Failed back syndrome
Failed back syndrome or post-laminectomy syndrome is a condition characterized by persistent pain following back surgeries.
Failed back syndrome (FBS), also called "failed back surgery syndrome" (FBSS), refers to chronic back and/or leg pain that occurs after back (spinal) surgery,[1][2] usually after laminectomy.[3] It is characterized as a chronic pain syndrome. Multiple factors can contribute to the onset or development of FBS. Contributing factors include but are not limited to residual or recurrent spinal disc herniation, persistent post-operative pressure on a spinal nerve, altered joint mobility, joint hypermobility with instability, scar tissue (fibrosis), depression, anxiety, sleeplessness and spinal muscular deconditioning. An individual may be predisposed to the development of FBS due to systemic disorders such as diabetes, autoimmune disease and peripheral blood vessels (vascular) disease.
Common symptoms associated with FBS include diffuse, dull and aching pain involving the back and/or legs. Abnormal sensibility may include sharp, pricking, and stabbing pain in the extremities. The term "post-laminectomy syndrome" is used by some doctors to indicate the same condition as failed back syndrome.
The treatments of post-laminectomy syndrome include physical therapy, low force specific chiropractic care, Microcurrent electrical neuromuscular stimulator,[4] minor nerve blocks, transcutaneous electrical nerve stimulation (TENS), behavioral medicine, non-steroidal anti-inflammatory (NSAID) medications, membrane stabilizers, antidepressants, spinal cord stimulation, and intrathecal morphine pump. Use of epidural steroid injections may be minimally helpful in some cases. The targeted anatomic use of a potent anti-inflammatory anti-TNF therapeutics is being investigated.
The number of spinal surgeries varies around the world. The United States and the Netherlands report the highest number of spinal surgeries, while the United Kingdom and Sweden report the fewest. Recently, there have been calls for more aggressive surgical treatment in Europe (see infra). Success rates of spinal surgery vary for many reasons.[5][6]
Cause

Patients who have undergone one or more operations on the lumbar spine, and continue to experience and report pain afterward can be divided into two groups. The first group are those in whom surgery was never indicated, or the surgery performed was never likely to achieve the desired result; and those in whom the surgery was indicated, but which technically did not achieve the intended result.[7] It has been observed that patients who have a predominant painful presentation in a radicular pattern will have a better result than those who have predominant complaints of back pain.
The second group includes patients who had incomplete or inadequate operations. Lumbar spinal stenosis may be overlooked, especially when it is associated with disc protrusion or herniation. Removal of a disc, while not addressing the underlying presence of stenosis can lead to disappointing results.[8] Occasionally operating on the wrong level occurs, as does failure to recognize an extruded or sequestered disc fragment. Inadequate or inappropriate surgical exposure can lead to other problems in not getting to the underlying pathology. Hakelius reported a 3% incidence of serious nerve root damage.[9]
In 1992, Turner et al. published a survey of 74 journal articles which reported the results after decompression for spinal stenosis. Good to excellent results were on average reported by 64% of the patients. There was, however, a wide variation in outcomes reported. There was a better result in patients who had a degenerative spondylolisthesis.[10] A similarly designed study by Mardjekto et al. found that a concomitant spinal arthrodesis (fusion) had a greater success rate.[11] Herron and Trippi evaluated 24 patients, all with degenerative spondylolisthesis treated with laminectomy alone. At follow-up varying between 18 to 71 months after surgery, 20 out of the 24 patients reported a good result.[12] Epstein reported on 290 patients treated over a 25-year period. Excellent results were obtained in 69% and good results in 13%.[13] However, these optimistic reports do not correlate with "return to competitive employment" rates, which for the most part are dismal in most spinal surgery series.
Studies by Cohen show that up to 25% of all low back pain is sacroiliac joint in origin and that the diagnosis of sacroiliac joint disease is frequently overlooked by physicians.[14] Studies by Ha, et al., show that the incidence of SI joint degeneration in post-lumbar fusion surgery is 75% at 5 years post-surgery, based on imaging.[15] Studies by DePalma and Liliang, et al., demonstrate that 40-61% of post-lumbar fusion patients were symptomatic for SI joint dysfunction based on diagnostic blocks.[16][17]
In the past two decades there has been a dramatic increase in fusion surgery in the U.S.: in 2001 over 122,000 lumbar fusions were performed, a 22% increase from 1990 in fusions per 100,000 population, increasing to an estimate of 250,000 in 2003, and 500,000 in 2006.[18][19][20] In 2003, the national bill for the hardware for fusion alone was estimated to have soared to $2.5 billion a year.[19][21] For patients with continued pain after surgery which is not due to the above complications or conditions, interventional pain physicians speak of the need to identify the "pain generator" i.e. the anatomical structure responsible for the patient's pain. To be effective, the surgeon must operate on the correct anatomic structure; however it is often not possible to determine the source of the pain.[22][23] The reason for this is that many patients with chronic pain often have disc bulges at multiple spinal levels and the physical examination and imaging studies are unable to pinpoint the source of pain.[22] In addition, spinal fusion itself, particularly if more than one spinal level is operated on, may result in "adjacent segment degeneration".[24] This is thought to occur because the fused segments may result in increased torsional and stress forces being transmitted to the intervertebral discs located above and below the fused vertebrae.[24] This pathology is one reason behind the development of artificial discs as a possible alternative to fusion surgery. But fusion surgeons argue that spinal fusion is more time-tested, and artificial discs contain metal hardware that is unlikely to last as long as biological material without shattering and leaving metal fragments in the spinal canal. These represent different schools of thought. (See discussion on disc replacement infra.)
Another highly relevant consideration is the increasing recognition of the importance of "chemical radiculitis" in the generation of back pain.[25] A primary focus of surgery is to remove "pressure" or reduce mechanical compression on a neural element: either the spinal cord, or a nerve root. But it is increasingly recognized that back pain, rather than being solely due to compression, may instead entirely be due to chemical inflammation of the nerve root. It has been known for several decades that disc herniations result in a massive inflammation of the associated nerve root.[25][26][27][28] In the past five years increasing evidence has pointed to a specific inflammatory mediator of this pain.[29][30] This inflammatory molecule, called tumor necrosis factor-alpha (TNF), is released not only by the herniated or protruding disc, but also in cases of disc tear (annular tear), by facet joints, and in spinal stenosis.[25][31][32][33] In addition to causing pain and inflammation, TNF may also contribute to disc degeneration.[34] If the cause of the pain is not compression, but rather is inflammation mediated by TNF, then this may well explain why surgery might not relieve the pain, and might even exacerbate it, resulting in FBSS.
