Familial Mediterranean fever
| Familial Mediterranean Fever | |
|---|---|
| Classification and external resources | |
| Specialty | endocrinology |
| ICD-10 | E85.0 |
| ICD-9-CM | 277.31 |
| OMIM | 249100 608107 |
| DiseasesDB | 9836 |
| MedlinePlus | 000363 |
| eMedicine | med/1410 |
| Patient UK | Familial Mediterranean fever |
| MeSH | D010505 |
| GeneReviews | |
Familial Mediterranean fever (FMF), also known as Armenian disease,[1][2] is a hereditary inflammatory disorder.[3]:149 FMF is an autoinflammatory disease caused by mutations in MEFV, a gene which encodes a 781–amino acid protein denoted pyrin.[4]
The disorder has been given various names including familial paroxysmal polyserositis, periodic peritonitis, recurrent polyserositis, benign paroxysmal peritonitis, periodic disease or periodic fever, Reimann periodic disease or Reimann's syndrome, Siegal-Cattan-Mamou disease, and Wolff periodic disease.[5][6][7] Note that "periodic fever" can also refer to any of the Periodic fever syndromes.
Signs and symptoms
Attacks
There are seven types of attacks. Ninety percent of all patients have their first attacks before they are 18 years old. All develop over 2–4 hours and last anywhere from 6 hours to 4 days. Most attacks involve fever.[8]
- Abdominal attacks, featuring abdominal pain, affect the whole abdomen with all signs of peritonitis (inflammation of abdominal lining), and acute abdominal pain like appendicitis. They occur in 95% of all patients and may lead to unnecessary laparotomy. Incomplete attacks, with local tenderness and normal blood tests, have been reported.
- Joint attacks mainly occur in large joints, especially in the legs. Usually, only one joint is affected. Seventy-five percent of all FMF patients experience joint attacks.
- Chest attacks include pleuritis (inflammation of the pleura) and pericarditis (inflammation of the pericardium). Pleuritis occurs in 40% of patients, and makes it difficult to breathe or lie flat, but pericarditis is rare.
- Scrotal attacks due to inflammation of the tunica vaginalis occurs in up to 5% and may be mistaken for acute scrotum (i.e. testicular torsion).
- Myalgia (rare in isolation)
- Erysipeloid (a skin reaction on the legs, rare in isolation)
- Fever without any of the other symptoms listed above (25%)
Complications
AA-amyloidosis with kidney failure is a complication and may develop without overt crises. AA amyloid protein is produced in very large quantities during attacks, and at a low rate between them, and accumulates mainly in the kidney, as well as the heart, spleen, gastrointestinal tract and thyroid.[8]
There appears to be an increase in the risk for developing particular vasculitis-related diseases (e.g. Henoch-Schönlein purpura), spondylarthropathy, prolonged arthritis of certain joints and protracted myalgia.[8]
Pathophysiology
Virtually all cases are due to a mutation in the MEFV gene on the sixteenth chromosome, which codes for a protein called pyrin or marenostrin. Various mutations of this gene lead to FMF, although some mutations cause a more severe picture than others. Mutations occur mainly in exons 2, 3, 5 and 10.[8]
The function of pyrin has not been completely elucidated, but it appears to be a suppressor of the activation of caspase 1, the enzyme that stimulates production of interleukin 1β, a cytokine central to the process of inflammation. In other words an ineffective pyrin doesn't inhibit inflammation normally, resulting in inflammatory episodes of membranes at differing sites. It is not conclusively known what exactly sets off the attacks, and why overproduction of IL-1 would lead to particular symptoms in particular organs (e.g. joints or the peritoneal cavity).[8]
Diagnosis
