Fibrolamellar hepatocellular carcinoma
| Fibrolamellar hepatocellular carcinoma | |
|---|---|
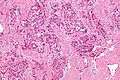
 Micrograph of fibrolamellar hepatocarcinoma showing the characteristic laminated fibrosis between the tumor cells with a low NC ratio. H&E stain. | |
| Classification and external resources | |
| Specialty | oncology |
| ICD-10 | C22.0 |
| ICD-9-CM | 155 |
| ICD-O | M8171/3 |
| DiseasesDB | 34518 |
| eMedicine | med/787 |
Fibrolamellar hepatocellular carcinoma (FHCC) is a rare form of hepatocellular carcinoma (HCC) that typically affects young adults and is characterized, under the microscope, by laminated fibrous layers interspersed between the tumour cells. Approximately 200 new cases are diagnosed worldwide each year.[1]
Diagnosis
Due to lack of symptoms, until the tumor is sizable, this form of cancer is often advanced when diagnosed. Local symptoms may include a palpable liver mass.[2]
FHCC often does not produce alpha fetoprotein (AFP), a widely used marker for conventional hepatocellular carcinoma. However, FHCC is associated with elevated neurotensin levels.
Epidemiology
FHCC has a low age of onset (~27 years[3]) when compared to conventional HCC. Also, unlike conventional HCC, patients most often do not have coexistent liver disease.
FHCC generally occurs in young adults without underlying cirrhosis. Compared to conventional HCC, FHCC grows slowly and has better prognosis, probably owing to its high resectability.
Pathology
The histopathology of FHCC is characterized by laminated fibrous layers, interspersed between the tumor cells. Cytologically, the tumor cells have a low nuclear to cytoplasmic ratio with abundant eosinophilic cytoplasm. Tumors are non-encapsulated, but well circumscribed, when compared to conventional HCC (which typically has an invasive border). A recent study showed the presence of the DNAJB1-PRKACA chimeric transcript (resulting from a 400kb somatic deletion on chromosome 19) in 100% of the FHCCs examined (15/15)[4]
Treatment
In FHCC, plasma neurotensin and serum vitamin B12 binding globulin are commonly increased and are useful in monitoring the disease and detecting recurrence.
FHCC has a high resectability rate, i.e. it can often be surgically removed. Liver resection is the optimal treatment and may need to be performed more than once, since this disease has a very high recurrence rate. Due to such recurrence, periodic follow-up medical imaging (CT or MRI) is necessary.
As the tumor is quite rare, there is no standard chemotherapy regimen.
The survival rate for fibrolamellar HCC largely depends on whether (and to what degree) the cancer has metastasized, i.e. spread to the lymph nodes or other organs. Distant spread (metastases), significantly reduces the median survival rate.
Additional images
-
Intermed. mag.
-

High mag.
See also
References
- ↑ http://www.nbcnews.com/health/cancer/teen-makes-genetic-discovery-her-own-rare-cancer-n75991
- ↑ Yen, JB.; Chang, KW. (2009). "Fibrolamellar hepatocellular carcinoma- report of a case.". Chang Gung Med J 32 (3): 336–9. PMID 19527614.
- ↑ Stipa F, Yoon SS, Liau KH, et al. (March 2006). "Outcome of patients with fibrolamellar hepatocellular carcinoma". Cancer 106 (6): 1331–8. doi:10.1002/cncr.21703. PMID 16475212.
- ↑ Honeyman, Joshua; Elana P. Simon, Nicolas Robine, Rachel Chiaroni-Clarke, David G. Darcy, Irene Isabel P. Lim, Caroline E. Gleason, Jennifer M. Murphy, Brad R. Rosenberg, Lydia Teegan, Constantin N. Takacs, Sergio Botero, Rachel Belote, Soren Germer, Anne-Katrin Emde, Vladimir Vacic, Umesh Bhanot, Michael P. LaQuaglia, and Sanford M. Simon (28 February 2014). "Detection of a Recurrent DNAJB1-PRKACA Chimeric Transcript in Fibrolamellar Hepatocellular Carcinoma". Science 343 (6174): 1010–4. doi:10.1126/science.1249484. PMC 4286414. PMID 24578576. Retrieved 16 April 2014. Cite uses deprecated parameter
|coauthors=(help)
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||