Smoking
Recent studies have shown that cigarette smokers will routinely fail all spinal surgery, if the goal of that surgery is the decrease of pain and impairment. Many surgeons consider smoking to be an absolute contraindication to spinal surgery. Nicotine appears to interfere with bone metabolism through induced calcitonin resistance and decreased osteoblastic function. It may also restrict small blood vessel diameter leading to increased scar formation.[35][36][37][38][39][40][41]
There is an association between cigarette smoking, back pain and chronic pain syndromes of all types.[42][43][44][45][46]
In a report of 426 spinal surgery patients in Denmark, smoking was shown to have a negative effect on fusion and overall patient satisfaction, but no measurable influence on the functional outcome.[47]
There is a validation of the hypothetical assumption that postoperative smoking cessation helps to reverse the impact of cigarette smoking on outcome after spinal fusion. If patients cease cigarette smoking in the immediate post operative period, there is a positive impact on success.[48]
Regular smoking in adolescence was associated with low back pain in young adults. Pack-years of smoking showed an exposure-response relationship among girls.[49]
A recent study suggested that cigarette smoking adversely affects serum hydrocodone levels. Prescribing physicians should be aware that in some cigarette smokers, serum hydrocodone levels might not be detectable.[50]
In a study from Denmark reviewing many reports in the literature, it was concluded that smoking should be considered a weak risk indicator and not a cause of low back pain. In a multitude of epidemiologic studies, an association between smoking and low back pain has been reported, but variations in approach and study results make this literature difficult to reconcile.[51] In a massive study of 3482 patients undergoing lumbar spine surgery from the National Spine Network, comorbidities of (1) smoking, (2) compensation, (3) self reported poor overall health and (4) pre-existing psychological factors were predictive in a high risk of failure. Followup was carried out at 3 months and one year after surgery. Pre-operative depressive disorders tended not to do well.[52]
Smoking has been shown to increase the incidence of post operative infection as well as decrease fusion rates. One study showed 90% of post operative infections occurred in smokers, as well as myonecrosis (muscle destruction) around the wound.[53][54]
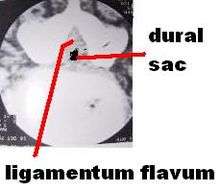
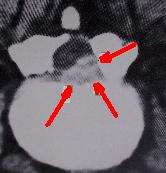
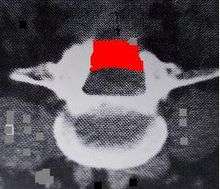
Pathology
Before the advent of CT scanning, the pathology in failed back syndrome was difficult to understand. Computerized tomography in conjunction with metrizamide myelography in the late 1960s and 1970s allowed direct observation of the mechanisms involved in post operative failures. Six distinct pathologic conditions were identified:
- Recurrent or persistent disc herniation
- Spinal stenosis
- Post operative infection
- Epidural post-operative fibrosis
- Adhesive arachnoiditis
- Nerve Injury
Recurrent or persistent disc herniation
Removal of a disc at one level can lead to disc herniation at a different level at a later time. Even the most complete surgical excision of the disc still leaves 30-40% of the disc, which cannot be safely removed. This retained disc can re-herniate sometime after surgery. Virtually every major structure in the abdomen and the posterior retroperitoneal space has been injured, at some point, by removing discs using posterior laminectomy/discectomy surgical procedures. The most prominent of these is a laceration of the left internal iliac vein, which lies in close proximity to the anterior portion of the disc.[55][56] In some studies, recurrent pain in the same radicular pattern or a different pattern can be as high as 50% after disc surgery.[57][58] Many observers have noted that the most common cause of a failed back syndrome is caused from recurrent disc herniation at the same level originally operated. A rapid removal in a second surgery can be curative. The clinical picture of a recurrent disc herniation usually involves a significant pain-free interval. However, physical findings may be lacking, and a good history is necessary.[59][60][61][62] The time period for the emergence of new symptoms can be short or long. Diagnostic signs such as the straight leg raise test may be negative even if real pathology is present.[58][63] The presence of a positive myelogram may represent a new disc herniation, but can also be indicative of a post operative scarring situation simply mimicking a new disc. Newer MRI imaging techniques have clarified this dilemma somewhat.[59][64][65][66][67][68] Conversely, a recurrent disc can be difficult to detect in the presence of post op scarring. Myelography is inadequate to completely evaluate the patient for recurrent disc disease, and CT or MRI scanning is necessary. Measurement of tissue density can be helpful.[8][65][69][70][71]
Even though the complications of laminectomy for disc herniation can be significant, a recent series of studies involving thousands of patients published under auspices of Dartmouth Medical School concluded at four-year follow-up that those who underwent surgery for a lumbar disc herniation achieved greater improvement than nonoperatively treated patients in all primary and secondary outcomes except work status.[72]
Spinal stenosis
Spinal stenosis can be a late complication after laminectomy for disc herniation or when surgery was performed for the primary pathologic condition of spinal stenosis.[8][73][74] In the Maine Study, among patients with lumbar spinal stenosis completing 8- to 10-year follow-up, low back pain relief, predominant symptom improvement, and satisfaction with the current state were similar in patients initially treated surgically or nonsurgically. However, leg pain relief and greater back-related functional status continued to favor those initially receiving surgical treatment.[75]
A large study of spinal stenosis from Finland found the prognostic factors for ability to work after surgery were ability to work before surgery, age under 50 years, and no prior back surgery. The very long-term outcome (mean follow-up time of 12.4 years) was excellent-to-good in 68% of patients (59% women and 73% men). Furthermore, in the longitudinal follow-up, the result improved between 1985 and 1991. No special complications were manifested during this very long-term follow-up time. The patients with total or subtotal block in preoperative myelography achieved the best result. Furthermore, patients with block stenosis improved their result significantly in the longitudinal follow-up. The postoperative stenosis seen in computed tomography (CT) scans was observed in 65% of 90 patients, and it was severe in 23 patients (25%). However, this successful or unsuccessful surgical decompression did not correlate with patients' subjective disability, walking capacity or severity of pain. Previous back surgery had a strong worsening effect on surgical results. This effect was very clear in patients with total block in the preoperative myelography. The surgical result of a patient with previous back surgery was similar to that of a patient without previous back surgery when the time interval between the last two operations was more than 18 months.[76]
Post-operative MRI findings of stenosis are probably of limited value compared to symptoms experienced by patients. Patients' perception of improvement had a much stronger correlation with long-term surgical outcome than structural findings seen on postoperation magnetic resonance imaging. Degenerative findings had a greater effect on patients' walking capacity than stenotic findings [77][78]
Postoperative radiologic stenosis was very common in patients operated on for lumbar spinal stenosis, but this did not correlate with clinical outcome. The clinician must be cautious when reconciling clinical symptoms and signs with postoperative computed tomography findings in patients operated on for lumbar spinal stenosis.[79]
A study from Georgetown University reported on one-hundred patients who had undergone decompressive surgery for lumbar stenosis between 1980 and 1985. Four patients with postfusion stenosis were included. A 5-year follow-up period was achieved in 88 patients. The mean age was 67 years, and 80% were over 60 years of age. There was a high incidence of coexisting medical diseases, but the principal disability was lumbar stenosis with neurological involvement. Initially there was a high incidence of success, but recurrence of neurological involvement and persistence of low-back pain led to an increasing number of failures. By 5 years this number had reached 27% of the available population pool, suggesting that the failure rate could reach 50% within the projected life expectancies of most patients. Of the 26 failures, 16 were secondary to renewed neurological involvement, which occurred at new levels of stenosis in eight and recurrence of stenosis at operative levels in eight. Reoperation was successful in 12 of these 16 patients, but two required a third operation. The incidence of spondylolisthesis at 5 years was higher in the surgical failures (12 of 26 patients) than in the surgical successes (16 of 64). Spondylolisthetic stenosis tended to recur within a few years following decompression. Because of age and associated illnesses, fusion may be difficult to achieve in this group.[80]
Post operative infection
