Epidemiology of HIV/AIDS


HIV/AIDS is a global pandemic.[1] As of 2012, approximately 35.3 million people are living with HIV globally.[2] Of these, approximately 17.2 million are men, 16.8 million are women and 3.4 million are less than 15 years old.[3] There were about 1.8 million deaths from AIDS in 2010, down from 2.2 million in 2005.[3]
Sub-Saharan Africa is the region most affected. In 2010, an estimated 68% (22.9 million) of all HIV cases and 66% of all deaths (1.2 million) occurred in this region.[4] This means that about 5% of the adult population in this area is infected.[5] Here, in contrast to other regions, women compose nearly 60% of cases.[4] South Africa has the largest population of people with HIV of any country in the world, at 5.9 million.[4] In Tanzania, HIV/AIDS was reported to have a prevalence of 6% among Tanzanian adults aged 15 - 49 in 2007-2008. This figure is lower than 2003 when the country's HIV/AIDS prevalence was 8.8%.[6]
South & South East Asia (a region with about 2 billion people as of 2010, over 30% of the global population) has an estimated 4 million cases (12% of all people living with HIV), with about 250,000 deaths in 2010.[5] Approximately 2.5 million of these cases are in India, where however the prevalence is only about 0.3% (somewhat higher than that found in Western and Central Europe or Canada).[4] Prevalence is lowest in East Asia at 0.1%.[5]
In 2008 approximately 1.2 million people in the United States had HIV; 20% did not realize that they were infected.[7] Over the 10-year period from 1999-2008 it resulted in about 17,500 deaths per year.[7] In the United Kingdom, as of 2009, there were approximately 86,500 cases and 516 deaths.[8] In Australia, as of 2009, there were about 21,171 cases and around 23 deaths.[9] In Canada as of 2008 there were about 65,000 cases and 53 deaths.[10]
A reconstruction of its genetic history shows that the HIV pandemic almost certainly originated in Kinshasa, the capital of the Democratic Republic of the Congo, around 1920.[11] AIDS was first recognized in 1981 and by 2009 had caused nearly 30 million deaths.[12]
HIV in World
HIV in World in 2014 - data from CIA World Factbook[13]
| Region/Country | HIV/AIDS - adult prevalence rate | HIV/AIDS - people living with HIV/AIDS | HIV/AIDS - deaths |
|---|---|---|---|
| World | 0.79% | 36 872 500 | 1 181 700 |
| Africa | |||
| North Africa | 122 200 | 5 100 | |
| Sudan | 0.25% | 53 200 | 2 900 |
| Egypt | 0.02% | 8 800 | 300 |
| Libya | 0.3% (2012) | 10 000 (2012) | NA |
| Tunisia | 0.04% | 2 700 | 100 |
| Algeria | 0.04% | 10 500 | 200 |
| Morocco | 0.14% | 28 700 | 1 100 |
| Western Sahara | NA | NA | NA |
| Mauritania | 0.92% | 8 300 | 500 |
| Western Africa | |||
| Senegal | 0.53% | 44 000 | 2 400 |
| The Gambia | 1.82% | 20 300 | 900 |
| Guinea Bissau | 3.69% | 42 000 | 1 900 |
| Guinea | 1.55% | 118.000 | 3 800 |
| Sierra Leone | 1.4% | 54 000 | 2 700 |
| Liberia | 1.17% | 33 100 | 2 000 |
| Cote d'Ivore | 3.46% | 460 100 | 21 800 |
| Ghana | 1.47% | 250 200 | 9 200 |
| Togo | 2.4% | 113 700 | 4 300 |
| Benin | 1.14% | 77 900 | 2 400 |
| Nigeria | 3.17% | 3 391 600 | 174 300 |
| Niger | 0.49% | 51 800 | 3 400 |
| Burkina Faso | 0.94% | 107 700 | 3 800 |
| Mali | 1.42% | 133 400 | 5 300 |
| Cape Verde | 1.09% | 3 400 | 100 |
| Central Africa | |||
| Chad | 2.53% | 215 000 | 11 700 |
| Cameroon | 4.77% | 657 700 | 34 200 |
| Central African Republic | 4.25% | 135 400 | 9 900 |
| Sao Tome and Principe | 0.78% | 1 000 | 100 |
| Equatorial Guinea | 6.16% | 31 600 | 800 |
| Gabon | 3.91% | 47 500 | 1 500 |
| Republic of the Congo | 2.75% | 80 700 | 4 400 |
| Democratic Republic of the Congo | 1.04% | 446 600 | 24 100 |
