Influenza
| Influenza | |
|---|---|
|
Influenza virus, magnified approximately 100,000 times | |
| Classification and external resources | |
| Specialty | Infectious disease |
| ICD-10 | J10, J11 |
| ICD-9-CM | 487 |
| OMIM | 614680 |
| DiseasesDB | 6791 |
| MedlinePlus | 000080 |
| eMedicine | med/1170 ped/3006 |
| Patient UK | Influenza |
| MeSH | D007251 |

Influenza, commonly known as "the flu", is an infectious disease caused by an influenza virus.[1] Symptoms can be mild to severe.[2] The most common symptoms include: a high fever, runny nose, sore throat, muscle pains, headache, coughing, and feeling tired. These symptoms typically begin two days after exposure to the virus and most last less than a week. The cough, however, may last for more than two weeks.[1] In children, there may be nausea and vomiting, but these are not common in adults. Nausea and vomiting occur more commonly in the unrelated infection gastroenteritis, which is sometimes inaccurately referred to as "stomach flu" or "24-hour flu".[3] Complications of influenza may include viral pneumonia, secondary bacterial pneumonia, sinus infections, and worsening of previous health problems such as asthma or heart failure.[2][4]
Three types of influenza viruses affect people, called Type A, Type B, and Type C.[4] Usually, the virus is spread through the air from coughs or sneezes.[1] This is believed to occur mostly over relatively short distances.[5] It can also be spread by touching surfaces contaminated by the virus and then touching the mouth or eyes.[2][5] A person may be infectious to others both before and during the time they are sick.[2] The infection may be confirmed by testing the throat, sputum, or nose for the virus. A number of rapid tests are available; however, people may still have the infection if the results are negative. A type of polymerase chain reaction that detects the virus's RNA is more accurate.[4]
Frequent hand washing reduces the risk of infection because the virus is inactivated by soap.[6] Wearing a surgical mask is also useful.[6] Yearly vaccinations against influenza are recommended by the World Health Organization for those at high risk. The vaccine is usually effective against three or four types of influenza.[1] It is usually well tolerated. A vaccine made for one year may not be useful in the following year, since the virus evolves rapidly. Antiviral drugs such as the neuraminidase inhibitors oseltamivir among others have been used to treat influenza.[1] Their benefits in those who are otherwise healthy do not appear to be greater than their risks.[7] No benefit has been found in those with other health problems.[7][8]
Influenza spreads around the world in a yearly outbreak, resulting in about three to five million cases of severe illness and about 250,000 to 500,000 deaths.[1] In the Northern and Southern parts of the world outbreaks occur mainly in winter while in areas around the equator outbreaks may occur at any time of the year.[1] Death occurs mostly in the young, the old and those with other health problems.[1] Larger outbreaks known as pandemics are less frequent.[4] In the 20th century three influenza pandemics occurred: Spanish influenza in 1918, Asian influenza in 1958, and Hong Kong influenza in 1968, each resulting in more than a million deaths.[9] The World Health Organization declared an outbreak of a new type of influenza A/H1N1 to be a pandemic in June 2009.[10] Influenza may also affect other animals, including pigs, horses and birds.[11]
Signs and symptoms
| Symptom: | sensitivity | specificity |
|---|---|---|
| Fever | 68–86% | 25–73% |
| Cough | 84–98% | 7–29% |
| Nasal congestion | 68–91% | 19–41% |
| ||

Approximately 33% of people with influenza are asymptomatic.[14]
Symptoms of influenza can start quite suddenly one to two days after infection. Usually the first symptoms are chills or a chilly sensation, but fever is also common early in the infection, with body temperatures ranging from 38 to 39 °C (approximately 100 to 103 °F).[15] Many people are so ill that they are confined to bed for several days, with aches and pains throughout their bodies, which are worse in their backs and legs.[16] Symptoms of influenza may include:
- Fever and extreme coldness (chills shivering, shaking (rigor))
- Cough
- Nasal congestion
- Runny nose
- Sneezing
- Body aches, especially joints and throat
- Fatigue
- Headache
- Irritated, watering eyes
- Reddened eyes, skin (especially face), mouth, throat and nose
- Petechial rash[17]
- In children, gastrointestinal symptoms such as diarrhea and abdominal pain,[18][19] (may be severe in children with influenza B)[20]
It can be difficult to distinguish between the common cold and influenza in the early stages of these infections,[21] but a flu can be identified by a high fever with a sudden onset and extreme fatigue. Influenza is a mixture of symptoms of common cold and pneumonia, body ache, headache, and fatigue. Diarrhea is not normally a symptom of influenza in adults,[12] although it has been seen in some human cases of the H5N1 "bird flu"[22] and can be a symptom in children.[18] The symptoms most reliably seen in influenza are shown in the table to the right.[12]
Since antiviral drugs are effective in treating influenza if given early (see treatment section, below), it can be important to identify cases early. Of the symptoms listed above, the combinations of fever with cough, sore throat and/or nasal congestion can improve diagnostic accuracy.[23] Two decision analysis studies[24][25] suggest that during local outbreaks of influenza, the prevalence will be over 70%,[25] and thus patients with any of these combinations of symptoms may be treated with neuraminidase inhibitors without testing. Even in the absence of a local outbreak, treatment may be justified in the elderly during the influenza season as long as the prevalence is over 15%.[25]
The available laboratory tests for influenza continue to improve. The United States Centers for Disease Control and Prevention (CDC) maintains an up-to-date summary of available laboratory tests.[26] According to the CDC, rapid diagnostic tests have a sensitivity of 50–75% and specificity of 90–95% when compared with viral culture.[27] These tests may be especially useful during the influenza season (prevalence=25%) but in the absence of a local outbreak, or peri-influenza season (prevalence=10%[25]).
Occasionally, influenza can cause severe illness including primary viral pneumonia or secondary bacterial pneumonia.[28][29] The obvious symptom is trouble breathing. In addition, if a child (or presumably an adult) seems to be getting better and then relapses with a high fever, that is a danger sign since this relapse can be bacterial pneumonia.[30]
Virology
Types of virus

In virus classification influenza viruses are RNA viruses that make up three of the five genera of the family Orthomyxoviridae:[31]
These viruses are only distantly related to the human parainfluenza viruses, which are RNA viruses belonging to the paramyxovirus family that are a common cause of respiratory infections in children such as croup,[32] but can also cause a disease similar to influenza in adults.[33]
A fourth family of influenza viruses has been proposed - influenza D.[34][35][36][37][38][39][40] The type species for this family is Bovine Influenza D virus which was first isolated in 2012.
Influenzavirus A
This genus has one species, influenza A virus. Wild aquatic birds are the natural hosts for a large variety of influenza A. Occasionally, viruses are transmitted to other species and may then cause devastating outbreaks in domestic poultry or give rise to human influenza pandemics.[41] The type A viruses are the most virulent human pathogens among the three influenza types and cause the severest disease. The influenza A virus can be subdivided into different serotypes based on the antibody response to these viruses.[42] The serotypes that have been confirmed in humans, ordered by the number of known human pandemic deaths, are:
- H1N1, which caused Spanish Flu in 1918, and Swine Flu in 2009
- H2N2, which caused Asian Flu in 1957
- H3N2, which caused Hong Kong Flu in 1968
- H5N1, which caused Bird Flu in 2004
- H7N7, which has unusual zoonotic potential[43]
- H1N2, endemic in humans, pigs and birds
- H9N2
- H7N2
- H7N3
- H10N7
- H7N9
Influenzavirus B

This genus has one species, influenza B virus. Influenza B almost exclusively infects humans[42] and is less common than influenza A. The only other animals known to be susceptible to influenza B infection are the seal[44] and the ferret.[45] This type of influenza mutates at a rate 2–3 times slower than type A[46] and consequently is less genetically diverse, with only one influenza B serotype.[42] As a result of this lack of antigenic diversity, a degree of immunity to influenza B is usually acquired at an early age. However, influenza B mutates enough that lasting immunity is not possible.[47] This reduced rate of antigenic change, combined with its limited host range (inhibiting cross species antigenic shift), ensures that pandemics of influenza B do not occur.[48]
Influenzavirus C
This genus has one species, influenza C virus, which infects humans, dogs and pigs, sometimes causing both severe illness and local epidemics.[49][50] However, influenza C is less common than the other types and usually only causes mild disease in children.[51][52]
Structure, properties, and subtype nomenclature
Influenzaviruses A, B and C are very similar in overall structure.[53] The virus particle is 80–120 nanometers in diameter and usually roughly spherical, although filamentous forms can occur.[54][55] These filamentous forms are more common in influenza C, which can form cordlike structures up to 500 micrometers long on the surfaces of infected cells.[56] However, despite these varied shapes, the viral particles of all influenza viruses are similar in composition.[56] These are made of a viral envelope containing two main types of glycoproteins, wrapped around a central core. The central core contains the viral RNA genome and other viral proteins that package and protect this RNA. RNA tends to be single stranded but in special cases it is double.[55] Unusually for a virus, its genome is not a single piece of nucleic acid; instead, it contains seven or eight pieces of segmented negative-sense RNA, each piece of RNA containing either one or two genes, which code for a gene product (protein).[56] For example, the influenza A genome contains 11 genes on eight pieces of RNA, encoding for 11 proteins: hemagglutinin (HA), neuraminidase (NA), nucleoprotein (NP), M1, M2, NS1, NS2 (NEP: nuclear export protein), PA, PB1 (polymerase basic 1), PB1-F2 and PB2.[57]
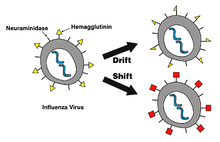
Hemagglutinin (HA) and neuraminidase (NA) are the two large glycoproteins on the outside of the viral particles. HA is a lectin that mediates binding of the virus to target cells and entry of the viral genome into the target cell, while NA is involved in the release of progeny virus from infected cells, by cleaving sugars that bind the mature viral particles.[58] Thus, these proteins are targets for antiviral drugs.[59] Furthermore, they are antigens to which antibodies can be raised. Influenza A viruses are classified into subtypes based on antibody responses to HA and NA. These different types of HA and NA form the basis of the H and N distinctions in, for example, H5N1.[60] There are 16 H and 9 N subtypes known, but only H 1, 2 and 3, and N 1 and 2 are commonly found in humans.[61]
Replication

Viruses can replicate only in living cells.[62] Influenza infection and replication is a multi-step process: First, the virus has to bind to and enter the cell, then deliver its genome to a site where it can produce new copies of viral proteins and RNA, assemble these components into new viral particles, and, last, exit the host cell.[56]
Influenza viruses bind through hemagglutinin onto sialic acid sugars on the surfaces of epithelial cells, typically in the nose, throat, and lungs of mammals, and intestines of birds (Stage 1 in infection figure).[63] After the hemagglutinin is cleaved by a protease, the cell imports the virus by endocytosis.[64]
The intracellular details are still being elucidated. It is known that virions converge to the microtubule organizing center, interact with acidic endosomes and finally enter the target endosomes for genome release.[65]
Once inside the cell, the acidic conditions in the endosome cause two events to happen: First, part of the hemagglutinin protein fuses the viral envelope with the vacuole's membrane, then the M2 ion channel allows protons to move through the viral envelope and acidify the core of the virus, which causes the core to disassemble and release the viral RNA and core proteins.[56] The viral RNA (vRNA) molecules, accessory proteins and RNA-dependent RNA polymerase are then released into the cytoplasm (Stage 2).[66] The M2 ion channel is blocked by amantadine drugs, preventing infection.[67]
These core proteins and vRNA form a complex that is transported into the cell nucleus, where the RNA-dependent RNA polymerase begins transcribing complementary positive-sense vRNA (Steps 3a and b).[68] The vRNA either is exported into the cytoplasm and translated (step 4) or remains in the nucleus. Newly synthesized viral proteins are either secreted through the Golgi apparatus onto the cell surface (in the case of neuraminidase and hemagglutinin, step 5b) or transported back into the nucleus to bind vRNA and form new viral genome particles (step 5a). Other viral proteins have multiple actions in the host cell, including degrading cellular mRNA and using the released nucleotides for vRNA synthesis and also inhibiting translation of host-cell mRNAs.[69]
Negative-sense vRNAs that form the genomes of future viruses, RNA-dependent RNA polymerase, and other viral proteins are assembled into a virion. Hemagglutinin and neuraminidase molecules cluster into a bulge in the cell membrane. The vRNA and viral core proteins leave the nucleus and enter this membrane protrusion (step 6). The mature virus buds off from the cell in a sphere of host phospholipid membrane, acquiring hemagglutinin and neuraminidase with this membrane coat (step 7).[70] As before, the viruses adhere to the cell through hemagglutinin; the mature viruses detach once their neuraminidase has cleaved sialic acid residues from the host cell.[63] After the release of new influenza viruses, the host cell dies.