A small minority of lumbar surgical patients will develop a post operative infection. In most cases, this is a bad complication and does not bode well for eventual improvement or future employability. Reports from the surgical literature indicate an infection rate anywhere from 0% to almost 12%.[81][82][83][84][85][86][87][88][89][90][91][92][93][94][95][96] The incidence of infection tends to increase as the complexity of the procedure and operating time increase. Usage of metal implants (instrumentation) tends to increase the risk of infection. Factors associated with an increased infection include diabetes mellitus, obesity, malnutrition, smoking, previous infection, rheumatoid arthritis, and immunodeficiency.[97][98][99][100][101][102] Previous wound infection should be considered as a contraindication to any further spinal surgery, since the likelihood of improving such patients with more surgery is small.[103][104][105][106][107][108] Antimicrobial prophylaxis (giving antibiotics during or after surgery before an infection begins) reduces the rate of surgical site infection in lumbar spine surgery, but a great deal of variation exists regarding its use. In a Japanese study, utilizing the Centers for Disease Control recommendations for antibiotic prophylaxis, an overall rate of 0.7% infection was noted, with a single dose antibiotic group having 0.4% infection rate and multiple dosage antibiotic infection rate of 0.8%. The authors had previously used prophylactic antibiotics for 5 to 7 postoperative days. Based on the Centers for Disease Control and Prevention guideline, their antibiotic prophylaxis was changed to the day of surgery only. It was concluded there was no statistical difference in the rate of infection between the two different antibiotic protocols. Based on the CDC guideline, a single dose of prophylactic antibiotic was proven to be efficacious for the prevention of infection in lumbar spine surgeries.[109]
Epidural post-operative fibrosis
Epidural scarring following a laminectomy for disc excision is a common feature when re-operating for recurrent sciatica or radiculopathy.[59] When the scarring is associated with a disc herniation and/or recurrent spinal stenosis, it is relatively common, occurring in more than 60% of cases. For a time, it was theorized that placing a fat graft over the dural could prevent post operative scarring. However, initial enthusiasm has waned in recent years.[110][111][112][113][114] In an extensive laminectomy involving 2 or more vertebra, post operative scarring is the norm. It is most often seen around the L5 and S1 nerve roots.[115][116][117]
Adhesive arachnoiditis

Fibrous scarring can also be a complication within the subarachnoid space. It is notoriously difficult to detect and evaluate. Prior to the development of magnetic resonance imaging, the only way to ascertain the presence of arachnoiditis was by opening the dura. In the days of CT scanning and Pantopaque and later, Metrizamide myelography, the presence of arachnoiditis could be speculated based on radiographic findings. Often, myelography prior to the introduction of Metrizamide was the cause of arachnoiditis. It can also be caused by the long term pressure brought about with either a severe disc herniation or spinal stenosis.[60][118][119][120][121] The presence of both epidural scarring and arachnoiditis in the same patient are probably quite common. Arachnoiditis is a broad term denoting inflammation of the meninges and subarachnoid space. A variety of etiologies exist, including infectious, inflammatory, and neoplastic processes. Infectious etiologies include bacterial, viral, fungal, and parasitic agents. Noninfectious inflammatory processes include surgery, intrathecal hemorrhage, and the administration of intrathecal (inside the dural canal) agents such as myelographic contrast media, anesthetics (e.g. chloroprocaine), and steroids (e.g. Depo-Medrol, Kenalog). Lately iatrogenic arachnoiditis has been attributed to misplaced Epidural Steroid Injection therapy when accidentally administered intrathecally. The preservatives and suspension agents found in all steroid injectates, which aren't indicated for epidural administration by the U.S. Food & Drug Administration due to reports of severe adverse events including arachnoiditis, paralysis and death, have now been directly linked to the onset of the disease following the initial stage of chemical meningitis.[122][123][124][125] Neoplasia includes the hematogenous spread of systemic tumors, such as breast and lung carcinoma, melanoma, and non-Hodgkin lymphoma. Neoplasia also includes direct seeding of the cerebrospinal fluid (CSF) from primary central nervous system (CNS) tumors such as glioblastoma multiforme, medulloblastoma, ependymoma, and choroid plexus carcinoma. Strictly speaking, the most common cause of arachnoiditis in failed back syndrome is not infectious or from cancer. It is due to non-specific scarring secondary to the surgery or the underlying pathology. [126][127][128][129][130][131][132][133]
Nerve injury
Laceration of a nerve root, or damage from cautery or traction can lead to chronic pain, however this can be difficult to determine. Chronic compression of the nerve root by a persistent agent such as disc, bone (osteophyte) or scarring can also permanently damage the nerve root. Epidural scarring caused by the initial pathology or occurring after the surgery can also contribute to nerve damage. In one study of failed back patients, the presence of pathology was noted to be at the same site as the level of surgery performed in 57% of cases. The remaining cases developed pathology at a different level, or on the opposite side, but at the same level as the surgery was performed. In theory, all failed back patients have some sort of nerve injury or damage which leads to a persistence of symptoms after a reasonable healing time.[57][58][134]
Management
Narcotics
Failed back syndrome (FBS) is a well-recognized complication of surgery of the lumbar spine. It can result in chronic pain and disability, often with disastrous emotional and financial consequences to the patient. Many patients have traditionally been classified as "spinal cripples" and are consigned to a life of long-term narcotic treatment with little chance of recovery. Despite extensive work in recent years, FBS remains a challenging and costly disorder.[135]
A Swedish study of chronic pain and iatrogenic opioid addiction was reported from the methadone program at the Uppsala University Hospital. The aims were to improve pain relief and quality of life in pain patients with problematic opioid use and to investigate background factors explaining problems with opioid use. Titration of oral methadone mixture in daily doses ranging from 10 to 350 mg was done on all patients. Background factors were low back and musculoskeletal pain in 40%, psychiatric disease in 68%, and substance use disorder in 32% of the patients. Before methadone treatment all patients were on sick leave. After treatment five patients returned to work. Ten patients failed treatment, 4 due to intractable nausea, 4 to drug diversion, 1 because of methadone related arrhythmia and 1 because of insufficient analgesia. Pain relief was rated good by 75% and moderate by 25% of the patients. Global quality of life was deemed to have improved, somewhat. It was concluded a structured methadone program can be used for treating chronic pain patients with opioid dependence improving pain relief and quality of life. However, side effects and serious adverse events may limit the beneficial effects of the method.[136]
A study of chronic pain patients from the University of Wisconsin found that methadone is most widely known for its use in the treatment of opioid dependence, but methadone also provides effective analgesia. Patients who experience inadequate pain relief or intolerable side effects with other opioids or who suffer from neuropathic pain may benefit from a transition to methadone as their analgesic agent. Adverse effects, particularly respiratory depression and death, make a fundamental knowledge of methadone's pharmacological properties essential to the provider considering methadone as analgesic therapy for a patient with chronic pain.[137] The beneficial experience of methadone usage in some chronic pain patients was also found in Canada.[138]
A recent Italian study examined the use of fentanyl patches, sustained release morphine and methadone in chronic pain patients with cancer. All the three opioids used as first-line therapy were effective, well tolerated, and required similar amounts of symptomatic drugs or co-analgesics. Methadone was significantly less expensive, but required more changes, up and down, of the doses, suggesting that dose titration of this drug requires major clinical expertise.[139]
Patient selection
Patients who have sciatic pain (pain in the back, radiating down the buttock to the leg) and clear clinical findings of an identifiable radicular nerve loss caused by a herniated disc will have a better post operative course than those who simply have low back pain. If a specific disc herniation causing pressure on a nerve root cannot be identified, the results of surgery are likely to be disappointing. Patients involved in worker's compensation, tort litigation or other compensation systems tend to fare more poorly after surgery. Surgery for spinal stenosis usually has a good outcome, if the surgery is done in an extensive manner, and done within the first year or so of the appearance of symptoms.[8][58][140][141][142]
Oaklander and North define the Failed Back Syndrome as a chronic pain patient after one or more surgical procedure to the spine. They delineated these characteristics of the relation between the patient and the surgeon:
- The patient makes increasing demands on the surgeon for pain relief. The surgeon may feel a strong responsibility to provide a remedy when the surgery has not achieved the desired goals.
- The patient grows increasingly angry at the failure and may become litigious.
- There is an escalation of narcotic pain medication which can be habituating or addictive.
- In the face of expensive conservative treatments which are likely to fail, the surgeon is persuaded to attempt further surgery, even though this is likely to fail as well.
- The probability of returning to gainful employment decreases with increasing length of disability.