| Angola | 2.41% | 304 400 | 11 770 |
| Eastern Africa | |||
| Eritrea | 0.68% | 16 100 | 700 |
| Djibouti | 1.59% | 9 900 | 600 |
| Somalia | 0.55% | 34 900 | 2 400 |
| Ethiopia | 1.15% | 730 300 | 23 400 |
| South Sudan | 2.71% | 193 400 | 12 700 |
| Kenya | 5.3% | 1 366 900 | 33 000 |
| Uganda | 7.25% | 1 486 600 | 32 900 |
| Rwanda | 2.82% | 210 500 | 3 000 |
| Burundi | 1.11% | 84 700 | 3 900 |
| Tanzania | 5.34% | 1 499 400 | 46 100 |
| Malawi | 10.04% | 1 063 900 | 32 600 |
| Mozambik | 10.58% | 1 543 000 | 44 900 |
| Zambia | 12.37% | 1 150 400 | 18 900 |
| Zimbabwe | 16.74% | 1 550 300 | 38 600 |
| Madagascar | 0.29% | 39 100 | 3 200 |
| Comoros | 0.1% (2012) | <500 (2012) | <100 (2012) |
| Mayotte | NA | NA | NA |
| Seychelles | NA | NA | NA |
| Mauritius | 0.92% | 8 300 | 500 |
| Reunion | NA | NA | NA |
| Southern Africa | |||
| Namibia | 15.97% | 245 400 (2013) | 5 100 |
| Botswana | 25.16% | 392 400 | 5 100 |
| Swaziland | 27.73% | 214 300 | 3 500 |
| Lesotho | 23.39% | 314 600 | 9 300 |
| South Africa | 18.92% | 6 836 500 | 138 400 |
| Asia | |||
| Western Asia | |||
| Georgia | 0.28% | 6 600 | 100 |
| Armenia | 0.22% | 4 000 | 200 |
| Azerbajian | 0.14% | 8 400 | 400 |
| Turkey | <0.1% (2012) | 4 600 (2012) | <200 (2012) |
| Iran | 0.14% | 74 400 | 4 100 |
| Iraq | <0.1% (2012) | <500 (2012) | NA |
| Syria | 0.01% | 900 | <100 |
| Jordan | <0.1% (2012) | 600 (2012) | <500 (2012) |
| Lebanon | 0.06% | 1 800 | <100 |
| Israel | 0.2% (2012) | 7 500 (2012) | <100 (2012) |
| Gaza Strip (Palestine) | NA | NA | NA |
| West Bank (Palestine) | NA | NA | NA |
| Yemen | 0.05% | 7 200 | 300 |
| Oman | 0.16% | 2 400 | <100 |
| United Arab Emirates | 0.2% (2012) | NA | NA |
| Qatar | <0.1% (2012) | <200 (2012) | <100 (2012) |
| Bahrain | 0.2% (2012) | <600 (2012) | <200 (2012) |
| Kuwait | 0.1% (2012) | NA | NA |
| Central Asia | |||
| Kazakhstan | 0.19% | 20 300 | 500 |
| Uzbekistan | 0.15% | 32 300 | 2 200 |
| Turkmenistan | <0.01% (2012) | <200 (2012) | <100 (2012) |
| Kyrgyzstan | 0.26% | 9 300 | 400 |
| Tajikistan | 0.35% | 16 400 | 700 |
| Afghanistan | 0.04% | 6 700 | 300 |
| Southern Asia | |||
| Pakistan | 0.09% | 93 900 | 2 800 |
| Nepal | 0.2% | 39 200 | 2 600 |
| Bhutan | 0.13% (2013) | 600 (2013) | 100 (2012) |
| India | 0.26% (2013) | 2 079 700 (2013) | 127 200 (2013) |
| Bangladesh | 0.01% | 8 900 | 700 |
| Sri Lanka | 0.03% | 3 300 | 100 |
| Maldives | 0.01% (2013) | <100 (2013) | <100 (2013) |
| Southeastern Asia | |||
| Myanmar (Burma) | 0.69% | 212 600 | 10 100 |
| Thailand | 1.13% | 445 600 | 19 400 |
| Laos | 0.26% | 11 100 | 500 |
| Cambodia | 0.64% | 74 600 | 2 600 |
| Vietnam | 0.47% | 250 200 | 10 600 |
| Malaysia | 0.45% | 100 800 | 9 000 |
| Singapore | 0.1% (2012) | 3 400 (2012) | <100 (2012) |
| Brunei | <0.1% (2012) | <200 (2012) | <200 (2012) |
| Philippines | 0.06% | 35 600 | 500 |
| Indonesia | 0.47% | 660 300 | 33 700 |
| East Timor (Timor-Leste) | NA | NA | NA |
| Eastern Asia | |||
| Mongolia | 0.04% (2013) | 600 (2013) | <100 (2013) |
| Japan | <0.1% (2012) | 8 100 (2012) | <100 (2012) |
| North Korea | NA | NA | NA |
| South Korea | <0.1% (2012) | 9 500 (2012) | <500 (2012) |
| China | 0.1% (2012) | 780 000 (2012) | 26 000 (2012) |
| Taiwan | NA | NA | NA |
| Hong Kong | 0.1% (2012) | 2 600 (2012) | <200 (2012) |
| Macau | NA | NA | NA |
| Australia and Oceania | |||
| Australia | 0.17% (2013) | 28 200 (2013) | <100 (2013) |
| New Zealand | 0.1% (2012) | 2 500 (2012) | <100 (2012) |
| Papua New Guinea | 0.72% | 37 200 | 900 |
| Palau | NA | NA | NA |
| Northern Mariana Islands | NA | NA | NA |
| Guam | NA | NA | NA |
| Federated States of Micronesia | NA | NA | NA |
| Marshall Islands | NA | NA | NA |