Because of the absence of RNA proofreading enzymes, the RNA-dependent RNA polymerase that copies the viral genome makes an error roughly every 10 thousand nucleotides, which is the approximate length of the influenza vRNA. Hence, the majority of newly manufactured influenza viruses are mutants; this causes antigenic drift, which is a slow change in the antigens on the viral surface over time.[71] The separation of the genome into eight separate segments of vRNA allows mixing or reassortment of vRNAs if more than one type of influenza virus infects a single cell. The resulting rapid change in viral genetics produces antigenic shifts, which are sudden changes from one antigen to another. These sudden large changes allow the virus to infect new host species and quickly overcome protective immunity.[60] This is important in the emergence of pandemics, as discussed below in the section on Epidemiology.
Mechanism
Transmission
In otherwise healthy adults, influenza virus shedding (the time during which a person might be infectious to another person) increases sharply one-half to one day after infection, peaks on day 2 and persists for an average total duration of 5 days—but can persist as long as 9 days.[72] In those who develop symptoms from experimental infection (only 67% of healthy experimentally infected individuals), symptoms and viral shedding show a similar pattern, but with viral shedding preceding illness by one day.[72] Children are much more infectious than adults and shed virus from just before they develop symptoms until two weeks after infection.[73] In immunocompromised people, viral shedding can continue for longer than two weeks.[74]
Influenza can be spread in three main ways:[75][76] by direct transmission (when an infected person sneezes mucus directly into the eyes, nose or mouth of another person); the airborne route (when someone inhales the aerosols produced by an infected person coughing, sneezing or spitting) and through hand-to-eye, hand-to-nose, or hand-to-mouth transmission, either from contaminated surfaces or from direct personal contact such as a hand-shake. The relative importance of these three modes of transmission is unclear, and they may all contribute to the spread of the virus.[5] In the airborne route, the droplets that are small enough for people to inhale are 0.5 to 5 µm in diameter and inhaling just one droplet might be enough to cause an infection.[75] Although a single sneeze releases up to 40,000 droplets,[77] most of these droplets are quite large and will quickly settle out of the air.[75] How long influenza survives in airborne droplets seems to be influenced by the levels of humidity and UV radiation, with low humidity and a lack of sunlight in winter aiding its survival.[75]
As the influenza virus can persist outside of the body, it can also be transmitted by contaminated surfaces such as banknotes,[78] doorknobs, light switches and other household items.[16] The length of time the virus will persist on a surface varies, with the virus surviving for one to two days on hard, non-porous surfaces such as plastic or metal, for about fifteen minutes from dry paper tissues, and only five minutes on skin.[79] However, if the virus is present in mucus, this can protect it for longer periods (up to 17 days on banknotes).[75][78] Avian influenza viruses can survive indefinitely when frozen.[80] They are inactivated by heating to 56 °C (133 °F) for a minimum of 60 minutes, as well as by acids (at pH <2).[80]
Pathophysiology

The mechanisms by which influenza infection causes symptoms in humans have been studied intensively. One of the mechanisms is believed to be the inhibition of adrenocorticotropic hormone (ACTH) resulting in lowered cortisol levels.[81] Knowing which genes are carried by a particular strain can help predict how well it will infect humans and how severe this infection will be (that is, predict the strain's pathophysiology).[50][82]
For instance, part of the process that allows influenza viruses to invade cells is the cleavage of the viral hemagglutinin protein by any one of several human proteases.[64] In mild and avirulent viruses, the structure of the hemagglutinin means that it can only be cleaved by proteases found in the throat and lungs, so these viruses cannot infect other tissues. However, in highly virulent strains, such as H5N1, the hemagglutinin can be cleaved by a wide variety of proteases, allowing the virus to spread throughout the body.[82]
The viral hemagglutinin protein is responsible for determining both which species a strain can infect and where in the human respiratory tract a strain of influenza will bind.[83] Strains that are easily transmitted between people have hemagglutinin proteins that bind to receptors in the upper part of the respiratory tract, such as in the nose, throat and mouth. In contrast, the highly lethal H5N1 strain binds to receptors that are mostly found deep in the lungs.[84] This difference in the site of infection may be part of the reason why the H5N1 strain causes severe viral pneumonia in the lungs, but is not easily transmitted by people coughing and sneezing.[85][86]
Common symptoms of the flu such as fever, headaches, and fatigue are the result of the huge amounts of proinflammatory cytokines and chemokines (such as interferon or tumor necrosis factor) produced from influenza-infected cells.[21][87] In contrast to the rhinovirus that causes the common cold, influenza does cause tissue damage, so symptoms are not entirely due to the inflammatory response.[88] This massive immune response might produce a life-threatening cytokine storm. This effect has been proposed to be the cause of the unusual lethality of both the H5N1 avian influenza,[89] and the 1918 pandemic strain.[90][91] However, another possibility is that these large amounts of cytokines are just a result of the massive levels of viral replication produced by these strains, and the immune response does not itself contribute to the disease.[92]
Prevention
Vaccination

The influenza vaccine is recommended by the World Health Organization and United States Centers for Disease Control and Prevention for high-risk groups, such as children, the elderly, health care workers, and people who have chronic illnesses such as asthma, diabetes, heart disease, or are immuno-compromised among others.[93][94] In healthy adults it is modestly effective in decreasing the amount of influenza-like symptoms in a population.[95] Evidence is supportive of a decreased rate of influenza in children over the age of two.[96] In those with chronic obstructive pulmonary disease vaccination reduces exacerbations,[97] it is not clear if it reduces asthma exacerbations.[98] Evidence supports a lower rate of influenza-like illness in many groups who are immunocompromised such as those with: HIV/AIDS, cancer, and post organ transplant.[99] In those at high risk immunization may reduce the risk of heart disease.[100] Whether immunizing health care workers affects patient outcomes is controversial with some reviews finding insufficient evidence[101][102] and others finding tentative evidence.[103][104]
Due to the high mutation rate of the virus, a particular influenza vaccine usually confers protection for no more than a few years. Every year, the World Health Organization predicts which strains of the virus are most likely to be circulating in the next year (see Historical annual reformulations of the influenza vaccine), allowing pharmaceutical companies to develop vaccines that will provide the best immunity against these strains.[105] The vaccine is reformulated each season for a few specific flu strains but does not include all the strains active in the world during that season. It takes about six months for the manufacturers to formulate and produce the millions of doses required to deal with the seasonal epidemics; occasionally, a new or overlooked strain becomes prominent during that time.[106] It is also possible to get infected just before vaccination and get sick with the strain that the vaccine is supposed to prevent, as the vaccine takes about two weeks to become effective.[107]
Vaccines can cause the immune system to react as if the body were actually being infected, and general infection symptoms (many cold and flu symptoms are just general infection symptoms) can appear, though these symptoms are usually not as severe or long-lasting as influenza. The most dangerous adverse effect is a severe allergic reaction to either the virus material itself or residues from the hen eggs used to grow the influenza; however, these reactions are extremely rare.[108]
The cost-effectiveness of seasonal influenza vaccination has been widely evaluated for different groups and in different settings.[109] It has generally been found to be a cost-effective intervention, especially in children[110] and the elderly,[111] however the results of economic evaluations of influenza vaccination have often been found to be dependent on key assumptions.[112][113]
Infection control
Reasonably effective ways to reduce the transmission of influenza include good personal health and hygiene habits such as: not touching your eyes, nose or mouth;[114] frequent hand washing (with soap and water, or with alcohol-based hand rubs);[115] covering coughs and sneezes; avoiding close contact with sick people; and staying home yourself if you are sick. Avoiding spitting is also recommended.[116] Although face masks might help prevent transmission when caring for the sick,[117][118] there is mixed evidence on beneficial effects in the community.[116][119] Smoking raises the risk of contracting influenza, as well as producing more severe disease symptoms.[120][121]
Since influenza spreads through both aerosols and contact with contaminated surfaces, surface sanitizing may help prevent some infections.[122] Alcohol is an effective sanitizer against influenza viruses, while quaternary ammonium compounds can be used with alcohol so that the sanitizing effect lasts for longer.[123] In hospitals, quaternary ammonium compounds and bleach are used to sanitize rooms or equipment that have been occupied by patients with influenza symptoms.[123] At home, this can be done effectively with a diluted chlorine bleach.[124]
During past pandemics, closing schools, churches and theaters slowed the spread of the virus but did not have a large effect on the overall death rate.[125][126] It is uncertain if reducing public gatherings, by for example closing schools and workplaces, will reduce transmission since people with influenza may just be moved from one area to another; such measures would also be difficult to enforce and might be unpopular.[116] When small numbers of people are infected, isolating the sick might reduce the risk of transmission.[116]
Treatment
People with the flu are advised to get plenty of rest, drink plenty of liquids, avoid using alcohol and tobacco and, if necessary, take medications such as acetaminophen (paracetamol) to relieve the fever and muscle aches associated with the flu.[127] Children and teenagers with flu symptoms (particularly fever) should avoid taking aspirin during an influenza infection (especially influenza type B), because doing so can lead to Reye's syndrome, a rare but potentially fatal disease of the liver.[128] Since influenza is caused by a virus, antibiotics have no effect on the infection; unless prescribed for secondary infections such as bacterial pneumonia. Antiviral medication may be effective, if given early, but some strains of influenza can show resistance to the standard antiviral drugs and there is concern about the quality of the research.[129]
Antivirals
The two classes of antiviral drugs used against influenza are neuraminidase inhibitors (oseltamivir and zanamivir) and M2 protein inhibitors (adamantane derivatives).
Neuraminidase inhibitors
Overall the benefits of neuraminidase inhibitors in those who are otherwise healthy do not appear to be greater than the risks.[7] There does not appear to be any benefit in those with other health problems.[7] In those believed to have the flu, they decreased the length of time symptoms were present by slightly less than a day but did not appear to affect the risk of complications such as needing hospitalization or pneumonia.[8] Previous to 2013 the benefits were unclear as the manufacturer (Roche) refused to release trial data for independent analysis.[130]
M2 inhibitors
The antiviral drugs amantadine and rimantadine inhibit a viral ion channel (M2 protein), thus inhibiting replication of the influenza A virus.[67] These drugs are sometimes effective against influenza A if given early in the infection but are ineffective against influenza B viruses, which lack the M2 drug target.[131] Measured resistance to amantadine and rimantadine in American isolates of H3N2 has increased to 91% in 2005.[132] This high level of resistance may be due to the easy availability of amantadines as part of over-the-counter cold remedies in countries such as China and Russia,[133] and their use to prevent outbreaks of influenza in farmed poultry.[134][135] The CDC recommended against using M2 inhibitors during the 2005–06 influenza season due to high levels of drug resistance.[136]
Prognosis
Influenza's effects are much more severe and last longer than those of the common cold. Most people will recover completely in about one to two weeks, but others will develop life-threatening complications (such as pneumonia). Thus, influenza can be deadly, especially for the weak, young and old, or chronically ill.[60] People with a weak immune system, such as people with advanced HIV infection or transplant patients (whose immune systems are medically suppressed to prevent transplant organ rejection), suffer from particularly severe disease.[137] Pregnant women and young children are also at a high risk for complications.[138]
The flu can worsen chronic health problems. People with emphysema, chronic bronchitis or asthma may experience shortness of breath while they have the flu, and influenza may cause worsening of coronary heart disease or congestive heart failure.[139] Smoking is another risk factor associated with more serious disease and increased mortality from influenza.[140]
According to the World Health Organization: "Every winter, tens of millions of people get the flu. Most are only ill and out of work for a week, yet the elderly are at a higher risk of death from the illness. We know the worldwide death toll exceeds a few hundred thousand people a year, but even in developed countries the numbers are uncertain, because medical authorities don't usually verify who actually died of influenza and who died of a flu-like illness."[141] Even healthy people can be affected, and serious problems from influenza can happen at any age. People over 50 years old, very young children and people of any age with chronic medical conditions are more likely to get complications from influenza, such as pneumonia, bronchitis, sinus, and ear infections.[107]
In some cases, an autoimmune response to an influenza infection may contribute to the development of Guillain-Barré syndrome.[142] However, as many other infections can increase the risk of this disease, influenza may only be an important cause during epidemics.[142][143] This syndrome has been believed to also be a rare side effect of influenza vaccines. One review gives an incidence of about one case per million vaccinations.[144] Getting infected by influenza itself increases both the risk of death (up to 1 in 10,000) and increases the risk of developing GBS to a much higher level than the highest level of suspected vaccine involvement (approx. 10 times higher by recent estimates).[145][146]
Epidemiology
Seasonal variations
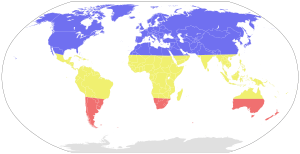
Influenza reaches peak prevalence in winter, and because the Northern and Southern Hemispheres have winter at different times of the year, there are actually two different flu seasons each year. This is why the World Health Organization (assisted by the National Influenza Centers) makes recommendations for two different vaccine formulations every year; one for the Northern, and one for the Southern Hemisphere.[105]
A long-standing puzzle has been why outbreaks of the flu occur seasonally rather than uniformly throughout the year. One possible explanation is that, because people are indoors more often during the winter, they are in close contact more often, and this promotes transmission from person to person. Increased travel due to the Northern Hemisphere winter holiday season may also play a role.[147] Another factor is that cold temperatures lead to drier air, which may dehydrate mucus, preventing the body from effectively expelling virus particles. The virus also survives longer on surfaces at colder temperatures and aerosol transmission of the virus is highest in cold environments (less than 5 °C) with low relative humidity.[148] The lower air humidity in winter seems to be the main cause of seasonal influenza transmission in temperate regions.[149][150]
However, seasonal changes in infection rates also occur in tropical regions, and in some countries these peaks of infection are seen mainly during the rainy season.[151] Seasonal changes in contact rates from school terms, which are a major factor in other childhood diseases such as measles and pertussis, may also play a role in the flu. A combination of these small seasonal effects may be amplified by dynamical resonance with the endogenous disease cycles.[152] H5N1 exhibits seasonality in both humans and birds.[153]
An alternative hypothesis to explain seasonality in influenza infections is an effect of vitamin D levels on immunity to the virus.[154] This idea was first proposed by Robert Edgar Hope-Simpson in 1965.[155] He proposed that the cause of influenza epidemics during winter may be connected to seasonal fluctuations of vitamin D, which is produced in the skin under the influence of solar (or artificial) UV radiation. This could explain why influenza occurs mostly in winter and during the tropical rainy season, when people stay indoors, away from the sun, and their vitamin D levels fall.