- The financial incentives to remain disabled may be perceived as outweighing the incentive to recover.[143]
In the absence of a financial source for disability or worker's compensation, other psychological features may limit the ability of the patient to recover from surgery. Some patients are simply unfortunate, and fall into the category of "chronic pain" despite their desire to recover and the best efforts of the physicians involved in their care.[144][145][146][147][148][149][150][151][152][153][154] Even less invasive forms of surgery are not uniformly successful; approximately 30,000-40,000 laminectomy patients obtain either no relief of symptomatology or a recurrence of symptoms.[155] Another less invasive form of spinal surgery, percutaneous disc surgery, has reported revision rates as high as 65%.[156] It is no surprise, therefore, that FBSS is a significant medical concern which merits further research and attention by the medical and surgical communities.[22][23]
Total disc replacement
Lumbar total disc replacement was originally designed to be an alternative to lumbar arthodesis (fusion). The procedure was met with great excitement and heightened expectations both in the United States and Europe. In late 2004, the first lumbar total disc replacement received approval from the U.S. Food and Drug Administration (FDA). More experience existed in Europe. Since then, the initial excitement has given way to skepticism and concern.[157][158][159][160][161][162][163] Various failure rates and strategies for revision of total disc replacement have been reported.[164]
The role of artificial or total disc replacement in the treatment of spinal disorders remains ill-defined and unclear.[165] Evaluation of any new technique is difficult or impossible because physician experience may be minimal or lacking. Patient expectations may be distorted.[166][167] It has been difficult to establish clear cut indications for artificial disc replacement. It may not be a replacement procedure or alternative to fusion, since recent studies have shown that 100% of fusion patients had one or more contraindications to disc replacement.[168][169][170] The role of disc replacement must come from new indications not defined in today's literature or a relaxation of current contraindications.[165]
A study by Regan [171] found the result of replacement was the same at L4-5 and L5-S1 with the CHARITE disc. However, the ProDisc II had more favorable results at L4-5 compared with L5-S1.[172]
A younger age was predictive of a better outcome in several studies.[162][173][174] In others it has been found to be a negative predictor or of no predictive value.[175][176][177][178][179] Older patients may have more complications.[180]
Prior spinal surgery has mixed effects on disc replacement. It has been reported to be negative in several studies.[175][181][182][183][184][185] It has been reported to have no effect in other studies.[186][187][188][189][190][191] Many studies are simply inconclusive.[175] Existing evidence does not allow drawing definite conclusions about the status of disc replacement at present.[165]
Electrical stimulation
Many failed back patients are significantly impaired by chronic pain in the back and legs. Many of these will be treated with some form of electrical stimulation. This can be either a transcutaneous electrical nerve stimulation device placed on the skin over the back or a nerve stimulator implanted into the back with electrical probes which directly touch the spinal cord. Also, some chronic pain patients utilize fentanyl or narcotic patches. These patients are generally severely impaired and it is unrealistic to conclude that application of neurostimulation will reduce that impairment. For example, it is doubtful that neurostimulation will improve the patient enough to return to competitive employment. Neurostimulation is palliative. TENS units work by blocking neurotransmission as described by the pain theory of Melzack and Wall.[192] Success rates for implanted neurostimulation has been reported to be 25% to 55%. Success is defined as a relative decrease in pain.[193]
Prognosis
Under rules promulgated by Titles II and XVI of the United States Social Security Act, chronic radiculopathy, arachnoiditis and spinal stenosis are recognized as disabling conditions under Listing 1.04 A (radiculopathy), 1.04 B (arachnoiditis) and 1.04 C (spinal stenosis). [194][195]
Return to work

In a groundbreaking Canadian study, Waddell et al.[196] reported on the value of repeat surgery and the return to work in worker's compensation cases. They concluded that workers who undergo spinal surgery take longer to return to their jobs. Once two spinal surgeries are performed, few if any ever return to gainful employment of any kind. After two spinal surgeries, most people in the worker's comp system will not be made better by more surgery. Most will be worse after a third surgery.
Episodes of back pain associated with on the job injuries in the worker's compensation setting are usually of short duration. About 10% of such episodes will not be simple, and will degenerate into chronic and disabling back pain conditions, even if surgery is not performed.[197][198]
It has been hypothesized that job dissatisfaction and individual perception of physical demands are associated with an increased time of recovery or an increased risk of no recovery at all.[199] Individual psychological and social work factors, as well as worker-employer relations are also likely to be associated with time and rates of recovery.[200][201][202]
A Finnish study of return to work in patients with spinal stenosis treated by surgery found that: (1) none of the patients who had retired before the operation returned to work afterward. (2) The variables that predicted postoperative ability to work for women were: being fit to work at the time of operation, age < 50 years at the time of operation, and duration of lumbar spinal stenosis symptoms < 2 years. (3) For men, these variables were: being fit to work at the time of operation, age < 50 years at the time of operation, no prior surgery, and the extent of the surgical procedure equal to or less than one laminectomy. Women's and men's working capacity do not differ after lumbar spinal stenosis operation. If the aim is to maximize working capacity, then, when a lumbar spinal stenosis operation is indicated, it should be performed without delay. In lumbar spinal stenosis patients who are > 50 years old and on sick leave, it is unrealistic to expect that they will return to work. Therefore, after such an extensive surgical procedure, re-education of patients for lighter jobs could improve the chances of these patients returning to work.[203]
In a related Finnish study, a total of 439 patients operated on for lumbar spinal stenosis during the period 1974-1987 was re-examined and evaluated for working and functional capacity approximately 4 years after the decompressive surgery. The ability to work before or after the operation and a history of no prior back surgery were variables predictive of a good outcome. Before the operation 86 patients were working, 223 patients were on sick leave, and 130 patients were retired. After the operation 52 of the employed patients and 70 of the unemployed patients returned to work. None of the retired patients returned to work. Ability to work preoperatively, age under 50 years at the time of operation and the absence of prior back surgery predicted a postoperative ability to work.[204]
A report from Belgium noted that patients reportedly return to work an average of 12 to 16 weeks after surgery for lumbar disc herniation. However, there are studies that lend credence to the value of an earlier stimulation for return to work and performance of normal activities after a limited discectomy. At follow-up assessment, it was found that no patient had changed employment because of back or leg pain. The sooner the recommendation is made to return to work and perform normal activities, the more likely the patient is to comply. Patients with ongoing disabling back conditions have a low priority for return to work. The probability of return to work decreases as time off work increases. This is especially true in Belgium, where 20% of individuals did not resume work activities after surgery for a disc herniation of the lumbar spine.
In Belgium, the medical advisers of sickness funds have an important role legally in the assessment of working capacity and medical rehabilitation measures for employees whose fitness for work is jeopardized or diminished for health reasons. The measures are laid down in the sickness and invalidity legislation. They are in accordance with the principle of preventing long-term disability. It is apparent from the authors' experience that these measures are not adapted consistently in medical practice. Most of the medical advisers are focusing purely on evaluation of corporal damage, leaving little or no time for rehabilitation efforts. In many other countries, the evaluation of work capacity is done by social security doctors with a comparable task.[205]
In a comprehensive set of studies carried out by the University of Washington School of Medicine, it was determined that the outcome of lumbar fusion performed on injured workers was worse than reported in most published case series. They found 68% of lumbar fusion patients still unable to return to work two years after surgery. This was in stark contrast to reports of 68% post-op satisfaction in many series.[206][207] In a follow-up study it was found that the use of intervertebral fusion devices rose rapidly after their introduction in 1996. This increase in metal usage was associated with a greater risk of complication without improving disability or re-operation rates.[208][209][210][211]
Research
The identification of tumor necrosis factor-alpha (TNF) as a central cause of inflammatory spinal pain now suggests the possibility of an entirely new approach to selected patients with FBSS. Specific and potent inhibitors of TNF became available in the U.S. in 1998, and were demonstrated to be potentially effective for treating sciatica in experimental models beginning in 2001.[212][213][214] Targeted anatomic administration of one of these anti-TNF agents, etanercept, a patented treatment method,[215] has been suggested in published pilot studies to be effective for treating selected patients with chronic disc-related pain and FBSS.[216][217] The scientific basis for pain relief in these patients is supported by the many current review articles.[218][219] In the future new imaging methods may allow non-invasive identification of sites of neuronal inflammation, thereby enabling more accurate localization of the "pain generators" responsible for symptom production. These treatments are still experimental.