| Nauru | NA | NA | NA |
| Solomon Islands | NA | NA | NA |
| Vanuatu | NA | NA | NA |
| New Caledonia | NA | NA | NA |
| Fiji | 0.13% | 700 | <100 |
| Tuvalu | NA | NA | NA |
| Tokelau | NA | NA | NA |
| Wallis and Futuna | NA | NA | NA |
| Samoa | NA | NA | NA |
| American Samoa | NA | NA | NA |
| Tonga | NA | NA | NA |
| Niue | NA | NA | NA |
| Cook Islands | NA | NA | NA |
| French Polynesia | NA | NA | NA |
| Kiribati | NA | NA | NA |
| Americas | |||
| North America | |||
| Greenland | NA | 100 (1999) | NA |
| Saint Pierre and Miguelon | NA | NA | NA |
| Canada | 0.3% (2012) | 68 000 (2012) | <400 (2013) |
| USA | 0.6% (2012) | 1 200 000 (2012) | 17 000 (2012) |
| Bermuda | 0.3% (2012) | NA | NA |
| Central America | |||
| Mexico | 0.23% | 194 100 | 6 000 |
| Belize | 1.18% | 2 700 | 100 |
| Guatemala | 0.54% | 49 100 | 1 700 |
| El Salvador | 0.53% | 20 900 | 400 |
| Honduras | 0.42% | 23 000 | 1 200 |
| Nicaragua | 0.27% | 10 000 | 400 |
| Costa Rica | 0.26% | 8 800 | 200 |
| Panama | 0.65% | 16 600 | 600 |
| Carribean | |||
| The Bahamas | 3.22% (2013) | 7 700 (2013) | 500 (2013) |
| Cuba | 0.25% | 17 100 | 100 |
| Cayman Islands | NA | NA | NA |
| Turks and Caicos | NA | NA | NA |
| Jamaica | 1.62% | 29 400 | 1 300 |
| Haiti | 1.93% | 141 300 | 3 800 |
| Dominican Republic | 1.04% | 69 300 | 3 100 |
| Puerto Rico | NA | 7 397 (1997) | NA |
| British Virgin Islands | NA | NA | NA |
| USA Virgin Islands | NA | NA | NA |
| Anguilla | NA | NA | NA |
| Saint Kitts and Nevis | NA | NA | NA |
| Antigua and Barbuda | NA | NA | NA |
| Montserrat | NA | NA | NA |
| Guadeloupe | NA | NA | NA |
| Dominica | NA | NA | NA |
| Martinique | NA | NA | NA |
| Saint Lucia | NA | NA | NA |
| Saint Vincent and Grenadines | NA | NA | NA |
| Grenada | NA | NA | NA |
| Barbados | 0.88% (2013) | 1 500 (2012) | <100 (2009) |
| Trinidad and Tobago | 1.65% (2013) | 14 000 (2013) | 700 (2013) |
| Aruba | NA | NA | NA |
| Curacao | NA | NA | NA |
| South America | |||
| French Guiana | NA | NA | NA |
| Suriname | 1.02% | 3 800 | 200 |
| Guyana | 1.81% | 9 700 | 100 |
| Venezuela | 0.55% | 106 900 | 4 400 (2013) |
| Colombia | 0.4% | 124 400 | 4 700 |
| Ecuador | 0.34% | 32 700 | 1 200 |
| Peru | 0.36% | 71 900 | 2 500 |
| Bolivia | 0.29% | 17 900 | 700 |
| Chile | 0.29% | 39 300 | 700 |
| Paraguay | 0.41% | 16 800 | 400 |
| Uruguay | 0.7% | 14 400 | 600 |
| Argentina | 0.47% | 126 600 | 1 500 |
| Falkland Islands | NA | NA | NA |
| Brazil | 0.55% (2013) | 726 000 (2013) | 15 800 (2013) |
| Europe | |||
| Russia | 1% (2012) | 980 000 (2012) | 40 000 (2007) |
| Ukraine | 0.83% (2013) | 210 700 (2013) | 13 400 (2013) |
| Estonia | 1.3% (2013) | 8 600 (2013) | <500 (2012) |
| Latvia | 0.7% (2012) | 8 600 (2012) | <1 000 (2012) |
| Lithuania | 0.1% (2009) | 1 200 | <100 (2009) |
| Belarus | 0.52% | 29 400 | 1 000 |
| Poland | 0.07% | 27 000 (2009) | <200 (2009) |
| Moldova | 0.63% | 17 600 | 800 |
| Romania | 0.11% (2013) | 16 200 (2013) | 500 (2013) |
| Bulgaria | 0.1% (2012) | 3 800 (2012) | <200 (2012) |
| Czech Republic | 0.05% (2013) | 3 400 (2013) | <100 (2013) |
| Slovakia | 0.02% | <500 (2012) | <100 |
| Slovenia | 0.08% | 900 | <100 |
| Hungary | <0.1% (2012) | 3 000 (2012) | 100 (2013) |
| Croatia | <0.1% (2012) | <1 000 (2012) | <100 (2012) |
| Bosnia and Herzegovina | <0.1% (2012) | 900 (2012) | 100 (2012) |
| Serbia | 0.05% (2013) | 3 000 (2013) | 100 (2013) |
| Montenegro | NA | NA | NA |
| Albania | 0.04% (2013) | NA | NA |
| Kosovo | NA | NA | NA |
| Macedonia | 0.01% (2013) | 200 (2013) | <100 (2013) |
| Greece | 0.1% (2012) | 8 800 (2012) | <500 (2012) |
| Cyprus | 0.06% (2013) | 400 (2013) | <100 (2013) |
| Malta | 0.1% (2012) | <500 (2012) | <100 (2012) |