Epidemic and pandemic spread
As influenza is caused by a variety of species and strains of viruses, in any given year some strains can die out while others create epidemics, while yet another strain can cause a pandemic. Typically, in a year's normal two flu seasons (one per hemisphere), there are between three and five million cases of severe illness and around 500,000 deaths worldwide,[156] which by some definitions is a yearly influenza epidemic.[157] Although the incidence of influenza can vary widely between years, approximately 36,000 deaths and more than 200,000 hospitalizations are directly associated with influenza every year in the United States.[158][159] One method of calculating influenza mortality produced an estimate of 41,400 average deaths per year in the United States between 1979 and 2001.[160] Different methods in 2010 by the Centers for Disease Control and Prevention (CDC) reported a range from a low of about 3,300 deaths to a high of 49,000 per year.[161]
Roughly three times per century, a pandemic occurs, which infects a large proportion of the world's population and can kill tens of millions of people (see pandemics section). One study estimated that if a strain with similar virulence to the 1918 influenza emerged today, it could kill between 50 and 80 million people.[162]

New influenza viruses are constantly evolving by mutation or by reassortment.[42] Mutations can cause small changes in the hemagglutinin and neuraminidase antigens on the surface of the virus. This is called antigenic drift, which slowly creates an increasing variety of strains until one evolves that can infect people who are immune to the pre-existing strains. This new variant then replaces the older strains as it rapidly sweeps through the human population, often causing an epidemic.[163] However, since the strains produced by drift will still be reasonably similar to the older strains, some people will still be immune to them. In contrast, when influenza viruses reassort, they acquire completely new antigens—for example by reassortment between avian strains and human strains; this is called antigenic shift. If a human influenza virus is produced that has entirely new antigens, everybody will be susceptible, and the novel influenza will spread uncontrollably, causing a pandemic.[164] In contrast to this model of pandemics based on antigenic drift and shift, an alternative approach has been proposed where the periodic pandemics are produced by interactions of a fixed set of viral strains with a human population with a constantly changing set of immunities to different viral strains.[165]

From a public health point of view, flu epidemics spread rapidly and are very difficult to control. Most influenza virus strains are not very infectious and each infected individual will only go on to infect one or two other individuals (the basic reproduction number for influenza is generally around 1.4). However, the generation time for influenza is extremely short: the time from a person becoming infected to when he infects the next person is only two days. The short generation time means that influenza epidemics generally peak at around 2 months and burn out after 3 months: the decision to intervene in an influenza epidemic therefore has to be taken early, and the decision is therefore often made on the back of incomplete data. Another problem is that individuals become infectious before they become symptomatic, which means that putting people in quarantine after they become ill is not an effective public health intervention.[166] For the average person, viral shedding tends to peak on day two whereas symptoms peak on day three.[14]
History
Etymology
The word Influenza comes from the Italian language meaning "influence" and refers to the cause of the disease; initially, this ascribed illness to unfavorable astrological influences.[167] Changes in medical thought led to its modification to influenza del freddo, meaning "influence of the cold". The word influenza was first used in English to refer to the disease we know today in 1703 by J. Hugger of the University of Edinburgh in his thesis De Catarrho epidemio, vel Influenza, prout in India occidentali sese ostendit.[168] Archaic terms for influenza include epidemic catarrh, grippe (from the French, first used by Molyneaux in 1694 [169]), sweating sickness, and Spanish fever (particularly for the 1918 flu pandemic strain).[170]
Pandemics


The symptoms of human influenza were clearly described by Hippocrates roughly 2,400 years ago.[172][173] Although the virus seems to have caused epidemics throughout human history, historical data on influenza are difficult to interpret, because the symptoms can be similar to those of other respiratory diseases.[174][175] The disease may have spread from Europe to the Americas as early as the European colonization of the Americas; since almost the entire indigenous population of the Antilles was killed by an epidemic resembling influenza that broke out in 1493, after the arrival of Christopher Columbus.[176][177]
The first convincing record of an influenza pandemic was of an outbreak in 1580, which began in Russia and spread to Europe via Africa. In Rome, over 8,000 people were killed, and several Spanish cities were almost wiped out. Pandemics continued sporadically throughout the 17th and 18th centuries, with the pandemic of 1830–1833 being particularly widespread; it infected approximately a quarter of the people exposed.[175]
The most famous and lethal outbreak was the 1918 flu pandemic (Spanish flu pandemic) (type A influenza, H1N1 subtype), which lasted from 1918 to 1919. It is not known exactly how many it killed, but estimates range from 50 to 100 million people.[171][178][179] This pandemic has been described as "the greatest medical holocaust in history" and may have killed as many people as the Black Death.[175] This huge death toll was caused by an extremely high infection rate of up to 50% and the extreme severity of the symptoms, suspected to be caused by cytokine storms.[179] Symptoms in 1918 were so unusual that initially influenza was misdiagnosed as dengue, cholera, or typhoid. One observer wrote, "One of the most striking of the complications was hemorrhage from mucous membranes, especially from the nose, stomach, and intestine. Bleeding from the ears and petechial hemorrhages in the skin also occurred."[178] The majority of deaths were from bacterial pneumonia, a secondary infection caused by influenza, but the virus also killed people directly, causing massive hemorrhages and edema in the lung.[180]
The 1918 flu pandemic (Spanish flu pandemic) was truly global, spreading even to the Arctic and remote Pacific islands. The unusually severe disease killed between 2 and 20% of those infected, as opposed to the more usual flu epidemic mortality rate of 0.1%.[171][178] Another unusual feature of this pandemic was that it mostly killed young adults, with 99% of pandemic influenza deaths occurring in people under 65, and more than half in young adults 20 to 40 years old.[181] This is unusual since influenza is normally most deadly to the very young (under age 2) and the very old (over age 70). The total mortality of the 1918–1919 pandemic is not known, but it is estimated that 2.5% to 5% of the world's population was killed. As many as 25 million may have been killed in the first 25 weeks; in contrast, HIV/AIDS has killed 25 million in its first 25 years.[178]
Later flu pandemics were not so devastating. They included the 1957 Asian Flu (type A, H2N2 strain) and the 1968 Hong Kong Flu (type A, H3N2 strain), but even these smaller outbreaks killed millions of people. In later pandemics antibiotics were available to control secondary infections and this may have helped reduce mortality compared to the Spanish Flu of 1918.[171]
| Name of pandemic | Date | Deaths | Case fatality rate | Subtype involved | Pandemic Severity Index |
|---|---|---|---|---|---|
| 1889–1890 flu pandemic (Asiatic or Russian Flu)[182] |
1889–1890 | 1 million | 0.15% | possibly H3N8 or H2N2 | N/A |
| 1918 flu pandemic (Spanish flu)[183] |
1918–1920 | 20 to 100 million | 2% | H1N1 | 5 |
| Asian Flu | 1957–1958 | 1 to 1.5 million | 0.13% | H2N2 | 2 |
| Hong Kong Flu | 1968–1969 | 0.75 to 1 million | <0.1% | H3N2 | 2 |
| Russian flu | 1977–1978 | no accurate count | N/A | H1N1 | N/A |
| 2009 flu pandemic[184] | 2009–2010 | 105,700-395,600[185] | 0.03% | H1N1 | N/A |
The first influenza virus to be isolated was from poultry, when in 1901 the agent causing a disease called "fowl plague" was passed through Chamberland filters, which have pores that are too small for bacteria to pass through.[186] The etiological cause of influenza, the Orthomyxoviridae family of viruses, was first discovered in pigs by Richard Shope in 1931.[187] This discovery was shortly followed by the isolation of the virus from humans by a group headed by Patrick Laidlaw at the Medical Research Council of the United Kingdom in 1933.[188] However, it was not until Wendell Stanley first crystallized tobacco mosaic virus in 1935 that the non-cellular nature of viruses was appreciated.

The first significant step towards preventing influenza was the development in 1944 of a killed-virus vaccine for influenza by Thomas Francis, Jr.. This built on work by Australian Frank Macfarlane Burnet, who showed that the virus lost virulence when it was cultured in fertilized hen's eggs.[190] Application of this observation by Francis allowed his group of researchers at the University of Michigan to develop the first influenza vaccine, with support from the U.S. Army.[191] The Army was deeply involved in this research due to its experience of influenza in World War I, when thousands of troops were killed by the virus in a matter of months.[178] In comparison to vaccines, the development of anti-influenza drugs has been slower, with amantadine being licensed in 1966 and, almost thirty years later, the next class of drugs (the neuraminidase inhibitors) being developed.[61]
Society and culture
Influenza produces direct costs due to lost productivity and associated medical treatment, as well as indirect costs of preventative measures. In the United States, influenza is responsible for a total cost of over $10 billion per year, while it has been estimated that a future pandemic could cause hundreds of billions of dollars in direct and indirect costs.[192] However, the economic impacts of past pandemics have not been intensively studied, and some authors have suggested that the Spanish influenza actually had a positive long-term effect on per-capita income growth, despite a large reduction in the working population and severe short-term depressive effects.[193] Other studies have attempted to predict the costs of a pandemic as serious as the 1918 Spanish flu on the U.S. economy, where 30% of all workers became ill, and 2.5% were killed. A 30% sickness rate and a three-week length of illness would decrease the gross domestic product by 5%. Additional costs would come from medical treatment of 18 million to 45 million people, and total economic costs would be approximately $700 billion.[194]
Preventative costs are also high. Governments worldwide have spent billions of U.S. dollars preparing and planning for a potential H5N1 avian influenza pandemic, with costs associated with purchasing drugs and vaccines as well as developing disaster drills and strategies for improved border controls.[195] On 1 November 2005, United States President George W. Bush unveiled the National Strategy to Safeguard Against the Danger of Pandemic Influenza[196] backed by a request to Congress for $7.1 billion to begin implementing the plan.[197] Internationally, on 18 January 2006, donor nations pledged US$2 billion to combat bird flu at the two-day International Pledging Conference on Avian and Human Influenza held in China.[198]
In an assessment of the 2009 H1N1 pandemic on selected countries in the Southern Hemisphere, data suggest that all countries experienced some time-limited and/or geographically isolated socio/economic effects and a temporary decrease in tourism most likely due to fear of 2009 H1N1 disease. It is still too early to determine whether the H1N1 pandemic has caused any long-term economic impacts.[199]
Research

Research on influenza includes studies on molecular virology, how the virus produces disease (pathogenesis), host immune responses, viral genomics, and how the virus spreads (epidemiology). These studies help in developing influenza countermeasures; for example, a better understanding of the body's immune system response helps vaccine development, and a detailed picture of how influenza invades cells aids the development of antiviral drugs. One important basic research program is the Influenza Genome Sequencing Project, which is creating a library of influenza sequences; this library should help clarify which factors make one strain more lethal than another, which genes most affect immunogenicity, and how the virus evolves over time.[200]
Research into new vaccines is particularly important, as current vaccines are very slow and expensive to produce and must be reformulated every year. The sequencing of the influenza genome and recombinant DNA technology may accelerate the generation of new vaccine strains by allowing scientists to substitute new antigens into a previously developed vaccine strain.[201] New technologies are also being developed to grow viruses in cell culture, which promises higher yields, less cost, better quality and surge capacity.[202] Research on a universal influenza A vaccine, targeted against the external domain of the transmembrane viral M2 protein (M2e), is being done at the University of Ghent by Walter Fiers, Xavier Saelens and their team[203][204][205] and has now successfully concluded Phase I clinical trials. There has been some research success towards a "universal flu vaccine" that produces antibodies against proteins on the viral coat which mutate less rapidly, and thus a single shot could potentially provide longer-lasting protection.[206][207][208]
A number of biologics, therapeutic vaccines and immunobiologics are also being investigated for treatment of infection caused by viruses. Therapeutic biologics are designed to activate the immune response to virus or antigens. Typically, biologics do not target metabolic pathways like anti-viral drugs, but stimulate immune cells such as lymphocytes, macrophages, and/or antigen presenting cells, in an effort to drive an immune response towards a cytotoxic effect against the virus. Influenza models, such as murine influenza, are convenient models to test the effects of prophylactic and therapeutic biologics. For example, Lymphocyte T-Cell Immune Modulator inhibits viral growth in the murine model of influenza.[209]
Other animals
Influenza infects many animal species, and transfer of viral strains between species can occur. Birds are thought to be the main animal reservoirs of influenza viruses.[210] Sixteen forms of hemagglutinin and nine forms of neuraminidase have been identified. All known subtypes (HxNy) are found in birds, but many subtypes are endemic in humans, dogs, horses, and pigs; populations of camels, ferrets, cats, seals, mink, and whales also show evidence of prior infection or exposure to influenza.[47] Variants of flu virus are sometimes named according to the species the strain is endemic in or adapted to. The main variants named using this convention are: bird flu, human flu, swine flu, horse flu and dog flu. (Cat flu generally refers to feline viral rhinotracheitis or feline calicivirus and not infection from an influenza virus.) In pigs, horses and dogs, influenza symptoms are similar to humans, with cough, fever and loss of appetite.[47] The frequency of animal diseases are not as well-studied as human infection, but an outbreak of influenza in harbor seals caused approximately 500 seal deaths off the New England coast in 1979–1980.[211] However, outbreaks in pigs are common and do not cause severe mortality.[47] Vaccines have also been developed to protect poultry from avian influenza. These vaccines can be effective against multiple strains and are used either as part of a preventative strategy, or combined with culling in attempts to eradicate outbreaks.[212]
Bird flu
Flu symptoms in birds are variable and can be unspecific.[213] The symptoms following infection with low-pathogenicity avian influenza may be as mild as ruffled feathers, a small reduction in egg production, or weight loss combined with minor respiratory disease.[214] Since these mild symptoms can make diagnosis in the field difficult, tracking the spread of avian influenza requires laboratory testing of samples from infected birds. Some strains such as Asian H9N2 are highly virulent to poultry and may cause more extreme symptoms and significant mortality.[215] In its most highly pathogenic form, influenza in chickens and turkeys produces a sudden appearance of severe symptoms and almost 100% mortality within two days.[216] As the virus spreads rapidly in the crowded conditions seen in the intensive farming of chickens and turkeys, these outbreaks can cause large economic losses to poultry farmers.