The diagnosis is clinically made on the basis of the history of typical attacks, especially in patients from the ethnic groups in which FMF is more highly prevalent. An acute phase response is present during attacks, with high C-reactive protein levels, an elevated white blood cell count and other markers of inflammation. In patients with a long history of attacks, monitoring the kidney function is of importance in predicting chronic kidney failure.[8]
A genetic test is also available to detect mutations in the MEFV gene. Sequencing of exons 2, 3, 5, and 10 of this gene detects an estimated 97% of all known mutations.[8]
A specific and highly sensitive test for FMF is the "Metaraminol Provocative Test (MPT)," whereby a single 10 mg infusion of Metaraminol is administered to the patient. A positive diagnosis is made if the patient presents with a typical, albeit milder, FMF attack within 48 hours. As MPT is more specific than sensitive, it does not identify all cases of FMF. Although a positive MPT can be very useful.[9][10]
Genetics
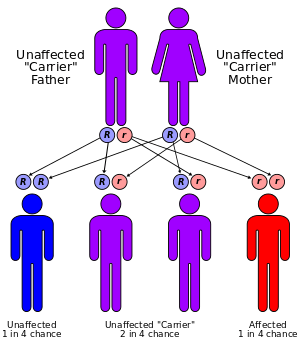
The MEFV gene is located on the short arm of chromosome 16 (16p13). Many different mutations of the MEFV gene can cause the disorder. Having one mutation is unlikely to cause the condition. Having two mutations either a copy from both parents, or two different mutations, one from each parent is the threshold for a genetic diagnosis of FMF. However, the bulk of individuals who comply with the genetic diagnosis of FMF remain asymptomatic or undiagnosed. Whether this is due to modifier genes or environmental factors remains to be established[11]
Treatment
Attacks are self-limiting, and require analgesia and NSAIDs (such as diclofenac).[8]
Colchicine, a drug otherwise mainly used in gout, decreases attack frequency in FMF patients. The exact way in which colchicine suppresses attacks is unclear. While this agent is not without side effects (such as abdominal pain and muscle pains), it may markedly improve quality of life in patients. The dosage is typically 1–2 mg a day. Development of amyloidosis is delayed with colchicine treatment. Interferon is being studied as a therapeutic modality.[8] Some advise discontinuation of colchicine before and during pregnancy, but the data are inconsistent, and others feel it is safe to take colchicine during pregnancy.[12]
Approximately 5–10% of FMF cases are resistant to colchicine therapy alone. In these cases, adding anakinra to the daily colchicine regimen has been successful.[13]
Epidemiology
FMF affects groups of people originating from around the Mediterranean Sea (hence its name). It is prominently present in the Armenians, Sephardi Jews (and, to a much lesser extent, Ashkenazi Jews), Cypriots, Turks, and Arabs.[8][14]
History
A New York allergist, Dr Sheppard Siegal, first described the attacks of peritonitis in 1945; he termed this "benign paroxysmal peritonitis", as the disease course was essentially benign.[15] Dr Hobart Reimann, working in the American University in Beirut, described a more complete picture which he termed "periodic disease".[16][17]
In 1972, colchicine was discovered to prevent attacks.[18]
The link to the MEFV gene was discovered in 1997 by two different groups, each working independently - the French FMF Consortium,[19] and the International FMF Consortium.[20]
See also
References
- ↑ Oxford Textbook of Medicine (4th ed.). Oxford: Oxford University Press. 2003. p. 159. ISBN 9780192629227.
- ↑ Unsal, Erbil (2006). Current Opinions in Pediatric Rheumatology. Hauppauge, N.Y.: Nova Science Publishers. p. 276. ISBN 9781594548710.
- ↑ James, William; Berger, Timothy; Elston, Dirk (2005). Andrews' Diseases of the Skin: Clinical Dermatology. (10th ed.). Saunders. ISBN 0-7216-2921-0.
- ↑ Chae JJ, Wood G, Richard K, et al. (September 2008). "The familial Mediterranean fever protein, pyrin, is cleaved by caspase-1 and activates NF-kappaB through its N-terminal fragment". Blood 112 (5): 1794–1803. doi:10.1182/blood-2008-01-134932. PMC 2518886. PMID 18577712.