| San Marino | NA | NA | NA |
| Italy | 0.28% (2013) | 122 000 (2013) | <1 000 (2012) |
| Gibraltar | NA | NA | NA |
| Portugal | 0.6% (2012) | 42 000 (2012) | <500 (2012) |
| Spain | 0.42% (2013) | 150 400 (2013) | 800 (2013) |
| Andorra | NA | NA | NA |
| Monaco | NA | NA | NA |
| France | 0.4% (2012) | 150 000 (2012) | 1 500 (2013) |
| Netherlands | 0.2% (2012) | 22 000 (2012) | <100 (2012) |
| Belgium | 0.2% (2012) | 14 000 (2012) | <100 (2012) |
| Luxembourg | 0.3% (2012) | <1 000 (2012) | <100 (2012) |
| Switzerland | 0.35% (2013) | 20 200 (2013) | 300 (2013) |
| Liechtenstein | NA | NA | NA |
| Austria | 0.3% (2012) | 15 000 (2012) | <100 (2012) |
| Germany | 0.15% (2013) | 77 500 (2013) | 400 (2013) |
| Denmark | 0.16% | 6 000 | <100 |
| Finland | 0.1% (2012) | 2 600 (2012) | <100 (2012) |
| Sweden | 0.18% | 8 100 (2012) | 100 |
| Norway | 0.15% | 5 800 | <100 |
| Faroe Islands | NA | NA | NA |
| Iceland | 0.3% (2012) | <1 000 (2012) | <100 (2012) |
| Ireland | 0.28% | 8 000 | 100 |
| United Kingdom | 0.33% (2013) | 126 700 (2013) | <600 (2013) |
By region
The pandemic is not homogeneous within regions, with some countries more afflicted than others. Even at the country level, there are wide variations in infection levels between different areas. The number of people infected with HIV continues to rise in most parts of the world, despite the implementation of prevention strategies, Sub-Saharan Africa being by far the worst-affected region, with an estimated 22.9 million at the end of 2010, 68% of the global total.[14]
South and South East Asia have an estimated 12% of the global total.[15] The rate of new infections has fallen slightly since 2005 after a more rapid decline between 1997 and 2005.[14] Annual AIDS deaths have been continually declining since 2005 as antiretroviral therapy has become more widely available.
| World region[14] | Estimated prevalence of HIV infection (adults and children) |
Estimated adult and child deaths during 2010 | Adult prevalence (%) |
|---|---|---|---|
| Worldwide | 31.6 million – 35.2 million | 1.6 – 1.9 million | 0.8% |
| Sub-Saharan Africa | 21.6 million – 24.1 million | 1.2 million | 5.0% |
| South and South-East Asia | 3.6 million – 4.5 million | 250,000 | 0.3% |
| Eastern Europe and Central Asia | 1.3 million – 1.7 million | 90,000 | 0.9% |
| Latin America | 1.2 million – 1.7 million | 67,000 | 0.4% |
| North America | 1.0 million – 1.9 million | 20,000 | 0.6% |
| East Asia | 580,000 – 1.1 million | 56,000 | 0.1% |
| Western and Central Europe | 770,000 – 930,000 | 9,900 | 0.2% |
Sub-Saharan Africa
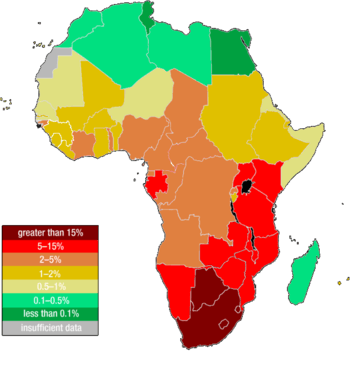
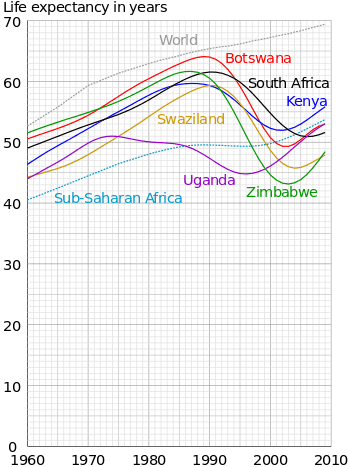
Sub-Saharan Africa remains the hardest-hit region. HIV infection is becoming endemic in sub-Saharan Africa, which is home to just over 12% of the world’s population but two-thirds of all people infected with HIV.[14] The adult HIV prevalence rate is 5.0% and between 21.6 million and 24.1 million total are affected.[14] However, the actual prevalence varies between regions. Presently, Southern Africa is the hardest hit region, with adult prevalence rates exceeding 20% in most countries in the region, and 30% in Swaziland and Botswana.
Eastern Africa also experiences relatively high levels of prevalence with estimates above 10% in some countries, although there are signs that the pandemic is declining in this region. West Africa on the other hand has been much less affected by the pandemic. Several countries reportedly have prevalence rates around 2 to 3%, and no country has rates above 10%. In Nigeria and Côte d'Ivoire, two of the region's most populous countries, between 5 and 7% of adults are reported to carry the virus.