An avian-adapted, highly pathogenic strain of H5N1 (called HPAI A(H5N1), for "highly pathogenic avian influenza virus of type A of subtype H5N1") causes H5N1 flu, commonly known as "avian influenza" or simply "bird flu", and is endemic in many bird populations, especially in Southeast Asia. This Asian lineage strain of HPAI A(H5N1) is spreading globally. It is epizootic (an epidemic in non-humans) and panzootic (a disease affecting animals of many species, especially over a wide area), killing tens of millions of birds and spurring the culling of hundreds of millions of other birds in an attempt to control its spread. Most references in the media to "bird flu" and most references to H5N1 are about this specific strain.[217][218]
At present, HPAI A(H5N1) is an avian disease, and there is no evidence suggesting efficient human-to-human transmission of HPAI A(H5N1). In almost all cases, those infected have had extensive physical contact with infected birds.[219] In the future, H5N1 may mutate or reassort into a strain capable of efficient human-to-human transmission. The exact changes that are required for this to happen are not well understood.[220] However, due to the high lethality and virulence of H5N1, its endemic presence, and its large and increasing biological host reservoir, the H5N1 virus was the world's pandemic threat in the 2006–07 flu season, and billions of dollars are being raised and spent researching H5N1 and preparing for a potential influenza pandemic.[195]

In March 2013, the Chinese government reported three cases of H7N9 influenza infections in humans. Two of whom had died and the third was critically ill. Although the strain of the virus is not thought to spread efficiently between humans,[221][222] by mid-April, at least 82 persons had become ill from H7N9, of which 17 had died. These cases include three small family clusters in Shanghai and one cluster between a neighboring girl and boy in Beijing, raising at least the possibility of human-to-human transmission. WHO points out that one cluster did not have two of the cases lab confirmed and further points out, as a matter of baseline information, that some viruses are able to cause limited human-to-human transmission under conditions of close contact but are not transmissible enough to cause large community outbreaks.[223][224]
Swine flu
In pigs swine influenza produces fever, lethargy, sneezing, coughing, difficulty breathing and decreased appetite.[225] In some cases the infection can cause abortion. Although mortality is usually low, the virus can produce weight loss and poor growth, causing economic loss to farmers.[225] Infected pigs can lose up to 12 pounds of body weight over a 3- to 4-week period.[225] Direct transmission of an influenza virus from pigs to humans is occasionally possible (this is called zoonotic swine flu). In all, 50 human cases are known to have occurred since the virus was identified in the mid-20th century, which have resulted in six deaths.[226]
In 2009, a swine-origin H1N1 virus strain commonly referred to as "swine flu" caused the 2009 flu pandemic, but there is no evidence that it is endemic to pigs (i.e. actually a swine flu) or of transmission from pigs to people, instead the virus is spreading from person to person.[227][228] This strain is a reassortment of several strains of H1N1 that are usually found separately, in humans, birds, and pigs.[229]
References
- 1 2 3 4 5 6 7 8 "Influenza (Seasonal) Fact sheet N°211". who.int. March 2014. Retrieved 25 November 2014.
- 1 2 3 4 "Key Facts about Influenza (Flu) & Flu Vaccine". cdc.gov. September 9, 2014. Retrieved 26 November 2014.
- ↑ Duben-Engelkirk, Paul G. Engelkirk, Janet (2011). Burton's microbiology for the health sciences (9th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 314. ISBN 9781605476735.
- 1 2 3 4 Longo, Dan L. (2012). "187: Influenza". Harrison's principles of internal medicine. (18th ed.). New York: McGraw-Hill. ISBN 9780071748896.
- 1 2 3 Brankston G, Gitterman L, Hirji Z, Lemieux C, Gardam M (April 2007). "Transmission of influenza A in human beings". Lancet Infect Dis 7 (4): 257–65. doi:10.1016/S1473-3099(07)70029-4. PMID 17376383.
- 1 2 Jefferson T, Del Mar CB, Dooley L, et al. (2011). "Physical interventions to interrupt or reduce the spread of respiratory viruses". Cochrane Database Syst Rev (7): CD006207. doi:10.1002/14651858.CD006207.pub4. PMID 21735402.
- 1 2 3 4 Michiels, B; Van Puyenbroeck, K; Verhoeven, V; Vermeire, E; Coenen, S (2013). "The value of neuraminidase inhibitors for the prevention and treatment of seasonal influenza: a systematic review of systematic reviews.". PLoS ONE 8 (4): e60348. doi:10.1371/journal.pone.0060348. PMC 3614893. PMID 23565231.
- 1 2 Ebell, MH; Call, M; Shinholser, J (April 2013). "Effectiveness of oseltamivir in adults: a meta-analysis of published and unpublished clinical trials.". Family practice 30 (2): 125–33. doi:10.1093/fampra/cms059. PMID 22997224.
- 1 2 "Ten things you need to know about pandemic influenza". World Health Organization. 14 October 2005. Archived from the original on 23 September 2009. Retrieved 26 September 2009.
- ↑ World Health Organization. World now at the start of 2009 influenza pandemic. http://www.who.int/mediacentre/news/statements/2009/h1n1_pandemic_phase6_20090611/en/index.html
- ↑ Palmer, S. R. (2011). Oxford textbook of zoonoses : biology, clinical practice, and public health control (2. ed.). Oxford u.a.: Oxford Univ. Press. p. 332. ISBN 9780198570028.
- 1 2 3 4 Call S, Vollenweider M, Hornung C, Simel D, McKinney W (2005). "Does this patient have influenza?". JAMA 293 (8): 987–97. doi:10.1001/jama.293.8.987. PMID 15728170.
- ↑ Centers for Disease Control and Prevention > Influenza Symptoms Page last updated 16 November 2007. Retrieved 28 April 2009.
- 1 2 Time Lines of Infection and Disease in Human Influenza: A Review of Volunteer Challenge Studies, American Journal of Epidemiology, Carrat, Vergu, Ferguson, et al., 167 (7): 775–785, 2008. "... In almost all studies, participants were individually confined for 1 week ..." See especially Figure 5 which shows that virus shedding tends to peak on day 2 whereas symptoms tend to peak on day 3.
- ↑ Suzuki E, Ichihara K, Johnson AM (January 2007). "Natural course of fever during influenza virus infection in children". Clin Pediatr (Phila) 46 (1): 76–9. doi:10.1177/0009922806289588. PMID 17164515.
- 1 2 "Influenza: Viral Infections: Merck Manual Home Edition". Merck. Retrieved 15 March 2008.
- ↑ Silva ME, Cherry JD, Wilton RJ, Ghafouri NM, Bruckner DA, Miller MJ (August 1999). "Acute fever and petechial rash associated with influenza A virus infection". Clinical Infectious Diseases : an Official Publication of the Infectious Diseases Society of America 29 (2): 453–4. doi:10.1086/520240. PMID 10476766.
- 1 2 Richards S (2005). "Flu blues". Nurs Stand 20 (8): 26–7. PMID 16295596.
- ↑ Heikkinen T (July 2006). "Influenza in children". Acta Paediatr. 95 (7): 778–84. doi:10.1080/08035250600612272. PMID 16801171.
- ↑ Kerr AA, McQuillin J, Downham MA, Gardner PS (1975). "Gastric 'flu influenza B causing abdominal symptoms in children". Lancet 1 (7902): 291–5. doi:10.1016/S0140-6736(75)91205-2. PMID 46444.
- 1 2 Eccles, R (2005). "Understanding the symptoms of the common cold and influenza". Lancet Infect Dis 5 (11): 718–25. doi:10.1016/S1473-3099(05)70270-X. PMID 16253889.
- ↑ Hui DS (March 2008). "Review of clinical symptoms and spectrum in humans with influenza A/H5N1 infection". Respirology. 13 Suppl 1: S10–3. doi:10.1111/j.1440-1843.2008.01247.x. PMID 18366521.
- ↑ Monto A, Gravenstein S, Elliott M, Colopy M, Schweinle J (2000). "Clinical signs and symptoms predicting influenza infection" (PDF). Arch Intern Med 160 (21): 3243–7. doi:10.1001/archinte.160.21.3243. PMID 11088084.
- ↑ Smith K, Roberts M (2002). "Cost-effectiveness of newer treatment strategies for influenza". Am J Med 113 (4): 300–7. doi:10.1016/S0002-9343(02)01222-6. PMID 12361816.
- 1 2 3 4 Rothberg M, Bellantonio S, Rose D (2 September 2003). "Management of influenza in adults older than 65 years of age: cost-effectiveness of rapid testing and antiviral therapy" (PDF). Annals of Internal Medicine 139 (5 Pt 1): 321–9. doi:10.7326/0003-4819-139-5_part_1-200309020-00007. PMID 12965940.
- ↑ Centers for Disease Control and Prevention. Lab Diagnosis of Influenza. Retrieved 1 May 2009
- ↑ "Rapid Diagnostic Testing for Influenza: Information for Clinical Laboratory Directors". Centers for Disease Control and Prevention. 13 October 2015. Retrieved 2 February 2016.
- ↑ Hospitalized Patients with 2009 H1N1 Influenza in the United States, April–June 2009, New England Journal of Medicine, Jain, Kamimoto, et al., 12 November 2009.
- ↑ Transcript of virtual press conference with Gregory Hartl, Spokesperson for H1N1, and Dr Nikki Shindo, Medical Officer, Global Influenza Programme, World Health Organization, 12 November 2009.
- ↑ Report Finds Swine Flu Has Killed 36 Children, New York Times, DENISE GRADY, 3 September 2009.
- ↑ Kawaoka Y (editor) (2006). Influenza Virology: Current Topics. Caister Academic Press. ISBN 978-1-904455-06-6.
- ↑ Vainionpää R, Hyypiä T (April 1994). "Biology of parainfluenza viruses". Clin. Microbiol. Rev. 7 (2): 265–75. doi:10.1128/CMR.7.2.265. PMC 358320. PMID 8055470.
- ↑ Hall CB (June 2001). "Respiratory syncytial virus and parainfluenza virus". N. Engl. J. Med. 344 (25): 1917–28. doi:10.1056/NEJM200106213442507. PMID 11419430.
- ↑ Hause BM, Collin EA, Liu R, Huang B, Sheng Z, Lu W, Wang D, Nelson EA, Li F (2014). "Characterization of a novel influenza virus in cattle and swine: proposal for a new genus in the Orthomyxoviridae family". MBio 5 (2): e00031–14. doi:10.1128/mBio.00031-14.
- ↑ Collin EA, Sheng Z, Lang Y, Ma W, Hause BM, Li F (2015). "Cocirculation of two distinct genetic and antigenic lineages of proposed influenza D virus in cattle". J Virol 89 (2): 1036–1042. doi:10.1128/JVI.02718-14.
- ↑ Ducatez MF, Pelletier C, Meyer G (2015). "Influenza D virus in cattle, France, 2011-2014". Emerg Infect Dis 21 (2): 368–371. doi:10.3201/eid2102.141449.