If chronic pain in FBSS has a chemical component producing inflammatory pain, then prior to additional surgery it may make sense to use an anti-inflammatory approach. Often this is first attempted with non-steroidal anti-inflammatory medications, but the long-term use of Non-steroidal anti-inflammatory drugs (NSAIDS) for patients with persistent back pain is complicated by their possible cardiovascular and gastrointestinal toxicity; and NSAIDs have limited value to intervene in TNF-mediated processes.[23] An alternative often employed is the injection of cortisone into the spine adjacent to the suspected pain generator, a technique known as "epidural steroid injection".[220] Although this technique began more than a decade ago for FBSS, the efficacy of epidural steroid injections is now generally thought to be limited to short term pain relief in selected patients only.[221] In addition, epidural steroid injections, in certain settings, may result in serious complications.[222] Fortunately there are now emerging new methods that directly target TNF.[216] These TNF-targeted methods represent a highly promising new approach for patients with chronic severe spinal pain, such as those with FBSS.[216] Ancillary approaches, such as rehabilitation, physical therapy, anti-depressants, and, in particular, graduated exercise programs, may all be useful adjuncts to anti-inflammatory approaches.[23] In addition, more invasive modalities, such as spinal cord stimulation, may offer relief for certain patients with FBSS, but these modalities, although often referred to as "minimally invasive", require additional surgery, and have complications of their own.[223][224]
Worldwide perspective

A report from Spain noted that the investigation and development of new techniques for instrumented surgery of the spine is not free from conflicts of interest. The influence of financial forces in the development of new technologies and its immediate application to spine surgery, shows the relationship between the published results and the industry support. Authors who have developed and defended fusion techniques have also published new articles praising new spinal technologies. The author calls spinal surgery the "American Stock and Exchange" and "the bubble of spine surgery". The scientific literature doesn't show clear evidence in the cost-benefit studies of most instrumented surgical interventions of the spine compared with the conservative treatments. It has not been yet demonstrated that fusion surgery and disc replacement are better options than the conservative treatment. It's necessary to point out that at present "there are relationships between the industry and back pain, and there is also an industry of the back pain". Nonetheless, the "market of the spine surgery" is growing because patients are demanding solutions for their back problems. The tide of scientific evidence seems to go against the spinal fusions in the degenerative disc disease, discogenic pain and in specific back pain. After decades of advances in this field, the results of spinal fusions are mediocre. New epidemiological studies show that "spinal fusion must be accepted as a non proved or experimental method for the treatment of back pain". The surgical literature on spinal fusion published in the last 20 years establishes that instrumentation seems to slightly increase the fusion rate and that instrumentation doesn't improve the clinical results in general. We still are in need of randomized studies to compare the surgical results with the natural history of the disease, the placebo effect, or conservative treatment. The European Guidelines for lumbar chronic pain management show "strong evidence" indicating that complex and demanding spine surgery where different instrumentation is used, is not more effective than a simple, safer and cheaper posterolateral fusion without instrumentation. Recently, the literature published in this field is sending a message to use "minimally invasive techniques"; - the abandonment of transpedicular fusions. Surgery in general, and usage of metal fixation should be discarded in most cases.[225]
In Sweden, the national registry of lumbar spine surgery reported in the year 2000 that 15% of patients with spinal stenosis surgery underwent a concomitant fusion.[226] Despite the traditionally conservative approach to spinal surgery in Sweden, there have been calls from that country for a more aggressive approach to lumbar procedures in recent years.
Cherkin et al.,[227] evaluated worldwide surgical attitudes. There were twice the number of surgeons per capita in the United States compared to the United Kingdom. Numbers were similar to Sweden. Despite having very few spinal surgeons, the Netherlands proved to be quite aggressive in surgery. Sweden, despite having a large number of surgeons was conservative and produced relatively few surgeries. The most surgeries were done in the United States. In the UK, more than a third of non-urgent patients waited over a year to see a spinal surgeon. In Wales, more than half waited over three months for consult. Lower rates of referrals in the United Kingdom was found to discourage surgery in general. Fee for service and easy access to care was thought to encourage spinal surgery in the United States, whereas salaried position and a conservative philosophy led to less surgery in the United Kingdom. There were more spinal surgeons in Sweden than in the United States. However, it was speculated that the Swedish surgeons being limited to compensation of 40–48 hours a week might lead to a conservative philosophy. It should be noted that there have been calls for a more aggressive approach to lumbar surgery in both the United Kingdom and Sweden in recent years.[71][228][229]
References
- ↑ Long DM (Oct 1991). "Failed back surgery syndrome". Neurosurg Clin N Am. 2 (4): 899–919. PMID 1840393.
- ↑ Fritsch EW, Heisel J, Rupp S (Mar 1996). "The failed back surgery syndrome: reasons, intraoperative findings, and long-term results: a report of 182 operative treatments". Spine 21 (5): 626–33. doi:10.1097/00007632-199603010-00017. PMID 8852320.
- ↑ "Conditions of the Spine - Post Laminectomy Syndrome". 2010. Retrieved 10 Sep 2014.
- ↑ Lee PB, Kim YC, Lim YJ, et al. (2006). "Efficacy of pulsed electromagnetic therapy for chronic lower back pain: a randomized, double-blind, placebo-controlled study". The Journal of International Medical Research 34 (2): 160–7. doi:10.1177/147323000603400205. PMID 16749411.
- ↑ Slipman CW, Shin CH, Patel RK, et al. (Sep 2002). "Etiologies of failed back surgery syndrome". Pain Med 3 (3): 200–14; discussion 214–7. doi:10.1046/j.1526-4637.2002.02033.x. PMID 15099254.
- ↑ Taylor VM, Deyo RA, Cherkin DC, Kreuter W (Jun 1994). "Low back pain hospitalization. Recent United States trends and regional variations". Spine 19 (11): 1207–12; discussion 13. doi:10.1097/00007632-199405310-00002. PMID 8073311.
- ↑ Fager C. A., Freiberg S. R. (1980). "Analysis of failures and poor results of lumbar spine surgery.". Spine 5 (1): 87–94. doi:10.1097/00007632-198001000-00015. PMID 7361201.
- 1 2 3 4 Burton CV, Kirkaldy-Willis WH, Yong-Hing K, Heithoff KB (June 1981). "Causes of failure of surgery on the lumbar spine". Clin. Orthop. Relat. Res. (157): 191–9. doi:10.1097/00003086-198106000-00032. PMID 7249453.
- ↑ Hakelius A (1970). "Prognosis in sciatica. A clinical follow-up of surgical and non-surgical treatment". Acta Orthop Scand Suppl 129: 1–76. PMID 5269867.
- ↑ Turner J, et al. (1992). "Surgery for lumbar spinal stenosis. Attempted meta-analysis of the literature.". Spine 17 (1): 1–8. doi:10.1097/00007632-199201000-00001. PMID 1531550.
- ↑ Mardjetko SM, Connolly PJ, Shott S (October 1994). "Degenerative lumbar spondylolisthesis. A meta-analysis of literature 1970–1993". Spine 19 (20 Suppl): 2256S–2265S. doi:10.1097/00007632-199410151-00002. PMID 7817240.
- ↑ Herron L. D., Trippi A. C. (1989). "L4-5 degenerative spondylolisthesis. The results of treatment by decompressive laminectomy without fusion.". Spine 14 (5): 534–538. doi:10.1097/00007632-198905000-00013. PMID 2727798.
- ↑ Epstein N. E. (1998). "Decompression in the surgical management of degenerative spondylolisthesis: advantages of a conservative approach in 290 patients.". J. Spinal Disorder 11 (2): 116–122. doi:10.1097/00002517-199804000-00004. PMID 9588467.
- ↑ Cohen Steven P (2005). "Sacroiliac Joint Pain: a Comprehensive Review of Anatomy, Diagnosis, and Treatment". Anesthesia and Analgesia 101 (5): 1440–1453. doi:10.1213/01.ane.0000180831.60169.ea.
- ↑ Ha, Kee-Yong, Jun-Seok Lee, and Ki-Won Kim. "Degeneration of Sacroiliac Joint After Instrumented Lumbar or Lumbosacral Fusion: a Prospective Cohort Study over Five-year Follow-up." Spine 33, no. 11 (May 15, 2008) 1192–1198.
- ↑ DePalma MJ, Ketchum JM, Saullo TR (May 2011). "Etiology of chronic low back pain in patients having undergone lumbar fusion". Pain Medicine 12 (5): 732–9. doi:10.1111/j.1526-4637.2011.01098.x. PMID 21481166.
- ↑ Liliang, Po-Chou, Kang Lu, Cheng-Loong Liang, Yu-Duan Tsai, Kuo-Wei Wang, and Han-Jung Chen. "Sacroiliac Joint Pain After Lumbar and Lumbosacral Fusion: Findings Using Dual Sacroiliac Joint Blocks." Pain Medicine (Malden, Mass.) 12, no. 4 (April 2011) 565–570.
- ↑ Deyo RA, Gray DT, Kreuter W, Mirza S, Martin BI (Jun 2005). "United States trends in lumbar fusion surgery for degenerative conditions". Spine 30 (12): 1441–5; discussion 1446–7. doi:10.1097/01.brs.0000166503.37969.8a. PMID 15959375.
- 1 2 Abelson R, Petersen M (December 31, 2003). "An operation to ease back pain bolsters the bottom line, too". New York Times. Retrieved January 8, 2011.