Across Sub-Saharan Africa, more women are infected with HIV than men, with 13 women infected for every 10 infected men. This gender gap continues to grow. Throughout the region, women are being infected with HIV at earlier ages than men. The differences in infection levels between women and men are most pronounced among young people (aged 15–24 years). In this age group, there are 36 women infected with HIV for every 10 men. The widespread prevalence of sexually transmitted diseases, the practice of scarification, unsafe blood transfusions, and the poor state of hygiene and nutrition in some areas may all be facilitating factors in the transmission of HIV-1 (Bentwich et al., 1995).
Mother-to-child transmission is another contributing factor in the transmission of HIV-1 in developing nations. Due to a lack of testing, a shortage in antenatal therapies and through the feeding of contaminated breast milk, 590,000 infants born in developing countries are infected with HIV-1 per year. In 2000, the World Health Organization estimated that 25% of the units of blood transfused in Africa were not tested for HIV, and that 10% of HIV infections in Africa were transmitted via blood.
Poor economic conditions (leading to the use of dirty needles in healthcare clinics) and lack of sex education contribute to high rates of infection. In some African countries, 25% or more of the working adult population is HIV-positive. Poor economic conditions caused by slow onset-emergencies, such as drought, or rapid onset natural disasters and conflict can result in young women and girls being forced into using sex as a survival strategy.[17] Worse still, research indicates that as emergencies, such as drought, take their toll and the number of potential 'clients' decreases, women are forced by clients to accept greater risks, such as not using contraceptives.[17]
AIDS-denialist policies have impeded the creation of effective programs for distribution of antiretroviral drugs. Denialist policies by former South African President Thabo Mbeki's administration led to several hundred thousand unnecessary deaths.[18][19] UNAIDS estimates that in 2005 there were 5.5 million people in South Africa infected with HIV — 12.4% of the population. This was an increase of 200,000 people since 2003.
Although HIV infection rates are much lower in Nigeria than in other African countries, the size of Nigeria's population meant that by the end of 2003, there were an estimated 3.6 million people infected. On the other hand, Uganda, Zambia, Senegal, and most recently Botswana have begun intervention and educational measures to slow the spread of HIV, and Uganda has succeeded in actually reducing its HIV infection rate.
Middle East and North Africa
HIV/AIDS prevalence in the Middle East and North Africa is around 0.2% (0.1–0.7%), with between 230,000 and 1.4 million people infected. Among young people 15–24 years of age, 0.3% of women [0.1–0.8%] and 0.17% of men [0.1–0.3%] were living with HIV infection by the end of 2004.
Approximately 500,000 people are living with HIV in the MENA region. This number is estimated at 470,000 (350,000–570,000) without Afghanistan and Pakistan (which are not considered by UNAIDS geographic definition as part of MENA region), and reaches 580,000 (430,000–810,000) if Pakistan and Afghanistan are included.[20]
Despite the low prevalence of HIV/AIDS in the MENA region, there are epidemics among vulnerable groups. As of 2012, the prevalence of HIV among men who have sex with men in Egypt is estimated to be 5.0%-9.9%.[21]
South and South-East Asia
The HIV prevalence rate in South and South-East Asia is less than 0.35 percent, with total of 4.2 – 4.7 million adults and children infected. More AIDS deaths (480,000) occur in this region than in any other except sub-Saharan Africa. The geographical size and human diversity of South and South-East Asia have resulted in HIV epidemics differing across the region. The AIDS picture in South Asia is dominated by the epidemic in India.
In South and Southeast Asia, the HIV epidemic remains largely concentrated in injecting drug users, men who have sex with men, sex workers, and clients of sex workers and their immediate sexual partners.[22] In the Philippines, in particular, sexual contact between males comprise the majority of new infections. An HIV surveillance study conducted by Dr. Louie Mar Gangcuangco and colleagues from the University of the Philippines-Philippine General Hospital showed that out of 406 MSM tested for HIV in Metro Manila, HIV prevalence was 11.8% (95% confidence interval: 8.7- 15.0).[23][24]
Migrants, in particular, are vulnerable and 67% of those infected in Bangladesh and 41% in Nepal are migrants returning from India.[22] This is in part due to human trafficking and exploitation, but also because even those migrants who willingly go to India in search of work are often afraid to access state health services due to concerns over their immigration status.[22]
East Asia
The national HIV prevalence levels in East Asia is 0.1% in the adult (15–49) group. However, due to the large populations of many East Asian nations, this low national HIV prevalence still means that large numbers of people are infected with HIV. The picture in this region is dominated by China. Much of the current spread of HIV in China is through injecting drug use and paid sex. In China, the number was estimated at between 430,000 and 1.5 million by independent researchers, with some estimates going much higher.
In the rural areas of China, where large numbers of farmers, especially in Henan province, participated in unclean blood transfusions; estimates of those infected are in the tens of thousands. In Japan, just over half of HIV/AIDS cases are officially recorded as occurring amongst homosexual men, with the remainder occurring amongst heterosexuals and also via drug abuse, in the womb or unknown means.
Americas
Caribbean
The Caribbean is the second-most affected region in the world.[14] Among adults aged 15–44, AIDS has become the leading cause of death. The region's adult prevalence rate is 0.9%.[14] with national rates ranging up to 2.7%.[25] HIV transmission occurs largely through heterosexual intercourse, with two-thirds of AIDS cases in this region attributed to this route. Sex between men is also a significant route of transmission, even though it is heavily stigmatised and illegal in many areas. HIV transmission through injecting drug use remains rare, except in Bermuda and Puerto Rico.