- ↑ Song H, Qi J, Khedri Z, Diaz S, Yu H, Chen X, Varki A, Shi Y, Gao GF (2016). "An open receptor-binding cavity of hemagglutinin-esterase-fusion glycoprotein from newly-identified Influenza D Virus: Basis for its broad cell tropism". PLoS Pathog 12 (1): e1005411. doi:10.1371/journal.ppat.1005411.
- ↑ Sheng Z, Ran Z, Wang D, Hoppe AD, Simonson R, Chakravarty S, Hause BM, Li F (2014). "Genomic and evolutionary characterization of a novel influenza-C-like virus from swine". Arch Virol 159 (2): 249–255. doi:10.1007/s00705-013-1815-3.
- ↑ Quast M, Sreenivasan C, Sexton G, Nedland H, Singrey A, Fawcett L, Miller G, Lauer D, Voss S, Pollock S, Cunha CW4, Christopher-Hennings J, Nelson E, Li F (2015) Serological evidence for the presence of influenza D virus in small ruminants. Vet Microbiol 180(3-4):281-285. doi:10.1016/j.vetmic.2015.09.005
- ↑ Smith DB, Gaunt ER, Digard P, Templeton K, Simmonds P (2016). "Detection of influenza C virus but not influenza D virus in Scottish respiratory samples". J Clin Virol 74: 50–53. doi:10.1016/j.jcv.2015.11.036.
- ↑ Klenk, Hans-Dieter; Matrosovich, Mikhail; Stech, Jürgen (2008). "Avian Influenza: Molecular Mechanisms of Pathogenesis and Host Range". Animal Viruses: Molecular Biology. Caister Academic Press. ISBN 978-1-904455-22-6.
- 1 2 3 4 Hay, A; Gregory V; Douglas A; Lin Y (29 December 2001). "The evolution of human influenza viruses". Philosophical Transactions of the Royal Society B 356 (1416): 1861–70. doi:10.1098/rstb.2001.0999. PMC 1088562. PMID 11779385.
- ↑ Fouchier, RAM; Schneeberger, PM; Rozendaal, FW; Broekman, JM; Kemink, SA; Munster, V; Kuiken, T; Rimmelzwaan, GF; et al. (2004). "Avian influenza A virus (H7N7) associated with human conjunctivitis and a fatal case of acute respiratory distress syndrome" (PDF). Proceedings of the National Academy of Sciences 101 (5): 1356–61. Bibcode:2004PNAS..101.1356F. doi:10.1073/pnas.0308352100. PMC 337057. PMID 14745020.
- ↑ Osterhaus, A; Rimmelzwaan G; Martina B; Bestebroer T; Fouchier R (2000). "Influenza B virus in seals". Science 288 (5468): 1051–3. Bibcode:2000Sci...288.1051O. doi:10.1126/science.288.5468.1051. PMID 10807575.
- ↑ Jakeman KJ, Tisdale M, Russell S, Leone A, Sweet C (August 1994). "Efficacy of 2'-deoxy-2'-fluororibosides against influenza A and B viruses in ferrets". Antimicrob. Agents Chemother. 38 (8): 1864–7. doi:10.1128/aac.38.8.1864. PMC 284652. PMID 7986023.
- ↑ Nobusawa, E; Sato K (April 2006). "Comparison of the mutation rates of human influenza A and B viruses". J Virol 80 (7): 3675–8. doi:10.1128/JVI.80.7.3675-3678.2006. PMC 1440390. PMID 16537638.
- 1 2 3 4 R, Webster; Bean W; Gorman O; Chambers T; Kawaoka Y (1992). "Evolution and ecology of influenza A viruses". Microbiol Rev 56 (1): 152–79. PMC 372859. PMID 1579108.
- ↑ Zambon, M (November 1999). "Epidemiology and pathogenesis of influenza" (PDF). J Antimicrob Chemother. 44 Suppl B (90002): 3–9. doi:10.1093/jac/44.suppl_2.3. PMID 10877456.
- ↑ Matsuzaki, Y; Sugawara K; Mizuta K; Tsuchiya E; Muraki Y; Hongo S; Suzuki H; Nakamura K (2002). "Antigenic and genetic characterization of influenza C viruses which caused two outbreaks in Yamagata City, Japan, in 1996 and 1998". J Clin Microbiol 40 (2): 422–9. doi:10.1128/JCM.40.2.422-429.2002. PMC 153379. PMID 11825952.
- 1 2 Taubenberger, JK; Morens, DM (2008). "The pathology of influenza virus infections". Annu Rev Pathol 3: 499–522. doi:10.1146/annurev.pathmechdis.3.121806.154316. PMC 2504709. PMID 18039138.
- ↑ Matsuzaki, Y; Katsushima N; Nagai Y; Shoji M; Itagaki T; Sakamoto M; Kitaoka S; Mizuta K; Nishimura H (1 May 2006). "Clinical features of influenza C virus infection in children". J Infect Dis 193 (9): 1229–35. doi:10.1086/502973. PMID 16586359.
- ↑ Katagiri, S; Ohizumi A; Homma M (July 1983). "An outbreak of type C influenza in a children's home". J Infect Dis 148 (1): 51–6. doi:10.1093/infdis/148.1.51. PMID 6309999.
- ↑ International Committee on Taxonomy of Viruses descriptions of:Orthomyxoviridae,Influenzavirus B and Influenzavirus C Archived 2 October 2006 at the Wayback Machine
- ↑ International Committee on Taxonomy of Viruses. "The Universal Virus Database, version 4: Influenza A". Archived from the original on 14 October 2006.
- 1 2 Lamb RA, Choppin PW (1983). "The gene structure and replication of influenza virus". Annu. Rev. Biochem. 52: 467–506. doi:10.1146/annurev.bi.52.070183.002343. PMID 6351727.
- 1 2 3 4 5 Bouvier NM, Palese P (September 2008). "The biology of influenza viruses". Vaccine. 26 Suppl 4: D49–53. doi:10.1016/j.vaccine.2008.07.039. PMC 3074182. PMID 19230160.
- ↑ Ghedin, E; Sengamalay, NA; Shumway, M; Zaborsky, J; Feldblyum, T; Subbu, V; Spiro, DJ; Sitz, J; et al. (October 2005). "Large-scale sequencing of human influenza reveals the dynamic nature of viral genome evolution". Nature 437 (7062): 1162–6. Bibcode:2005Natur.437.1162G. doi:10.1038/nature04239. PMID 16208317.
- ↑ Suzuki, Y (2005). "Sialobiology of influenza: molecular mechanism of host range variation of influenza viruses". Biol Pharm Bull 28 (3): 399–408. doi:10.1248/bpb.28.399. PMID 15744059.
- ↑ Wilson, J; von Itzstein M (July 2003). "Recent strategies in the search for new anti-influenza therapies". Curr Drug Targets 4 (5): 389–408. doi:10.2174/1389450033491019. PMID 12816348.
- 1 2 3 4 Hilleman, M (19 August 2002). "Realities and enigmas of human viral influenza: pathogenesis, epidemiology and control". Vaccine 20 (25–26): 3068–87. doi:10.1016/S0264-410X(02)00254-2. PMID 12163258.
- 1 2 Lynch JP, Walsh EE (April 2007). "Influenza: evolving strategies in treatment and prevention". Semin Respir Crit Care Med 28 (2): 144–58. doi:10.1055/s-2007-976487. PMID 17458769.
- ↑ Smith AE, Helenius A (April 2004). "How viruses enter animal cells". Science 304 (5668): 237–42. Bibcode:2004Sci...304..237S. doi:10.1126/science.1094823. PMID 15073366.
- 1 2 Wagner, R; Matrosovich M; Klenk H (May–June 2002). "Functional balance between haemagglutinin and neuraminidase in influenza virus infections". Rev Med Virol 12 (3): 159–66. doi:10.1002/rmv.352. PMID 11987141.
- 1 2 Steinhauer DA (May 1999). "Role of hemagglutinin cleavage for the pathogenicity of influenza virus". Virology 258 (1): 1–20. doi:10.1006/viro.1999.9716. PMID 10329563.
- ↑ Liu SL, Zhang ZL, Tian ZQ, Zhao HS, Liu H, Sun EZ, Xiao GF, Zhang W, Wang HZ, Pang DW (2011) Effectively and efficiently dissecting the infection of influenza virus by quantum dot-based single-particle tracking. ACS Nano
- ↑ Lakadamyali, M; Rust M; Babcock H; Zhuang X (5 August 2003). "Visualizing infection of individual influenza viruses". Proc Natl Acad Sci USA 100 (16): 9280–5. Bibcode:2003PNAS..100.9280L. doi:10.1073/pnas.0832269100. PMC 170909. PMID 12883000.
- 1 2 Pinto LH, Lamb RA (April 2006). "The M2 proton channels of influenza A and B viruses". J. Biol. Chem. 281 (14): 8997–9000. doi:10.1074/jbc.R500020200. PMID 16407184.
- ↑ Cros, J; Palese P (September 2003). "Trafficking of viral genomic RNA into and out of the nucleus: influenza, Thogoto and Borna disease viruses". Virus Res 95 (1–2): 3–12. doi:10.1016/S0168-1702(03)00159-X. PMID 12921991.
- ↑ Kash, J; Goodman A; Korth M; Katze M (July 2006). "Hijacking of the host-cell response and translational control during influenza virus infection". Virus Res 119 (1): 111–20. doi:10.1016/j.virusres.2005.10.013. PMID 16630668.
- ↑ Nayak, D; Hui E; Barman S (December 2004). "Assembly and budding of influenza virus". Virus Res 106 (2): 147–65. doi:10.1016/j.virusres.2004.08.012. PMID 15567494.
- ↑ Drake, J (1 May 1993). "Rates of spontaneous mutation among RNA viruses". Proc Natl Acad Sci USA 90 (9): 4171–5. Bibcode:1993PNAS...90.4171D. doi:10.1073/pnas.90.9.4171. PMC 46468. PMID 8387212.
- 1 2 Carrat, F.; Vergu, E.; Ferguson, N. M.; Lemaitre, M.; Cauchemez, S.; Leach, S.; Valleron, A.-J. (14 March 2008). "Time Lines of Infection and Disease in Human Influenza: A Review of Volunteer Challenge Studies". American Journal of Epidemiology 167 (7): 775–785. doi:10.1093/aje/kwm375.
- ↑ Mitamura K, Sugaya N (2006). "[Diagnosis and Treatment of influenza—clinical investigation on viral shedding in children with influenza]". Uirusu 56 (1): 109–16. doi:10.2222/jsv.56.109. PMID 17038819.
- ↑ Gooskens, Jairo; Jonges, Marcel; Claas, Eric C. J.; Meijer, Adam; Kroes, Aloys C. M. (15 May 2009). "Prolonged Influenza Virus Infection during Lymphocytopenia and Frequent Detection of Drug‐Resistant Viruses". The Journal of Infectious Diseases 199 (10): 1435–1441. doi:10.1086/598684.
- 1 2 3 4 5 Weber TP, Stilianakis NI (November 2008). "Inactivation of influenza A viruses in the environment and modes of transmission: a critical review". J. Infect. 57 (5): 361–73. doi:10.1016/j.jinf.2008.08.013. PMID 18848358.
- ↑ Hall CB (August 2007). "The spread of influenza and other respiratory viruses: complexities and conjectures" (PDF). Clin. Infect. Dis. 45 (3): 353–9. doi:10.1086/519433. PMID 17599315.
- ↑ Cole E, Cook C (1998). "Characterization of infectious aerosols in health care facilities: an aid to effective engineering controls and preventive strategies". Am J Infect Control 26 (4): 453–64. doi:10.1016/S0196-6553(98)70046-X. PMID 9721404.
- 1 2 Thomas Y, Vogel G, Wunderli W, et al. (May 2008). "Survival of influenza virus on banknotes". Appl. Environ. Microbiol. 74 (10): 3002–7. doi:10.1128/AEM.00076-08. PMC 2394922. PMID 18359825.
- ↑ Bean B, Moore BM, Sterner B, Peterson LR, Gerding DN, Balfour HH (July 1982). "Survival of influenza viruses on environmental surfaces". J. Infect. Dis. 146 (1): 47–51. doi:10.1093/infdis/146.1.47. PMID 6282993.
- 1 2 "Influenza Factsheet" (PDF). Center for Food Security and Public Health, Iowa State University. p. 7
- ↑ Jefferies WM, Turner JC, Lobo M, Gwaltney JM Jr (1998). "Low plasma levels of adrenocorticotropic hormone in patients with acute influenza" (PDF). Clin Infect Dis. 26 (3): 708–10. doi:10.1086/514594. PMID 9524849.
- 1 2 Korteweg C, Gu J (May 2008). "Pathology, molecular biology, and pathogenesis of avian influenza A (H5N1) infection in humans". Am. J. Pathol. 172 (5): 1155–70. doi:10.2353/ajpath.2008.070791. PMC 2329826. PMID 18403604.