- ↑ Abelson R (December 30, 2006). "Surgeons invest in makers of hardware". New York Times. Retrieved January 8, 2011.
- ↑ Guyer RD, Patterson M, Ohnmeiss DD (Sep 2006). "Failed back surgery syndrome: diagnostic evaluation". J Am Acad Orthop Surg 14 (9): 534–43. PMID 16959891.
- 1 2 3 Deyo RA (Jul 2002). "Diagnostic evaluation of LBP: reaching a specific diagnosis is often impossible". Arch Intern Med. 162 (13): 1444–7; discussion 1447–8. doi:10.1001/archinte.162.13.1444. PMID 12090877.
- 1 2 3 4 Carragee EJ (May 2005). "Clinical practice. Persistent low back pain". N Engl J Med. 352 (18): 1891–8. doi:10.1056/NEJMcp042054. PMID 15872204.
- 1 2 Levin DA, Hale JJ, Bendo JA (2007). "Adjacent segment degeneration following spinal fusion for degenerative disc disease". Bull NYU Hosp Jt Dis 65 (1): 29–36. PMID 17539759.
- 1 2 3 Peng B, Wu W, Li Z, Guo J, Wang X (Jan 2007). "Chemical radiculitis". Pain 127 (1–2): 11–6. doi:10.1016/j.pain.2006.06.034. PMID 16963186.
- ↑ Marshall LL, Trethewie ER (Aug 1973). "Chemical irritation of nerve-root in disc prolapse". Lancet 2 (7824): 320. doi:10.1016/S0140-6736(73)90818-0. PMID 4124797.
- ↑ McCarron RF, Wimpee MW, Hudkins PG, Laros GS (Oct 1987). "The inflammatory effect of nucleus pulposus. A possible element in the pathogenesis of low-back pain". Spine 12 (8): 760–4. doi:10.1097/00007632-198710000-00009. PMID 2961088.
- ↑ Takahashi H, Suguro T, Okazima Y, Motegi M, Okada Y, Kakiuchi T (Jan 1996). "Inflammatory cytokines in the herniated disc of the lumbar spine". Spine 21 (2): 218–24. doi:10.1097/00007632-199601150-00011. PMID 8720407.
- ↑ Igarashi T, Kikuchi S, Shubayev V, Myers RR (Dec 2000). "2000 Volvo Award winner in basic science studies: Exogenous tumor necrosis factor-alpha mimics nucleus pulposus-induced neuropathology. Molecular, histologic, and behavioral comparisons in rats". Spine 25 (23): 2975–80. doi:10.1097/00007632-200012010-00003. PMID 11145807.
- ↑ Sommer C, Schafers M (Dec 2004). "Mechanisms of neuropathic pain: the role of cytokines". Drug Discovery Today: Disease Mechanisms 1 (4): 441–8. doi:10.1016/j.ddmec.2004.11.018.
- ↑ Igarashi A, Kikuchi S, Konno S, Olmarker K (Oct 2004). "Inflammatory cytokines released from the facet joint tissue in degenerative lumbar spinal disorders". Spine 29 (19): 2091–5. doi:10.1097/01.brs.0000141265.55411.30. PMID 15454697.
- ↑ Sakuma Y, Ohtori S, Miyagi M, et al. (Aug 2007). "Up-regulation of p55 TNF alpha-receptor in dorsal root ganglia neurons following lumbar facet joint injury in rats". Eur Spine J 16 (8): 1273–8. doi:10.1007/s00586-007-0365-3. PMC 2200776. PMID 17468886.
- ↑ Sekiguchi M, Kikuchi S, Myers RR (May 2004). "Experimental spinal stenosis: relationship between degree of cauda equina compression, neuropathology, and pain". Spine 29 (10): 1105–11. doi:10.1097/00007632-200405150-00011. PMID 15131438.
- ↑ Séguin CA, Pilliar RM, Roughley PJ, Kandel RA (Sep 2005). "Tumor necrosis factor-alpha modulates matrix production and catabolism in nucleus pulposus tissue". Spine 30 (17): 1940–8. doi:10.1097/01.brs.0000176188.40263.f9. PMID 16135983.
- ↑ Frymoyer J. W.; et al. (1983). "Risk factors in low-back pain. An epidemiological survey" (PDF). J. Bone Joint Surg. 65A (2): 213–218. PMID 6218171.
- ↑ Deyo R. A., Bass J. E. (1989). "Lifestyle and low-back pain. The influence of smoking and obesity". Spine 14 (5): 501–506. doi:10.1097/00007632-198905000-00005. PMID 2524888.
- ↑ Svensson H. O.; et al. (1983). "Low-back pain in relation to other diseases and cardiovascular risk factors". Spine 8 (3): 277–285. doi:10.1097/00007632-198304000-00008. PMID 6226118.
- ↑ De Vernejoul M.C.; et al. (1989). "Evidence for defective osteoblastic function. A role for alcohol and tobacco consumption in osteoporosis in middle-aged men". Clin. Orthop 179 (179): 107–115. doi:10.1097/00003086-198310000-00016. PMID 6617002.
- ↑ An H. S.; et al. (1994). "Comparison of smoking habits between patients with surgically confirmed herniated lumbar and cervical disc disease and controls". J. Spinal Disord 7 (5): 369–373. doi:10.1097/00002517-199410000-00001. PMID 7819635.
- ↑ Hollo I, Gergely I, Boross M (June 1977). "Smoking results in calcitonin resistance". JAMA 237 (23): 2470. doi:10.1001/jama.1977.03270500022008. PMID 576955.
- ↑ Iwahashi M, et al. (2002). "Mechanism of intervertebral disc degeneration caused by nicotine in rabbits to explicate intervertebral disc disorders caused by smoking". Spine 27 (13): 1396–1401. doi:10.1097/00007632-200207010-00005. PMID 12131735.
- ↑ Biering-Sorensen F., Thomsen C. (1986). "Medical, social and occupational history as risk indicators for low-back trouble in a general population". Spine 11 (7): 720–5. doi:10.1097/00007632-198609000-00011. PMID 2947336.
- ↑ Boshuizen H, et al. (1993). "Do smokers get more back pain?". Spine 18 (1): 35–40. doi:10.1097/00007632-199301000-00007. PMID 8434323.
- ↑ Deyo R. A.; et al. (1989). "Lifestyle and low-back pain. The influence of smoking and obesity". Spine 14 (5): 501–506. doi:10.1097/00007632-198905000-00005. PMID 2524888.
- ↑ Heliovaara M, et al. (1991). "Determinants of sciatica and low-back pain". Spine 16 (6): 608–14. doi:10.1097/00007632-199106000-00002. PMID 1830689.
- ↑ Heliovaara M, et al. (1989). "Risk factors for low back pain and sciatica". Annals of Medicine 21 (4): 257–64. doi:10.3109/07853898909149202. PMID 2528971.
- ↑ Andersen T, et al. (2001). "Smoking as a Predictor of Negative Outcome in Lumbar Spinal Fusion". Spine 26 (23): 2623–28. doi:10.1097/00007632-200112010-00018. PMID 11725245.
- ↑ Glassman S. D.; et al. (2000). "The Effect of Cigarette Smoking and Smoking Cessation on Spinal Fusion". Spine 25 (20): 2608–15. doi:10.1097/00007632-200010150-00011. PMID 11034645.
- ↑ Mikkonen P, et al. (2008). "Is smoking a risk factor for low back pain in adolescents? A prospective cohort study". Spine 33 (5): 527–32. doi:10.1097/BRS.0b013e3181657d3c. PMID 18317198.
- ↑ Ackerman W. E., Ahmad M. (2007). "Effect of cigarette smoking on serum hydrocodone levels in chronic pain patients". J. Ark. Med. Soc. 104 (1): 19–21. PMID 17663288.
- ↑ Leboeuf-Yde C. (1999). "Smoking and low back pain. A systematic literature review of 41 journal articles reporting 47 epidemiologic studies". Spine 24 (14): 1463–70. doi:10.1097/00007632-199907150-00012. PMID 10423792.