- ↑ Dugdale III, David C; Jatin Vyas (2010-09-15). "Familial Mediterranean fever - PubMed Health". PubMed Health. National Centre for Biotechnology Information. Retrieved 2011-04-24.
- ↑ Siegal-Cattan-Mamou syndrome at Who Named It?
- ↑ "Familial Mediterranean fever - Genetics Home Reference". Genetics Home Reference. U.S. National Library of Medicine. 2011-04-14. Archived from the original on 2011-04-24. Retrieved 2011-04-24.
- 1 2 3 4 5 6 7 8 9 10 Livneh A, Langevitz P (2000). "Diagnostic and treatment concerns in familial Mediterranean fever". Baillieres Best Pract Res Clin Rheumatol 14 (3): 477–498. doi:10.1053/berh.2000.0089. PMID 10985982.
- ↑ Barakat MH, El-Khawad AO, Gumaa KA, El-Sobki NI, Fenech FF (1984). "Metaraminol provocative test: a specific diagnostic test for familial Mediterranean fever". Lancet 1 (8378): 656–7. doi:10.1016/s0140-6736(84)92172-x. PMID 6142351.
- ↑ Huppertz HI, Michels H (1988). "[The metaraminol provocation test in the diagnosis of familial Mediterranean fever]". Monatsschr Kinderheilkd 136 (5): 243–5. PMID 3405225.
- ↑ . Gershoni-Baruch, Ruth (August 2001). "Familial Mediterranean fever: prevalence, penetrance and genetic drift". European Journal of Human Genetics: http://www.nature.com/ejhg/journal/v9/n8/pdf/5200672a.pdf. doi:10.1038/sj.ejhg.5200672.
- ↑ Michael O, Goldman RD, Koren G (August 2003). "Safety of colchicine therapy during pregnancy". Can Fam Physician 49: 967–9. PMC 2214270. PMID 12943352.
- ↑ Calligaris L, Marchetti F, Tommasini A, Ventura A (2008). "The efficacy of anakinra in an adolescent with colchicine-resistant familial Mediterranean fever". European Journal of Pediatrics 167 (6): 695–696. doi:10.1007/s00431-007-0547-3. PMC 2292480. PMID 17588171.
- ↑ Sinha, Chandrasen K.; Davenport, Mark (2010). Handbook of Pediatric Surgery. New York: Springer. p. 192. ISBN 9781848821323.
- ↑ Siegal S (1945). "Benign paroxysmal peritonitis". Ann Intern Med 23 (2): 234–47. doi:10.7326/0003-4819-23-1-1. PMID 18124924.
- ↑ Reiman HA (1948). "Periodic disease. Probable syndrome including periodic fever, benign paroxysmal peritonitis, cyclic neutropenia and intermittent arthralgia". J Am Med Assoc 136 (4): 239–44. doi:10.1001/jama.1948.02890210023004. PMID 18920089.
- ↑ synd/2503 at Who Named It?
- ↑ Goldfinger, S.E. (1972-12-21). "Colchicine for familial Mediterranean fever". New England Journal of Medicine 287 (25): 1302. doi:10.1056/NEJM197212212872514. PMID 4636899.
- ↑ The French FMF Consortium (1997). "A candidate gene for familial Mediterranean fever". Nat. Genet. 17 (1): 25–31. doi:10.1038/ng0997-25. PMID 9288094.
- ↑ The International FMF Consortium (1997). "Ancient missense mutations in a new member of the RoRet gene family are likely to cause familial Mediterranean fever". Cell 90 (4): 797–807. doi:10.1016/S0092-8674(00)80539-5. PMID 9288758.
External links
- Proteopedia 2wl1 information about the MEFV gene.
- GeneReview/NIH/UW entry on Familial Mediterranean Fever
- Familial Mediterranean Fever (FMF) - US National Institute of Arthritis and Musculoskeletal and Skin Diseases
| ||||||||||||||||||||||||||||||||