Central and South America
In these regions of the American continent, only Guatemala and Honduras have national HIV prevalence of over 1%. In these countries, HIV-infected men outnumber HIV-infected women by roughly 3:1.
United States and Canada
The adult prevalence rate in this region is 0.7% with over 1 million people currently infected with HIV. In the United States from 2001–2005, the highest transmission risk behaviors were sex between men (40–49% of new cases) and high risk heterosexual sex (32–35% of new cases).[26] Currently, rates of HIV infection in the US are highest in the eastern and southern regions, with the exception of California. Currently, 35,000–40,000 new infections occur in the USA every year. AIDS is one of the top three causes of death for African American men aged 25–54 and for African American women aged 35–44 years in the United States of America. In the United States, African Americans make up about 48% of the total HIV-positive population and make up more than half of new HIV cases, despite making up only 12% of the population. The main route of transmission for women is through unprotected heterosexual sex. African American women are 19 times more likely to contract HIV than other women.[27]
In the United States in particular, a new wave of infection is being blamed on the use of methamphetamine, known as crystal meth. Research presented at the 12th Annual Retrovirus Conference in Boston in February 2005 concluded that using crystal meth or cocaine is the biggest single risk factor for becoming HIV+ among US gay men, contributing 29% of the overall risk of becoming positive and 28% of the overall risk of being the receptive partner in anal sex.[28]
In addition, several renowned clinical psychologists now cite methamphetamine as the biggest problem facing gay men today, including Michael Majeski, who believes meth is the catalyst for at least 80% of seroconversions currently occurring across the United States, and Tony Zimbardi, who calls methamphetamine the number one cause of HIV transmission, and says that high rates of new HIV infection are not being found among non-crystal users. In addition, various HIV and STD clinics across the United States report anecdotal evidence that 75% of new HIV seroconversions they deal with are methamphetamine-related; indeed, in Los Angeles, methamphetamine is regarded as the main cause of HIV seroconversion among gay men in their late thirties.[28] The chemical "methamphetamine", in and of itself, cannot infect someone with HIV.
Washington, D.C., the nation's capital, also has the nation's highest rate of infection, at 3%. This rate is comparable to what is seen in west Africa, and is considered a severe epidemic.[29]
In Canada, nearly 60,000 people were living with HIV/AIDS in 2005.[30] The HIV-positive population continues to increase in Canada, with the greatest increases amongst aboriginal Canadians.[31] As in Western Europe, the death rate from AIDS in North America fell sharply with the introduction of combination AIDS therapies (HAART).
In the United States, young African-American women are also at high risk for HIV infection.[32] African Americans make up 10% of the population but about half of the HIV/AIDS cases nationwide.[33] This is due in part to a lack of information about AIDS and a perception that they are not vulnerable, as well as to limited access to health-care resources and a higher likelihood of sexual contact with at-risk male sexual partners.[34] There are also geographic disparities in AIDS prevalence in the United States, where it is most common in the large metropolitan areas of the East Coast and California and in urban areas of the Deep South.[35] Rates are lower in Utah, Texas, and Northern Florida.[35]
Since 1985, the incidence of HIV infection among women has been steadily increasing. It is currently estimated that at least 27% of new HIV infections are in women.[36] There has been increasing concern for the concurrency of violence surrounding women infected with HIV. In 2012, a meta-analysis showed that the rates of psychological trauma, including Intimate Partner Violence and PTSD in HIV positive women were more than five times and twice the national averages, respectively.[37] In 2013, the White House commissioned an Interagency Federal Working Group to address the intersection of violence and women infected with HIV.[38]
A review of studies containing data regarding the prevalence of HIV in transgender women found that nearly 11.8% self-reported that they were infected with HIV.[39] In the National Transgender Discrimination Survey, 20.23% of black respondents reported being HIV-positive, with an additional 10% reporting that they were unaware of their status.[40]
Eastern Europe and Central Asia
There is growing concern about a rapidly growing epidemic in Eastern Europe and Central Asia, where an estimated 1.23–3.7 million people were infected as of December 2011, though the adult (15–49) prevalence rate is low (1.1%). The rate of HIV infections began to grow rapidly from the mid-1990s, due to social and economic collapse, increased levels of intravenous drug use and increased numbers of prostitutes. By 2010 the number of reported cases in Russia was over 450,000 according to the World Health Organization, up from 15,000 in 1995 and 190,000 in 2002; some estimates claim the real number is up to eight times higher, well over 2 million. There are predictions that the infection rate in Russia will continue to rise quickly, since education there about AIDS is almost non-existent.[41]
Ukraine and Estonia also have growing numbers of infected people, with estimates of 650,000 and 4,400 respectively in 2011. The disease is now officially epidemic in this region, which means that prevention strategies may not be able to halt and reverse its spread. Also, transmission of HIV is increasing through sexual contact and drug use among the young (<30 years). Indeed, over 84% of current AIDS cases in this region occur in non-drug-using heterosexuals less than 26 years of age.
Western Europe
In most countries of Western Europe, AIDS cases have fallen to levels not seen since the original outbreak; many attribute this trend to aggressive educational campaigns, screening of blood transfusions and increased use of condoms. Also, the death rate from AIDS in Western Europe has fallen sharply, as new AIDS therapies have proven to be an effective (though expensive) means of suppressing HIV.