- ↑ Slover J, et al. (2006). "The Impact of Comorbidities on the Change in Short-Form 36 and Oswestry Scores Following Lumbar Spine Surgery". Spine 31 (17): 1974–1988. doi:10.1097/01.brs.0000229252.30903.b9. PMID 16924216.
- ↑ Porter SE, Hanley EN (2001). "The musculoskeletal effects of smoking". J Am Acad Orthop Surg 9 (1): 9–17. PMID 11174159.
- ↑ Thalgott J. S.; et al. (1991). "Postoperative infections in spinal implants. Classification and analysis--a multicenter study". Spine 16 (8): 981–984. doi:10.1097/00007632-199108000-00020. PMID 1948385.
- ↑ Linton R. R., White P. D. (1945). "Arteriovenous Fistula Between The Right Common Iliac Artery And The Inferior Vena Cava". Arch. Surg. 50 (1): 6–13. doi:10.1001/archsurg.1945.01230030009002.
- ↑ Epps C. H. (1978). Complications in Orthopedic Surgery. Philadelphia: Lippincott and Co. pp. 1009–1037. ISBN 978-0-397-50382-7.
- 1 2 Cauchoix J, Ficat C, Girard B (1978). "Repeat Surgery After Disc Excision". Spine 3 (3): 256–59. doi:10.1097/00007632-197809000-00011. PMID 152469.
- 1 2 3 4 Weir B.K.A., Jacobs G. A. (1980). "Reoperation rate following lumbar discectomy. An analysis of 662 lumbar discectomies". Spine 5 (4): 366–70. doi:10.1097/00007632-198007000-00010. PMID 7455766.
- 1 2 3 Benoist M, et al. (1980). "Postoperative Lumbar Epiduro-Arachnoiditis". Spine 5 (5): 432–35. doi:10.1097/00007632-198009000-00007. PMID 6450453.
- 1 2 Benner B., Ehni G. (1978). "Spinal arachnoiditis. The postoperative variety in particular". Spine 3 (1): 40–44. doi:10.1097/00007632-197803000-00009. PMID 644391.
- ↑ Rothman R (1975). Orhop. Clin. North Amer. 6: 305–310. ISSN 0030-5898. Missing or empty
|title=(help) - ↑ Quiles M, Marchisello PJ, Tsairis P (March 1978). "Lumbar adhesive arachnoiditis. Etiologic and pathologic aspects". Spine 3 (1): 45–50. doi:10.1097/00007632-197803000-00010. PMID 644392.
- ↑ Spangfort EV (1972). "The lumbar disc herniation. A computer-aided analysis of 2,504 operations". Acta Orthop Scand Suppl 142: 1–95. PMID 4516334.
- ↑ Bener B., Ehni G. (1978). "Spinal arachnoiditis. The postoperative variety in particular". Spine 3 (1): 40–44. doi:10.1097/00007632-197803000-00009. PMID 644391.
- 1 2 Byrd S. E.; et al. (1985). "The radiographic evaluation of the symptomatic postoperative lumbar spine patient". Spine 10 (7): 652–61. doi:10.1097/00007632-198509000-00011. PMID 2933827.
- ↑ Deburge A., Badelon O. (1982). "Failure of the surgical treatment of common non-paralyzing disk sciaticas. A symposium" [Failure of the surgical treatment of common non-paralyzing disk sciaticas. A symposium]. Rev. Chir. Orthop (in French) 68 (4): 249–54. PMID 6217514.
- ↑ Irstam L (1984). "Differential diagnosis of recurrent lumbar disc herniation and postoperative deformation by myelography. An impossible task". Spine 9 (7): 759–63. doi:10.1097/00007632-198410000-00019. PMID 6505846.
- ↑ Thibierge M., Metzger J. (1982). "Failure of the surgical treatment of common non-paralyzing disk sciaticas. A symposium" [Failure of the surgical treatment of common non-paralyzing disk sciaticas. A symposium]. Rev. Chir. Orthop. (in French) 68 (4): 230–33. PMID 6217514.
- ↑ Massare C (1982). "Failure of the surgical treatment of common non-paralyzing disk sciaticas. A symposium" [Failure of the surgical treatment of common non-paralyzing disk sciaticas. A symposium]. Rev. Chir. Orthop 68 (4): 233–46. PMID 6217514.
- ↑ Teplik J. G., Haskin M. E. (1984). "Intravenous contrast-enhanced CT of the postoperative lumbar spine: improved identification of recurrent disk herniation, scar, arachnoiditis, and diskitis". AJR. American journal of roentgenology 143 (4): 845–55. doi:10.2214/ajr.143.4.845. PMID 6332496.
- 1 2 Deyo RA, Nachemson A, Mirza SK (Feb 2004). "Spinal-fusion surgery – the case for restraint". N Engl J Med. 350 (7): 722–6. doi:10.1056/NEJMsb031771. PMID 14960750.
- ↑ Weinstein J. N.; et al. (2008). "Surgical versus nonoperative treatment for lumbar disc herniation: four-year results for the Spine Patient Outcomes Research Trial (SPORT)". Spine 33 (25): 2789–2800. doi:10.1097/BRS.0b013e31818ed8f4. PMC 2756172. PMID 19018250.
- ↑ Crock H. V. (1976). "Observations on the management of failed spinal operations". J. Bone Joint Surg. 58B (2): 193–199. PMID 932081.
- ↑ Crock, H. V. Practice of Spinal Surgery, Vienna/New York; Springer Verlag, 1983
- ↑ Atlas S. J.; et al. (2005). "The Efficacy of Corticosteroids in Periradicular Infiltration for Chronic Radicular Pain". Spine 30 (8): 857–9. doi:10.1097/01.brs.0000158878.93445.a0.
- ↑ Herno A (1995). "Surgical results of lumbar spinal stenosis". Ann Chir Gynaecol Suppl 210: 1–969. PMID 8546434.
- ↑ Herno A, et al. (1999). "Long-term clinical and magnetic resonance imaging follow-up assessment of patients with lumbar spinal stenosis after laminectomy". Spine 24 (15): 1533–7. doi:10.1097/00007632-199908010-00006. PMID 10457572.
- ↑ Herno A, et al. (1999). "The degree of decompressive relief and its relation to clinical outcome in patients undergoing surgery for lumbar spinal stenosis". Spine 24 (10): 1010–4. doi:10.1097/00007632-199905150-00015. PMID 10332794.
- ↑ Herno A, et al. (1999). "Computed tomography findings 4 years after surgical management of lumbar spinal stenosis. No correlation with clinical outcome". Spine 24 (21): 2234–9. doi:10.1097/00007632-199911010-00011. PMID 10562990.
- ↑ Caputy A. J., Luessenhop A. J. (1992). "Long-term evaluation of decompressive surgery for degenerative lumbar stenosis". J. Neurosurg 77 (5): 669–76. doi:10.3171/jns.1992.77.5.0669. PMID 1403105.
- ↑ Sponseller P. D.; et al. (2000). "Deep wound infections after neuromuscular scoliosis surgery: a multicenter study of risk factors and treatment outcomes". Spine 25 (19): 2461–2466. doi:10.1097/00007632-200010010-00007. PMID 11013497.
- ↑ Weinstein M. A.; et al. (2000). "Postoperative spinal wound infection: a review of 2,391 consecutive index procedures". J. Spinal Disord 13: 422–426. doi:10.1097/00002517-200010000-00009.
- ↑ Massie JB, Heller JG, Abitbol JJ, McPherson D, Garfin SR (November 1992). "Postoperative posterior spinal wound infections". Clin. Orthop. Relat. Res. (284): 99–108. doi:10.1097/00003086-199211000-00013. PMID 1395319.
- ↑ Rechtine G. R.; et al. (2001). "Postoperative Wound Infection after Instrumentation of Thoracic and Lumbar Fractures". J. Ortho. Trauma 15 (8): 566–569. doi:10.1097/00005131-200111000-00006.
- ↑ Eck KR, Bridwell KH, Ungacta FF, et al. (May 2001). "Complications and results of long adult deformity fusions down to l4, l5, and the sacrum". Spine 26 (9): E182–92. doi:10.1097/00007632-200105010-00012. PMID 11337635.