- ↑ Nicholls JM, Chan RW, Russell RJ, Air GM, Peiris JS (April 2008). "Evolving complexities of influenza virus and its receptors". Trends Microbiol. 16 (4): 149–57. doi:10.1016/j.tim.2008.01.008. PMID 18375125.
- ↑ van Riel D, Munster VJ, de Wit E, et al. (April 2006). "H5N1 Virus Attachment to Lower Respiratory Tract". Science 312 (5772): 399. doi:10.1126/science.1125548. PMID 16556800.
- ↑ Shinya K, Ebina M, Yamada S, Ono M, Kasai N, Kawaoka Y (March 2006). "Avian flu: influenza virus receptors in the human airway". Nature 440 (7083): 435–6. Bibcode:2006Natur.440..435S. doi:10.1038/440435a. PMID 16554799.
- ↑ van Riel D, Munster VJ, de Wit E, et al. (October 2007). "Human and avian influenza viruses target different cells in the lower respiratory tract of humans and other mammals". Am. J. Pathol. 171 (4): 1215–23. doi:10.2353/ajpath.2007.070248. PMC 1988871. PMID 17717141.
- ↑ Schmitz N, Kurrer M, Bachmann M, Kopf M (2005). "Interleukin-1 is responsible for acute lung immunopathology but increases survival of respiratory influenza virus infection". J Virol 79 (10): 6441–8. doi:10.1128/JVI.79.10.6441-6448.2005. PMC 1091664. PMID 15858027.
- ↑ Winther B, Gwaltney J, Mygind N, Hendley J (1998). "Viral-induced rhinitis". Am J Rhinol 12 (1): 17–20. doi:10.2500/105065898782102954. PMID 9513654.
- ↑ Cheung CY, Poon LL, Lau AS, et al. (December 2002). "Induction of proinflammatory cytokines in human macrophages by influenza A (H5N1) viruses: a mechanism for the unusual severity of human disease?". Lancet 360 (9348): 1831–7. doi:10.1016/S0140-6736(02)11772-7. PMID 12480361.
- ↑ Kobasa D, Jones SM, Shinya K, et al. (January 2007). "Aberrant innate immune response in lethal infection of macaques with the 1918 influenza virus". Nature 445 (7125): 319–23. Bibcode:2007Natur.445..319K. doi:10.1038/nature05495. PMID 17230189.
- ↑ Kash JC, Tumpey TM, Proll SC, et al. (October 2006). "Genomic analysis of increased host immune and cell death responses induced by 1918 influenza virus". Nature 443 (7111): 578–81. Bibcode:2006Natur.443..578K. doi:10.1038/nature05181. PMC 2615558. PMID 17006449.
- ↑ Beigel J, Bray M (April 2008). "Current and future antiviral therapy of severe seasonal and avian influenza". Antiviral Res. 78 (1): 91–102. doi:10.1016/j.antiviral.2008.01.003. PMC 2346583. PMID 18328578.
- ↑ "Vaccine use". World Health Organization. Retrieved 6 December 2012.
- ↑ Smith NM, Bresee JS, Shay DK, Uyeki TM, Cox NJ, Strikas RA (July 2006). "Prevention and Control of Influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP)" (PDF). MMWR Recomm Rep 55 (RR–10): 1–42. PMID 16874296.
- ↑ Jefferson, T; Di Pietrantonj, C; Rivetti, A; Bawazeer, GA; Al-Ansary, LA; Ferroni, E (13 March 2014). "Vaccines for preventing influenza in healthy adults.". The Cochrane database of systematic reviews 3: CD001269. doi:10.1002/14651858.CD001269.pub5. PMID 24623315.
- ↑ Jefferson T, Rivetti A, Di Pietrantonj C, Demicheli V, Ferroni E (2012). "Vaccines for preventing influenza in healthy children". Cochrane Database Syst Rev 8: CD004879. doi:10.1002/14651858.CD004879.pub4. PMID 22895945.
- ↑ Poole PJ, Chacko E, Wood-Baker RW, Cates CJ (2006). "Influenza vaccine for patients with chronic obstructive pulmonary disease". Cochrane Database Syst Rev (1): CD002733. doi:10.1002/14651858.CD002733.pub2. PMID 16437444.
- ↑ Cates, CJ; Rowe, BH (28 February 2013). "Vaccines for preventing influenza in people with asthma.". The Cochrane database of systematic reviews 2: CD000364. doi:10.1002/14651858.CD000364.pub4. PMID 23450529.
- ↑ Beck, CR; McKenzie, BC; Hashim, AB; Harris, RC; University of Nottingham Influenza and the ImmunoCompromised (UNIIC) Study Group; Nguyen-Van-Tam, JS (October 2012). "Influenza vaccination for immunocompromised patients: systematic review and meta-analysis by etiology.". The Journal of Infectious Diseases 206 (8): 1250–9. doi:10.1093/infdis/jis487. PMID 22904335.
- ↑ Udell, JA.; Zawi, R.; Bhatt, DL.; Keshtkar-Jahromi, M.; Gaughran, F.; Phrommintikul, A.; Ciszewski, A.; Vakili, H.; et al. (Oct 2013). "Association between influenza vaccination and cardiovascular outcomes in high-risk patients: a meta-analysis.". JAMA 310 (16): 1711–20. doi:10.1001/jama.2013.279206. PMID 24150467.
- ↑ Abramson ZH (2012). "What, in Fact, Is the Evidence That Vaccinating Healthcare Workers against Seasonal Influenza Protects Their Patients? A Critical Review". Int J Family Med 2012: 205464. doi:10.1155/2012/205464. PMC 3502850. PMID 23209901.
- ↑ Thomas, RE; Jefferson, T; Lasserson, TJ (22 July 2013). "Influenza vaccination for healthcare workers who care for people aged 60 or older living in long-term care institutions.". The Cochrane database of systematic reviews 7: CD005187. doi:10.1002/14651858.CD005187.pub4. PMID 23881655.
- ↑ Ahmed, F; Lindley, MC; Allred, N; Weinbaum, CM; Grohskopf, L (13 November 2013). "Effect of Influenza Vaccination of Healthcare Personnel on Morbidity and Mortality Among Patients: Systematic Review and Grading of Evidence.". Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 58 (1): 50–7. doi:10.1093/cid/cit580. PMID 24046301.
- ↑ Dolan, GP; Harris, RC; Clarkson, M; Sokal, R; Morgan, G; Mukaigawara, M; Horiuchi, H; Hale, R; Stormont, L; Béchard-Evans, L; Chao, YS; Eremin, S; Martins, S; Tam, J; Peñalver, J; Zanuzadana, A; Nguyen-Van-Tam, JS (September 2013). "Vaccination of healthcare workers to protect patients at increased risk of acute respiratory disease: summary of a systematic review.". Influenza and other respiratory viruses. 7 Suppl 2: 93–6. doi:10.1111/irv.12087. PMID 24034492.
- 1 2 Recommended composition of influenza virus vaccines for use in the 2006–2007 influenza season WHO report 14 February 2006. Retrieved 19 October 2006.
- ↑ Holmes E, Ghedin E, Miller N, Taylor J, Bao Y, St George K, Grenfell B, Salzberg S, Fraser C, Lipman D, Taubenberger J (September 2005). "Whole-genome analysis of human influenza A virus reveals multiple persistent lineages and reassortment among recent H3N2 viruses". PLoS Biol 3 (9): e300. doi:10.1371/journal.pbio.0030300. PMC 1180517. PMID 16026181.
- 1 2 Key Facts about Influenza (Flu) Vaccine CDC publication. Published 17 October 2006. Retrieved 18 October 2006.
- ↑ Questions & Answers: Flu Shot CDC publication updated 24 July 2006. Retrieved 19 October 2006.
- ↑ Jit, Mark; Newall, Anthony T.; Beutels, Philippe (1 April 2013). "Key issues for estimating the impact and cost-effectiveness of seasonal influenza vaccination strategies". Human vaccines & immunotherapeutics 9 (4): 834–840. doi:10.4161/hv.23637. PMC 3903903. PMID 23357859.
- ↑ Newall, Anthony T.; Jit, Mark; Beutels, Philippe (1 August 2012). "Economic Evaluations of Childhood Influenza Vaccination". PharmacoEconomics 30 (8): 647–660. doi:10.2165/11599130-000000000-00000.
- ↑ Postma, Maarten J; Baltussen, Rob PM; Palache, Abraham M; Wilschut, Jan C (1 April 2006). "Further evidence for favorable cost-effectiveness of elderly influenza vaccination". Expert Review of Pharmacoeconomics & Outcomes Research 6 (2): 215–227. doi:10.1586/14737167.6.2.215. PMID 20528557.
- ↑ Newall, Anthony T.; Dehollain, Juan Pablo; Creighton, Prudence; Beutels, Philippe; Wood, James G. (4 May 2013). "Understanding the Cost-Effectiveness of Influenza Vaccination in Children: Methodological Choices and Seasonal Variability". PharmacoEconomics 31 (8): 693–702. doi:10.1007/s40273-013-0060-7.
- ↑ Newall, Anthony T.; Kelly, Heath; Harsley, Stuart; Scuffham, Paul A. (1 June 2009). "Cost Effectiveness of Influenza Vaccination in Older Adults". PharmacoEconomics 27 (6): 439–450. doi:10.2165/00019053-200927060-00001. PMID 19640008.
- ↑ Centers for Disease Control and Prevention: "QUESTIONS & ANSWERS: Novel H1N1 Flu (Swine Flu) and You". Retrieved 15 December 2009.
- ↑ Grayson ML, Melvani S, Druce J, et al. (February 2009). "Efficacy of soap and water and alcohol-based hand-rub preparations against live H1N1 influenza virus on the hands of human volunteers". Clin. Infect. Dis. 48 (3): 285–91. doi:10.1086/595845. PMID 19115974.
- 1 2 3 4 Aledort JE, Lurie N, Wasserman J, Bozzette SA (2007). "Non-pharmaceutical public health interventions for pandemic influenza: an evaluation of the evidence base". BMC Public Health 7: 208. doi:10.1186/1471-2458-7-208. PMC 2040158. PMID 17697389.
- ↑ MacIntyre CR, Cauchemez S, Dwyer DE, et al. (February 2009). "Face mask use and control of respiratory virus transmission in households" (PDF). Emerging Infect. Dis. 15 (2): 233–41. doi:10.3201/eid1502.081167. PMC 2662657. PMID 19193267.
- ↑ Bridges CB, Kuehnert MJ, Hall CB (October 2003). "Transmission of influenza: implications for control in health care settings". Clin. Infect. Dis. 37 (8): 1094–101. doi:10.1086/378292. PMID 14523774.
- ↑ Interim Guidance for the Use of Masks to Control Influenza Transmission Coordinating Center for Infectious Diseases (CCID) 8 August 2005
- ↑ Murin, Susan; Kathryn Smith Bilello (2005). "Respiratory tract infections: another reason not to smoke" (PDF). Cleveland Clinic Journal of Medicine 72 (10): 916–920. doi:10.3949/ccjm.72.10.916. PMID 16231688. Retrieved 1 October 2009.
- ↑ Kark, J D; M Lebiush; L Rannon (1982). "Cigarette smoking as a risk factor for epidemic a(h1n1) influenza in young men". The New England Journal of Medicine 307 (17): 1042–1046. doi:10.1056/NEJM198210213071702. ISSN 0028-4793. PMID 7121513.
- ↑ Hota B; Hota, B. (2004). "Contamination, disinfection, and cross-colonization: are hospital surfaces reservoirs for nosocomial infection?". Clin Infect Dis 39 (8): 1182–9. doi:10.1086/424667. PMID 15486843.
- 1 2 McDonnell G, Russell A (1 January 1999). "Antiseptics and disinfectants: activity, action, and resistance" (PDF). Clin Microbiol Rev 12 (1): 147–79. PMC 88911. PMID 9880479.
- ↑ "Chlorine Bleach: Helping to Manage the Flu Risk". Water Quality & Health Council. April 2009. Retrieved 12 May 2009.
- ↑ Hatchett RJ, Mecher CE, Lipsitch M (2007). "Public health interventions and epidemic intensity during the 1918 influenza pandemic" (PDF). Proc Natl Acad Sci U S A. 104 (18): 7582–7587. Bibcode:2007PNAS..104.7582H. doi:10.1073/pnas.0610941104. PMC 1849867. PMID 17416679.
- ↑ Bootsma MC, Ferguson NM (2007). "The effect of public health measures on the 1918 influenza pandemic in U.S. cities" (PDF). Proc Natl Acad Sci U S A. 104 (18): 7588–7593. Bibcode:2007PNAS..104.7588B. doi:10.1073/pnas.0611071104. PMC 1849868. PMID 17416677.
- ↑ "Flu: MedlinePlus Medical Encyclopedia". U.S. National Library of Medicine. Retrieved 7 February 2010.
- ↑ Glasgow, J; Middleton B (2001). "Reye syndrome — insights on causation and prognosis" (PDF). Arch Dis Child 85 (5): 351–3. doi:10.1136/adc.85.5.351. PMC 1718987. PMID 11668090.
- ↑ Hurt AC, Ho HT, Barr I (October 2006). "Resistance to anti-influenza drugs: adamantanes and neuraminidase inhibitors". Expert Rev Anti Infect Ther 4 (5): 795–805. doi:10.1586/14787210.4.5.795. PMID 17140356.