In this area, the routes of transmission of HIV is diverse, including paid sex, injecting drug use, mother to child, male with male sex and heterosexual sex. However, many new infections in this region occur through contact with HIV-infected individuals from other regions. The adult (15–49) prevalence in this region is 0.3% with between 570,000 and 890,000 people currently infected with HIV infection. Due to the availability of antiretroviral therapy, AIDS deaths have stayed low since the lows of the late 1990s. However, in some countries, a large share of HIV infections remain undiagnosed and there is worrying evidence of antiretroviral drug resistance among some newly HIV-infected individuals in this region.
Oceania
There is a very large range of national situations regarding AIDS and HIV in this region. This is due, in part, to the large distances between the islands of Oceania. The wide range of development in the region also plays an important role. The prevalence is estimated at between 0.2% and 0.7%, with between 45,000 and 120,000 adults and children currently infected with HIV.
Papua New Guinea has one of the most serious AIDS epidemics in the region. According to UNAIDS, HIV cases in the country have been increasing at a rate of 30 percent annually since 1997, and the country's HIV prevalence rate in late 2006 was 1.3%.[42]
AIDS and society
In June 2001, the United Nations held a Special General Assembly to intensify international action to fight the HIV/AIDS epidemic as a global health issue, and to mobilize the resources needed towards this aim, labelling the situation a "global crisis".[43]
Regarding the social effects of the HIV/AIDS pandemic, some sociologists suggest that AIDS has caused a "profound re-medicalization of sexuality".[44][45]
Social factors also influence HIV/AIDS. A 2003 study states that HIV and AIDS are less prevalent in Muslim populations and speculates that this may be due to the effect of several Islamic tenets, such as the avoidance of extramarital affairs and the "benefits arising from circumcision".[46]
See also
Notes
- ↑ Cohen, MS; Hellmann, N; Levy, JA; DeCock, K; Lange, J (April 2008). "The spread, treatment, and prevention of HIV-1: evolution of a global pandemic". The Journal of Clinical Investigation 118 (4): 1244–54. doi:10.1172/JCI34706. PMC 2276790. PMID 18382737. Retrieved 17 September 2012.
- ↑ "Fact Sheet". UNAIDS.org. 2013. Retrieved 4 December 2013.
- 1 2 UNAIDS 2011 pg. 1-10
- 1 2 3 4 UNAIDS 2011 pg. 20-30
- 1 2 3 UNAIDS 2011 pg. 40-50
- ↑ Exavery, Amon; Lutambi, Angelina M; Mubyazi, Godfrey M; Kweka, Khadija; Mbaruku, Godfrey; Masanja, Honorati (2011). "Multiple sexual partners and condom use among 10 - 19 year-olds in four districts in Tanzania: What do we learn?". BMC Public Health 11 (1): 490. doi:10.1186/1471-2458-11-490. ISSN 1471-2458.
- 1 2 Centers for Disease Control and Prevention, (CDC) (3 Jun 2011). "HIV surveillance--United States, 1981-2008.". MMWR. Morbidity and mortality weekly report 60 (21): 689–93. PMID 21637182.
- ↑ Health Protection Agency (2010). HIV in the United Kingdom: 2010 Report.
- ↑ Benson, Kate (19 October 2010). "HIV rate rising but other infections less common". The Sydney Morning Herald. Retrieved 19 October 2010.
- ↑ Surveillance; riques, Risk Assessment Division = Le VIH et le sida au Canada: rapport de surveillance en date du 31 décembre 2009 / Division de la surveillance et de l'évaluation des (2010). HIV and AIDS in Canada : surveillance report to December 31, 2009 (PDF). Ottawa: Public Health Agency of Canada, Centre for Communicable Diseases and Infection Control, Surveillance and Risk Assessment Division. ISBN 978-1-100-52141-1. Cite uses deprecated parameter
|coauthors=(help) - ↑ "HIV pandemic's origins located". University of Oxford. 3 October 2014. Retrieved 5 October 2014.
- ↑ "Global Report Fact Sheet" (PDF). UNAIDS. 2010.
- ↑ https://www.cia.gov/library/publications/resources/the-world-factbook/
- 1 2 3 4 5 6 7 "UNAIDS World Aids Day Report" (PDF). publisher. 2011. Retrieved 12 March 2014.
The ranges define the boundaries within which the actual numbers lie, based on the best available information.
- ↑ UNAIDS, WHO (2007). "2007 AIDS epidemic update" (PDF). Archived (PDF) from the original on 27 May 2008. Retrieved 2008-05-26.
- ↑ "Life expectancy at birth, total (years)". worldbank.org.
- 1 2 Samuels, Fiona (2009) HIV and emergencies: one size does not fit all London: Overseas Development Institute
- ↑ Chigwedere P, Seage GR, Gruskin S, Lee TH, Essex M (October 2008). "Estimating the Lost Benefits of Antiretroviral Drug Use in South Africa". Journal of acquired immune deficiency syndromes (1999) 49 (4): 410–415. doi:10.1097/QAI.0b013e31818a6cd5. PMID 19186354. Lay summary.
- ↑ Nattrass N (February 2008). "Estimating the Lost Benefits of Antiretroviral Drug Use in South Africa". African Affairs 107 (427): 157–76. doi:10.1093/afraf/adm087.
