Otto C, Crackau B, et al. (2009). "Randomized controlled trial of a brief intervention for problematic prescription drug use in non-treatment-seeking patients". Addiction 104 (1): 109–117. doi:10.1111/j.1360-0443.2008.02421.x. PMID 19133895.
- ↑ Etherington, J; Christenson, J; Innes, G; Grafstein, E; Pennington, S; Spinelli, JJ; Gao, M; Lahiffe, B; et al. (2000). "Is early discharge safe after naloxone reversal of presumed opioid overdose?". CJEM 2 (3): 156–62. PMID 17621393.
- ↑ Community management of opioid overdose (PDF). World Health Organization. 2014. ISBN 9789241548816.
- ↑ "OD Prevention Program Locator.". Overdose Prevention Alliance. Retrieved 15 May 2012.
- ↑ Centers for Disease Control and Prevention (2012). "Community-Based Opioid Overdose Prevention Programs Providing Naloxone — United States, 2010". Morbidity and Mortality Weekly Report 61 (6): 101–5. PMID 22337174.
- ↑ Albert, Su; Brason Ii, Fred W.; Sanford, Catherine K.; Dasgupta, Nabarun; Graham, Jim; Lovette, Beth (2011). "Project Lazarus: Community-Based Overdose Prevention in Rural North Carolina". Pain Medicine 12: S77–85. doi:10.1111/j.1526-4637.2011.01128.x. PMID 21668761.
- ↑ Beletsky, Leo; Burris, Scott C.; Kral, Alex H. (July 21, 2009). "Closing Death's Door: Action Steps to Facilitate Emergency Opioid Drug Overdose Reversal in the United States". SSRN Electronic Journal. doi:10.2139/ssrn.1437163. SSRN 1437163.
- ↑ Beletsky, Leo; Ruthazer, Robin; MacAlino, Grace E.; Rich, Josiah D.; Tan, Litjen; Burris, Scott (2006). "Physicians' Knowledge of and Willingness to Prescribe Naloxone to Reverse Accidental Opiate Overdose: Challenges and Opportunities". Journal of Urban Health 84 (1): 126–36. doi:10.1007/s11524-006-9120-z. PMC 2078257. PMID 17146712.
- ↑ Beletsky L, Moroz E. "The Quincy Police Department: Pioneering Naloxone Among First Responders". Overdose Prevention Alliance. Retrieved 15 May 2012.
- ↑ Lavoie D. (April 2012). "Naloxone: Drug-Overdose Antidote Is Put In Addicts' Hands". Huffington Post.
External links
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||