- ↑ Jefferson T, Jones MA, Doshi P, et al. (2012). "Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children". Cochrane Database Syst Rev 1: CD008965. doi:10.1002/14651858.CD008965.pub3. PMID 22258996.
- ↑ Stephenson, I; Nicholson K (1999). "Chemotherapeutic control of influenza" (PDF). J Antimicrob Chemother 44 (1): 6–10. doi:10.1093/jac/44.1.6. PMID 10459804.
- ↑ Centers for Disease Control and Prevention (CDC) (2006). "High levels of adamantane resistance among influenza A (H3N2) viruses and interim guidelines for use of antiviral agents — United States, 2005–06 influenza season" (PDF). MMWR Morb Mortal Wkly Rep 55 (2): 44–6. PMID 16424859.
- ↑ Bright, Rick A; Medina, Marie-jo; Xu, Xiyan; Perez-Oronoz, Gilda; Wallis, Teresa R; Davis, Xiaohong M; Povinelli, Laura; Cox, Nancy J; Klimov, Alexander I (2005). "Incidence of adamantane resistance among influenza A (H3N2) viruses isolated worldwide from 1994 to 2005: a cause for concern". The Lancet 366 (9492): 1175–81. doi:10.1016/S0140-6736(05)67338-2. PMID 16198766.
- ↑ Ilyushina NA, Govorkova EA, Webster RG (October 2005). "Detection of amantadine-resistant variants among avian influenza viruses isolated in North America and Asia" (PDF). Virology 341 (1): 102–6. doi:10.1016/j.virol.2005.07.003. PMID 16081121.
- ↑ Parry J (July 2005). "Use of antiviral drug in poultry is blamed for drug resistant strains of avian flu". BMJ 331 (7507): 10. doi:10.1136/bmj.331.7507.10. PMC 558527. PMID 15994677.
- ↑ Centers for Disease Control and Prevention. CDC Recommends against the Use of Amantadine and Rimantadine for the Treatment or Prophylaxis of Influenza in the United States during the 2005–06 Influenza Season. 14 January 2006. Retrieved 1 January 2007
- ↑ Hayden FG (March 1997). "Prevention and treatment of influenza in immunocompromised patients". Am. J. Med. 102 (3A): 55–60; discussion 75–6. doi:10.1016/S0002-9343(97)80013-7. PMID 10868144.
- ↑ Whitley RJ, Monto AS (2006). "Prevention and treatment of influenza in high-risk groups: children, pregnant women, immunocompromised hosts, and nursing home residents" (PDF). J Infect Dis. 194 S2: S133–8. doi:10.1086/507548. PMID 17163386.
- ↑ Angelo SJ, Marshall PS, Chrissoheris MP, Chaves AM (April 2004). "Clinical characteristics associated with poor outcome in patients acutely infected with Influenza A". Conn Med 68 (4): 199–205. PMID 15095826.
- ↑ Murin S, Bilello K (2005). "Respiratory tract infections: another reason not to smoke". Cleve Clin J Med 72 (10): 916–20. doi:10.3949/ccjm.72.10.916. PMID 16231688.
- ↑ Sandman, Peter M; Lanard, Jody (2005). "Bird Flu: Communicating the Risk" (PDF). Perspectives in Health Magazine 10 (2): 1–6.
- 1 2 Sivadon-Tardy V, Orlikowski D, Porcher R, et al. (January 2009). "Guillain-Barré syndrome and influenza virus infection". Clin. Infect. Dis. 48 (1): 48–56. doi:10.1086/594124. PMID 19025491.
- ↑ Jacobs BC, Rothbarth PH, van der Meché FG, et al. (October 1998). "The spectrum of antecedent infections in Guillain-Barré syndrome: a case-control study". Neurology 51 (4): 1110–5. doi:10.1212/wnl.51.4.1110. PMID 9781538.
- ↑ Vellozzi C, Burwen DR, Dobardzic A, Ball R, Walton K, Haber P (March 2009). "Safety of trivalent inactivated influenza vaccines in adults: Background for pandemic influenza vaccine safety monitoring". Vaccine 27 (15): 2114–2120. doi:10.1016/j.vaccine.2009.01.125. PMID 19356614.
- ↑ Stowe J, Andrews N, Wise L, Miller E (February 2009). "Investigation of the temporal association of Guillain-Barre syndrome with influenza vaccine and influenzalike illness using the United Kingdom General Practice Research Database" (PDF). Am. J. Epidemiol. 169 (3): 382–8. doi:10.1093/aje/kwn310. PMID 19033158.
- ↑ Sivadon-Tardy V, Orlikowski D, Porcher R, et al. (January 2009). "Guillain-Barré syndrome and influenza virus infection" (PDF). Clin. Infect. Dis. 48 (1): 48–56. doi:10.1086/594124. PMID 19025491.
- ↑ Weather and the Flu Season NPR Day to Day, 17 December 2003. Retrieved, 19 October 2006
- ↑ Lowen, AC; Mubareka, S; Steel, J; Palese, P (October 2007). "Influenza virus transmission is dependent on relative humidity and temperature". PLoS Pathogens 3 (10): e151. doi:10.1371/journal.ppat.0030151. PMC 2034399. PMID 17953482.
- ↑ Shaman J, Kohn M (March 2009). "Absolute humidity modulates influenza survival, transmission, and seasonality". Proc. Natl. Acad. Sci. U.S.A. 106 (9): 3243–8. Bibcode:2009PNAS..106.3243S. doi:10.1073/pnas.0806852106. PMC 2651255. PMID 19204283.
- ↑ Shaman J, Pitzer VE, Viboud C, Grenfell BT, Lipsitch M (February 2010). Ferguson, Neil M, ed. "Absolute humidity and the seasonal onset of influenza in the continental United States". PLoS Biol. 8 (2): e1000316. doi:10.1371/journal.pbio.1000316. PMC 2826374. PMID 20186267.
- ↑ Shek, LP; Lee, BW (2003). "Epidemiology and seasonality of respiratory tract virus infections in the tropics". Paediatric respiratory reviews 4 (2): 105–11. doi:10.1016/S1526-0542(03)00024-1. PMID 12758047.
- ↑ Dushoff, J; Plotkin, JB; Levin, SA; Earn, DJ (2004). "Dynamical resonance can account for seasonality of influenza epidemics". Proceedings of the National Academy of Sciences of the United States of America 101 (48): 16915–6. Bibcode:2004PNAS..10116915D. doi:10.1073/pnas.0407293101. PMC 534740. PMID 15557003.
- ↑ WHO Confirmed Human Cases of H5N1 Data published by WHO Epidemic and Pandemic Alert and Response (EPR). Retrieved 24 October 2006
- ↑ Cannell, J; Vieth R; Umhau J; Holick M; Grant W; Madronich S; Garland C; Giovannucci E (2006). "Epidemic influenza and vitamin D". Epidemiol Infect 134 (6): 1129–40. doi:10.1017/S0950268806007175. PMC 2870528. PMID 16959053.
- ↑ HOPE-SIMPSON, R (1965). "The nature of herpes zoster: a long-term study and a new hypothesis". Proceedings of the Royal Society of Medicine 58: 9–20. PMC 1898279. PMID 14267505.
- ↑ Lozano, R (15 December 2012). "Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010.". Lancet 380 (9859): 2095–128. doi:10.1016/S0140-6736(12)61728-0. PMID 23245604.
- ↑ Influenza WHO Fact sheet No. 211 revised March 2003. Retrieved 22 October 2006.
- ↑ Thompson, W; Shay D; Weintraub E; Brammer L; Cox N; Anderson L; Fukuda K (2003). "Mortality associated with influenza and respiratory syncytial virus in the United States" (PDF). JAMA 289 (2): 179–86. doi:10.1001/jama.289.2.179. PMID 12517228.
- ↑ Thompson, W; Shay D; Weintraub E; Brammer L; Bridges C; Cox N; Fukuda K (2004). "Influenza-associated hospitalizations in the United States" (PDF). JAMA 292 (11): 1333–40. doi:10.1001/jama.292.11.1333. PMID 15367555.
- ↑ Jonathan Dushoff; Plotkin, JB; Viboud, C; Earn, DJ; Simonsen, L (2006). "Mortality due to Influenza in the United States — An Annualized Regression Approach Using Multiple-Cause Mortality Data". American Journal of Epidemiology 163 (2): 181–7. doi:10.1093/aje/kwj024. PMID 16319291. Retrieved 29 October 2009.
The regression model attributes an annual average of 41,400 (95% confidence interval: 27,100, 55,700) deaths to influenza over the period 1979–2001
- ↑ Julie Steenhuysen (26 August 2010). "CDC backs away from decades-old flu death estimate". Reuters. Retrieved 13 September 2010.
Instead of the estimated 36,000 annual flu deaths in the United States ... the actual number in the past 30 years has ranged from a low of about 3,300 deaths to a high of nearly 49,000, the CDC said on Thursday
- ↑ Murray CJ, Lopez AD, Chin B, Feehan D, Hill KH (December 2006). "Estimation of potential global pandemic influenza mortality on the basis of vital registry data from the 1918–20 pandemic: a quantitative analysis". Lancet 368 (9554): 2211–8. doi:10.1016/S0140-6736(06)69895-4. PMID 17189032.
- ↑ Wolf, Yuri I; Viboud, C; Holmes, EC; Koonin, EV; Lipman, DJ (2006). "Long intervals of stasis punctuated by bursts of positive selection in the seasonal evolution of influenza A virus". Biol Direct 1 (1): 34. doi:10.1186/1745-6150-1-34. PMC 1647279. PMID 17067369.
- ↑ Parrish, C; Kawaoka Y (2005). "The origins of new pandemic viruses: the acquisition of new host ranges by canine parvovirus and influenza A viruses". Annual Rev Microbiol 59: 553–86. doi:10.1146/annurev.micro.59.030804.121059. PMID 16153179.
- ↑ Recker M, Pybus OG, Nee S, Gupta S (2007). "The generation of influenza outbreaks by a network of host immune responses against a limited set of antigenic types" (PDF). Proc Natl Acad Sci U S A. 104 (18): 7711–16. Bibcode:2007PNAS..104.7711R. doi:10.1073/pnas.0702154104. PMC 1855915. PMID 17460037.
- 1 2 Ferguson, NM; Cummings DA; Cauchemez S; Fraser C; Riley S; Meeyai A; Iamsirithaworn S; Burke DS (2005). "Strategies for containing an emerging influenza pandemic in Southeast Asia". Nature 437 (7056): 209–14. Bibcode:2005Natur.437..209F. doi:10.1038/nature04017. PMID 16079797.
- ↑ Influenza, The Oxford English Dictionary, second edition.
- ↑ Creighton, Charles (1965): A History Of Epidemics In Britain, With Additional Material By D.E.C. Eversley
- ↑ Potter, CW (2001). "A history of influenza". Journal of applied microbiology 91 (4): 572–579. doi:10.1046/j.1365-2672.2001.01492.x. PMID 11576290.
- ↑ Smith, P (2009). "Swine Flu". Croatian Medical Journal 50 (4): 412–5. doi:10.3325/cmj.2009.50.412. PMC 2728380. PMID 19673043.
- 1 2 3 4 Taubenberger, J; Morens D (2006). "1918 Influenza: the mother of all pandemics". Emerg Infect Dis 12 (1): 15–22. doi:10.3201/eid1201.050979. PMC 3291398. PMID 16494711.
- ↑ Martin, P; Martin-Granel E (June 2006). "2,500-year evolution of the term epidemic". Emerg Infect Dis 12 (6): 976–80. doi:10.3201/eid1206.051263. PMC 3373038. PMID 16707055.
- ↑ Hippocrates. "Of the Epidemics, c. 400 BCE". Adams, Francis (transl.). Retrieved 18 October 2006.
- ↑ Beveridge, W I (1991). "The chronicle of influenza epidemics". History and Philosophy of the Life Sciences 13 (2): 223–234. PMID 1724803.
- 1 2 3 4 Potter CW (October 2001). "A History of Influenza". Journal of Applied Microbiology 91 (4): 572–579. doi:10.1046/j.1365-2672.2001.01492.x. PMID 11576290.
- ↑ Guerra, Francisco (1988). "The Earliest American Epidemic: The Influenza of 1493". Social Science History 12 (3): 305–325. doi:10.2307/1171451. JSTOR 1171451. PMID 11618144. (only the first page can be read for free, but that has enough information about influenza being the main disease brought by Columbus killing 90 % of the indigenous population)
- ↑ Guerra, F (1993). "The European-American exchange". History and Philosophy of the Life Sciences 15 (3): 313–327. PMID 7529930.
- 1 2 3 4 5 Knobler S, Mack A, Mahmoud A, Lemon S (ed.). "1: The Story of Influenza". The Threat of Pandemic Influenza: Are We Ready? Workshop Summary (2005). Washington, D.C.: The National Academies Press. pp. 60–61.
- 1 2 Patterson, KD; Pyle GF (Spring 1991). "The geography and mortality of the 1918 influenza pandemic". Bull Hist Med. 65 (1): 4–21. PMID 2021692.