- ↑ "UNAIDS Middle East and North Africa Regional Report on AIDS 2011" (PDF). Retrieved 2014-12-16.
- ↑ "HIV in the Middle East: Low Prevalence but Not Low Risk". pbr.org. Population Reference Bureau. Retrieved 24 August 2014.
- 1 2 3 Fiona Samuels and Sanju Wagle 2011. Population mobility and HIV and AIDS: review of laws, policies and treaties between Bangladesh, Nepal and India. London: Overseas Development Institute
- ↑ Gangcuangco LM, Tan ML, Berba RP. "Prevalence and risk factors for HIV infection among men having sex with men in Metro Manila, Philippines". Southeast Asian Journal of Tropical Medicine and Public Health 2013 Sep; 44(5) 810-816. http://www.tm.mahidol.ac.th/seameo/2013-44-5/10-5743-12.pdf
- ↑ Gangcuangco, et al. http://www.iasociety.org/Abstracts/A200739361.aspx
- ↑ UNAIDS, WHO (2005). AIDS epidemic update 2005.
- ↑ "Cases of HIV infection and AIDS in the United States and Dependent Areas, 2005". Centers for Disease Control and Prevention. June 2007. Retrieved 2010-12-27.
- ↑ "Kaiser Daily HIV/AIDS Report Summarizes Opinion Pieces on U.S. AIDS Epidemic". The Body – The Complete HIV/AIDS Resource. 20 June 2005. Retrieved 2010-12-27.
- 1 2 "Life or Meth". Retrieved 2010-12-27.
- ↑ AIDS epidemic in Washington D.C.
- ↑ "The State of the HIV/AIDS Pandemic". Public Health Agency of Canada. Archived from the original on 4 January 2010. Retrieved 2010-01-05.
- ↑ "CBC News In Depth – AIDS". CBC.ca. 1 December 2008. Archived from the original on 4 December 2008. Retrieved 2008-12-01.
- ↑ "Report: Black U.S. AIDS rates rival some African nations". cnn.com.
- ↑ "DTL&feed=rss. news_politics White House summit on AIDS' impact on black men". San Francisco Chronicle. 3 June 2010.
- ↑ Arya M, Behforouz HL, and Viswanath K (9 March 2009). "African American Women and HIV/AIDS: A National Call for Targeted Health Communication Strategies to Address a Disparity". The AIDS Reader 19 (2).
- 1 2 http://www.cdc.gov/hiv/topics/surveillance/resources/reports/2005report/pdf/2005SurveillanceReport.pdf
- ↑ CDC. HIV/AIDS Surveillance Report, 2005. Vol. 17. Rev ed. Atlanta: US Department of Health and Human Services, CDC: 2007:1–46. Available at http://www.cdc. gov/hiv/topics/surveillance/resources/reports/. Accessed 28 June 2007.
- ↑ Machtinger EL, Wilson TC, Haberer JE, Weiss DS. Psychological trauma and PTSD in HIV-positive women: a meta-analysis. AIDS Behav. 2012 Nov;16(8):2091-100. doi: 10.1007/s10461-011-0127-4. http://www.medscape.com/viewarticle/773935
- ↑ http://www.whitehouse.gov/sites/default/files/docs/vaw-hiv_working_group_report_final_-_9-6--2013.pdf
- ↑ "Estimating HIV Prevalence and Risk Behaviors of Transgender Persons in the United States: A Systematic Review". AIDS and Behavior.
- ↑ "Injustice at Every Turn: A Look at Black Respondents in the National Transgender Discrimination Survey" (PDF). National Black Justice Coalition, National Center for Transgender Equality, and National Gay and Lesbian Task Force. Retrieved April 7, 2015.
- ↑ Center for Strategic and International Studies. http://csis.org/program/hivaids
- ↑ Health Profile: Papua New Guinea. United States Agency for International Development (September 2008). Accessed 20 March 2009.
- ↑ United Nations Special Session on HIV/AIDS. New York, 25–27 June 2001 - http://www.un.org/ga/aids/conference.html
- ↑ Aggleton, Peter; Parker, Richard Bordeaux; Barbosa, Regina Maria (2000). Framing the sexual subject: the politics of gender, sexuality, and power. Berkeley: University of California Press. ISBN 0-520-21838-8. p.3
- ↑ Vance, Carole S. (1991). "Anthropology Rediscovers Sexuality: A Theoretical Comment". Social Science and Medicine 33 (8): 875–884. doi:10.1016/0277-9536(91)90259-F. PMID 1745914.
- ↑ Gray, Peter B. (Harvard University) (May 2004). "HIV and Islam: is HIV prevalence lower among Muslims?". Social Science & Medicine 58 (9): 1751–6. doi:10.1016/S0277-9536(03)00367-8. PMID 14990375.
- References
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2011). Global HIV/AIDS Response, Epidemic update and health sector progress towards universal access (PDF). Joint United Nations Programme on HIV/AIDS.
Further reading
- Global report with AIDS info database from UNAIDS
- Global, regional and national profiles from AVERT.org
- The River: A Journey to the Source of HIV and AIDS Edward Hooper (1999) ISBN 978-0-316-37261-9
- IASSTD & AIDS – Indian Association for the Study of Sexually Transmitted Diseases & AIDS
- AIDS.gov – The U.S. Federal Domestic HIV/AIDS Resource
| ||||||