- ↑ Taubenberger JK, Reid AH, Janczewski TA, Fanning TG (December 2001). "Integrating historical, clinical and molecular genetic data in order to explain the origin and virulence of the 1918 Spanish influenza virus". Philosophical Transactions of the Royal Society B 356 (1416): 1829–39. doi:10.1098/rstb.2001.1020. PMC 1088558. PMID 11779381.
- ↑ Simonsen, L; Clarke M; Schonberger L; Arden N; Cox N; Fukuda K (July 1998). "Pandemic versus epidemic influenza mortality: a pattern of changing age distribution". J Infect Dis 178 (1): 53–60. doi:10.1086/515616. PMID 9652423.
- ↑ Valleron AJ, Cori A, Valtat S, Meurisse S, Carrat F, Boëlle PY (May 2010). "Transmissibility and geographic spread of the 1889 influenza pandemic". Proc. Natl. Acad. Sci. U.S.A. 107 (19): 8778–81. Bibcode:2010PNAS..107.8778V. doi:10.1073/pnas.1000886107. PMC 2889325. PMID 20421481.
- ↑ Mills CE, Robins JM, Lipsitch M (December 2004). "Transmissibility of 1918 pandemic influenza". Nature 432 (7019): 904–6. Bibcode:2004Natur.432..904M. doi:10.1038/nature03063. PMID 15602562.
- ↑ Donaldson LJ, Rutter PD, Ellis BM, et al. (2009). "Mortality from pandemic A/H1N1 2009 influenza in England: public health surveillance study". BMJ 339: b5213. doi:10.1136/bmj.b5213. PMC 2791802. PMID 20007665.
- ↑ Fatimah S Dawood, A Danielle Iuliano, Carrie Reed, Martin I Meltzer, David K Shay, Po-Yung Cheng, Don Bandaranayake, Robert F Breiman, W Abdullah Brooks, Philippe Buchy, Daniel R Feikin, Karen B Fowler, Aubree Gordon, Nguyen Tran Hien, Peter Horby, Q Sue Huang, Mark A Katz, Anand Krishnan, Renu Lal, Joel M Montgomery, Kåre Mølbak, Richard Pebody, Anne M Presanis, Hugo Razuri, Anneke Steens, Yeny O Tinoco, Jacco Wallinga, Hongjie, Sirenda Vong, Joseph Bresee, Marc-Alain Widdowson (26 June 2012). "Estimated global mortality associated with the first 12 months of 2009 pandemic influenza A H1N1 virus circulation: a modelling study". The Lancet Infectious Diseases 12 (9): 687–95. doi:10.1016/S1473-3099(12)70121-4. PMID 22738893. Retrieved 19 March 2014.
- ↑ Heinen PP (15 September 2003). "Swine influenza: a zoonosis". Veterinary Sciences Tomorrow. ISSN 1569-0830.
- ↑ Shimizu, K (October 1997). "History of influenza epidemics and discovery of influenza virus". Nippon Rinsho 55 (10): 2505–201. PMID 9360364.
- ↑ Smith, W; Andrewes CH; Laidlaw PP (1933). "A virus obtained from influenza patients". Lancet 2 (5732): 66–68. doi:10.1016/S0140-6736(00)78541-2.
- ↑ Palese P (December 2004). "Influenza: old and new threats". Nat. Med. 10 (12 Suppl): S82–7. doi:10.1038/nm1141. PMID 15577936.
- ↑ Sir Frank Macfarlane Burnet: Biography The Nobel Foundation. Retrieved 22 October 2006
- ↑ Kendall, H (2006). "Vaccine Innovation: Lessons from World War II". Journal of Public Health Policy 27 (1): 38–57. doi:10.1057/palgrave.jphp.3200064. PMID 16681187.
- ↑ Statement from President George W. Bush on Influenza Retrieved 26 October 2006
- ↑ Brainerd, E. and M. Siegler (2003), "The Economic Effects of the 1918 Influenza Epidemic", CEPR Discussion Paper, no. 3791.
- ↑ Poland G (2006). "Vaccines against avian influenza—a race against time" (PDF). N Engl J Med 354 (13): 1411–3. doi:10.1056/NEJMe068047. PMID 16571885.
- 1 2 Rosenthal, E; Bradsher, K (16 March 2006). "Is Business Ready for a Flu Pandemic?". The New York Times. Retrieved 17 April 2006.
- ↑ National Strategy for Pandemic Influenza Whitehouse.gov Retrieved 26 October 2006.
- ↑ Bush Outlines $7 Billion Pandemic Flu Preparedness Plan US Mission to the EU. Retrieved 12 December 2009.
- ↑ Donor Nations Pledge $1.85 Billion to Combat Bird Flu Newswire Retrieved 26 October 2006.
- ↑ Assessment of the 2009 Influenza A (H1N1) Outbreak on Selected Countries in the Southern Hemisphere. 2009. http://flu.gov/professional/global/southhemisphere.html
- ↑ Influenza A Virus Genome Project at The Institute of Genomic Research. Retrieved 19 October 2006
- ↑ Subbarao K, Katz J (2004). "Influenza vaccines generated by reverse genetics". Curr Top Microbiol Immunol 283: 313–42. doi:10.1007/978-3-662-06099-5_9. PMID 15298174.
- ↑ Bardiya N, Bae J (2005). "Influenza vaccines: recent advances in production technologies". Appl Microbiol Biotechnol 67 (3): 299–305. doi:10.1007/s00253-004-1874-1. PMID 15660212.
- ↑ Neirynck S, Deroo T, Saelens X, Vanlandschoot P, Jou WM, Fiers W (October 1999). "A universal influenza A vaccine based on the extracellular domain of the M2 protein". Nat. Med. 5 (10): 1157–63. doi:10.1038/13484. PMID 10502819.
- ↑ Fiers W, Neirynck S, Deroo T, Saelens X, Jou WM (December 2001). "Soluble recombinant influenza vaccines". Philosophical Transactions of the Royal Society B 356 (1416): 1961–3. doi:10.1098/rstb.2001.0980. PMC 1088575. PMID 11779398.
- ↑ Fiers W, De Filette M, Birkett A, Neirynck S, Min Jou W (July 2004). "A "universal" human influenza A vaccine". Virus Res. 103 (1–2): 173–6. doi:10.1016/j.virusres.2004.02.030. PMID 15163506.
- ↑ Petsch B, Schnee M, Vogel AB, et al. (November 2012). "Protective efficacy of in vitro synthesized, specific mRNA vaccines against influenza A virus infection". Nat. Biotechnol. 30 (12): 1210–6. doi:10.1038/nbt.2436. PMID 23159882.
- ↑ Stephen Adams (8 July 2011). "Universal flu vaccine a step closer". The Telegraph.
- ↑ Ekiert, DC; Friesen, RHE; Bhabha, G; Kwaks, T; Jongeneelen, M; Yu, W; Ophorst, C; Cox, F; et al. (2011). "A Highly Conserved Neutralizing Epitope on Group 2 Influenza a Viruses". Science 333 (6044): 843–50. Bibcode:2011Sci...333..843E. doi:10.1126/science.1204839. PMC 3210727. PMID 21737702.
- ↑ Gingerich, DA (2008). "Lymphocyte T-Cell Immunomodulator: Review of the ImmunoPharmacology of a new Veterinary Biologic" (PDF). Journal of Applied Research in Veterinary Medicine 6 (2): 61–68. Retrieved 5 December 2010.
- ↑ Gorman O, Bean W, Kawaoka Y, Webster R (1990). "Evolution of the nucleoprotein gene of influenza A virus". J Virol 64 (4): 1487–97. PMC 249282. PMID 2319644.
- ↑ Hinshaw V, Bean W, Webster R, Rehg J, Fiorelli P, Early G, Geraci J, St Aubin D (1984). "Are seals frequently infected with avian influenza viruses?". J Virol 51 (3): 863–5. PMC 255856. PMID 6471169.
- ↑ Capua, I; Alexander D (2006). "The challenge of avian influenza to the veterinary community" (PDF). Avian Pathol 35 (3): 189–205. doi:10.1080/03079450600717174. PMID 16753610.
- ↑ Elbers A, Koch G, Bouma A (2005). "Performance of clinical signs in poultry for the detection of outbreaks during the avian influenza A (H7N7) epidemic in The Netherlands in 2003". Avian Pathol 34 (3): 181–7. doi:10.1080/03079450500096497. PMID 16191700.
- ↑ Capua, I; Mutinelli, F (2001). "Low pathogenicity (LPAI) and highly pathogenic (HPAI) avian influenza in turkeys and chicken". A Colour Atlas and Text on Avian Influenza. Bologna: Papi Editore. pp. 13–20. ISBN 88-88369-00-7.
- ↑ Bano S, Naeem K, Malik S (2003). "Evaluation of pathogenic potential of avian influenza virus serotype H9N2 in chickens". Avian Dis 47 (3 Suppl): 817–22. doi:10.1637/0005-2086-47.s3.817. PMID 14575070.
- ↑ Swayne D, Suarez D (2000). "Highly pathogenic avian influenza". Rev Sci Tech 19 (2): 463–82. PMID 10935274.
- ↑ Li K, Guan Y, Wang J, Smith G, Xu K, Duan L, Rahardjo A, Puthavathana P, Buranathai C, Nguyen T, Estoepangestie A, Chaisingh A, Auewarakul P, Long H, Hanh N, Webby R, Poon L, Chen H, Shortridge K, Yuen K, Webster R, Peiris J (2004). "Genesis of a highly pathogenic and potentially pandemic H5N1 influenza virus in eastern Asia". Nature 430 (6996): 209–13. Bibcode:2004Natur.430..209L. doi:10.1038/nature02746. PMID 15241415.
- ↑ Li KS, Guan Y, Wang J, Smith GJ, Xu KM, Duan L, Rahardjo AP, Puthavathana P, Buranathai C, Nguyen TD, Estoepangestie AT, Chaisingh A, Auewarakul P, Long HT, Hanh NT, Webby RJ, Poon LL, Chen H, Shortridge KF, Yuen KY, Webster RG, Peiris JS. "The Threat of Pandemic Influenza: Are We Ready?" Workshop Summary The National Academies Press (2005) "Today's Pandemic Threat: Genesis of a Highly Pathogenic and Potentially Pandemic H5N1 Influenza Virus in Eastern Asia", pages 116–130
- ↑ Liu J (2006). "Avian influenza—a pandemic waiting to happen?" (PDF). J Microbiol Immunol Infect 39 (1): 4–10. PMID 16440117.
- ↑ Salomon R, Webster RG (February 2009). "The influenza virus enigma". Cell 136 (3): 402–10. doi:10.1016/j.cell.2009.01.029. PMC 2971533. PMID 19203576.
- ↑ 2 Men in China Die of Lesser-Known Strain of Bird Flu, New York Times, DAVID BARBOZA, 31 March 2013.
- ↑ H7N9 avian influenza human infections in China, World Health Organization, 1 April 2013. "... So far no further cases have been identified among the 88 identified contacts under follow up."
- ↑ Deadly Bird Flu Spreading in China, Unclear How, ABC News, Katie Moisse, 18 April 2013.
- ↑ Background and summary of human infection with influenza A(H7N9) virus– as of 5 April 2013, World Health Organization.
- 1 2 3 Kothalawala H, Toussaint MJ, Gruys E (June 2006). "An overview of swine influenza". Vet Q 28 (2): 46–53. doi:10.1080/01652176.2006.9695207. PMID 16841566.
- ↑ Myers KP, Olsen CW, Gray GC (April 2007). "Cases of swine influenza in humans: a review of the literature". Clin. Infect. Dis. 44 (8): 1084–8. doi:10.1086/512813. PMC 1973337. PMID 17366454.
- ↑ Maria Zampaglione (29 April 2009). "Press Release: A/H1N1 influenza like human illness in Mexico and the USA: OIE statement". World Organisation for Animal Health. Archived from the original on 30 April 2009. Retrieved 29 April 2009.
- ↑ Grady, Denise (1 May 2009). "W.H.O. Gives Swine Flu a Less Loaded, More Scientific Name". The New York Times. Retrieved 31 March 2010.
- ↑ McNeil Jr, Donald G (1 May 2009). "Virus's Tangled Genes Straddle Continents, Raising a Mystery About Its Origins". The New York Times. Retrieved 31 March 2010.
Further reading
|
General
History
Microbiology
|
Pathogenesis
Epidemiology
Treatment and prevention
Research
|
External links
- ERS Online Course on Influenza
- Info on influenza at CDC
- Fact Sheet Overview of influenza at World Health Organization
- The Multinational Influenza Seasonal Mortality Study (MISMS) Fogarty International Center
- Influenza Virus Resource from the NCBI
- European Influenza Surveillance Scheme
- Online video discussing influenza outbreaks and spread of other infectious diseases (Vega Science Trust)
- PATH Vaccine Resource Library influenza resources
- Influenza Research Database – Database of influenza genomic sequences, serotypes, polymorphisms, structures, epitopes, drugs and related tools
- Recombinomics – What's New: Up to date details of circulating strains.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|