- ↑ Capen D. A.; et al. (1996). "Perioperative risk factors for wound infections after lower back fusions". Orthop. Clin. North. Am. 27 (1): 83–86. PMID 8539055.
- ↑ Hee H. T.; et al. (2001). "Anterior/posterior lumbar fusion versus transforaminal lumbar interbody fusion: analysis of complications and predictive factors". J. Spinal Disord 14 (6): 533–540. doi:10.1097/00002517-200112000-00013. PMID 11723406.
- ↑ Aydinli U, et al. (1999). "Postoperative deep wound infection in instrumented spinal surgery". Acta Orthop. Belg. 65 (2): 182–187. PMID 10427800.
- ↑ Wimmer C, et al. (1998). "Influence of antibiotics on infection in spinal surgery: a prospective study of 110 patients". J. Spinal Disord 11 (6): 498–500. doi:10.1097/00002517-199812000-00008. PMID 9884294.
- ↑ Wimmer C, Gluch H, Franzreb M, Ogon M (April 1998). "Predisposing factors for infection in spine surgery: a survey of 850 spinal procedures". J Spinal Disord 11 (2): 124–8. doi:10.1097/00002517-199804000-00006. PMID 9588468.
- ↑ Hodges SD, Humphreys SC, Eck JC, Covington LA, Kurzynske NG (December 1998). "Low postoperative infection rates with instrumented lumbar fusion". South. Med. J. 91 (12): 1132–6. doi:10.1097/00007611-199812000-00007. PMID 9853725.
- ↑ Perry J. W.; et al. (1997). "Wound infections following spinal fusion with posterior segmental spinal instrumentation". Clin. Infect. Dis. 24 (4): 558–561. doi:10.1093/clind/24.4.558. PMID 9145726.
- ↑ Abbey D. M.; et al. (1995). "Treatment of postoperative wound infections following spinal fusion with instrumentation". J. Spinal. Disord 8 (4): 278–283. doi:10.1097/00002517-199508040-00003. PMID 8547767.
- ↑ West J. L.; et al. (1991). "Complications of the variable screw plate pedicle screw fixation". Spine 16 (5): 576–579. doi:10.1097/00007632-199105000-00016. PMID 2053001.
- ↑ Esses SI, Sachs BL, Dreyzin V (November 1993). "Complications associated with the technique of pedicle screw fixation. A selected survey of ABS members". Spine 18 (15): 2231–8; discussion 2238–9. doi:10.1097/00007632-199311000-00015. PMID 8278838.
- ↑ Dave S. H., Meyers D. L. (1992). "Complications of Lumbar Spinal Fusion with Transpedicular Instrumentation". Spine 17 (Suppl 6): S184–189. doi:10.1097/00007632-199206001-00021.
- ↑ Andreshak T. G.; et al. (1997). "Lumbar spine surgery in the obese patient". J. Spinal Disord 10 (5): 376–379. doi:10.1097/00002517-199710000-00003. PMID 9355052.
- ↑ Viola R. W.; et al. (1997). "Point of View: Delayed Infection After Elective Spinal Instrumentation and Fusion". Spine 22 (20): 2450–2451. doi:10.1097/00007632-199710150-00024.
- ↑ Klein J. D.; et al. (1996). "Perioperative nutrition and postoperative complications in patients undergoing spinal surgery". Spine 21 (22): 2676–2682. doi:10.1097/00007632-199611150-00018. PMID 8961455.
- ↑ Swank S.M.; et al. (1981). "Surgical treatment of adult scoliosis. A review of two hundred and twenty-two cases". The Journal of bone and joint surgery. American volume 63 (2): 268–87. PMID 6450768.
- ↑ Klein J. D., Garfin S. R. (1996). "Nutritional status in the patient with spinal infection". Orthop. Clin. North. Am. 27 (1): 33–36. PMID 8539050.
- ↑ Heary R. F.; et al. (1994). "HIV status does not affect microbiologic spectrum or neurologic outcome in spinal infections". Surg. Neurol 42 (5): 417–423. doi:10.1016/0090-3019(94)90350-6. PMID 7974148.
- ↑ Bertrand G (January 1975). "The "battered" root problem". Orthop. Clin. North Am. 6 (1): 305–10. PMID 1113977.
- ↑ Depalma and Rothman, The Intervertebral Disc, Philadelphia, W. B. Saunders, 1970
- ↑ Finnegan W., Rothman R.; et al. (1975). "The American Academy of Orthopaedic Surgeons" (PDF). J. Bone Joint Surg. 57A (7): 1022–1035 [1034].
- ↑ Ghormley RK (1957). "The problem of multiple operations on the back". Instr Course Lect 14: 56–63. PMID 13524946.
- ↑ Greenwood J, McGuire Th, Kimbell F (January 1952). "A study of the causes of failure in the herniated intervertebral disc operation; an analysis of sixty-seven reoperated cases". J. Neurosurg. 9 (1): 15–20. doi:10.3171/jns.1952.9.1.0015. PMID 14908634.
- ↑ Hirsch C (1965). "Efficiency Of Surgery In Low-back Disorders. Pathoanatomical, Experimental, And Clinical Studies". J. Bone Joint Surg. 47A: 991–1004. PMID 14318637.
- ↑ Kanayama M, et al. (2007). "Effective prevention of surgical site infection using a Centers for Disease Control and Prevention guideline-based antimicrobial prophylaxis in lumbar spine surgery". J. Neurosurg. Spine 6 (4): 327–9. doi:10.3171/spi.2007.6.4.7. PMID 17436921.
- ↑ Langenskold A., Valle M. (1976). "Prevention of epidural scar formation after operations on the lumbar spine by means of free fat transplants. A preliminary report". Clin. Orthop 115 (115): 92–95. doi:10.1097/00003086-197603000-00015. PMID 1253503.
- ↑ La Rocca H., Macnab I. (1974). "The laminectomy membrane. Studies in its evolution, characteristics, effects and prophylaxis in dogs". J. Bone Joint Surgery 56B (3): 545–50. PMID 4421702.
- ↑ Law J. D.; et al. (1978). "Reoperation after lumbar intervertebral disc surgery". J. Neurosurgery 48 (2): 259–63. doi:10.3171/jns.1978.48.2.0259.
- ↑ Lee C. K., Alexander H. (1984). "Prevention of postlaminectomy scar formation". Spine 9 (3): 305–12. doi:10.1097/00007632-198404000-00016. PMID 6729595.
- ↑ Lehmann TR, LaRocca HS (1981). "Repeat lumbar surgery. A review of patients with failure from previous lumbar surgery treated by spinal canal exploration and lumbar spinal fusion". Spine 6 (6): 615–9. doi:10.1097/00007632-198111000-00014. PMID 6461073.
- ↑ Lähde S, Puranen J (August 1985). "Disk-space hypodensity in CT: the first radiological sign of postoperative diskitis". Eur J Radiol 5 (3): 190–2. PMID 4029155.
- ↑ Hinton JL, Warejcka DJ, Mei Y, et al. (1995). "Inhibition of epidural scar formation after lumbar laminectomy in the rat". Spine 20 (5): 564–570. doi:10.1097/00007632-199503010-00011. PMID 7604326.
- ↑ Fischgrund J. S. (2000). "Perspectives on modern orthopaedics: use of Adcon-L for epidural scar prevention". J. Am. Acad. Orthop. Surg. 8 (6): 339–343. PMID 11104397.
- ↑ Benoit M, et al. (1980). "Postoperative Lumbar Epiduro-Arachnoiditis". Spine 5 (5): 432–35. doi:10.1097/00007632-198009000-00007. PMID 6450453.
- ↑ Brodsky A. E. (1978). "Chronic spinal arachnoiditis. A postoperative syndrome that may signal its onset". Spine 3 (1): 88–91. doi:10.1097/00007632-197803000-00017. PMID 644396.
- ↑ Burton C. V. (1978). "Lumbosacral arachnoiditis". Spine 3 (1): 24–30. doi:10.1097/00007632-197803000-00006. PMID 148106.
- ↑ Quiles M, et al. (1978). "Lumbar adhesive arachnoiditis. Etiologic and pathologic aspects". Spine 3 (1): 45–50. doi:10.1097/00007632-197803000-00010. PMID 644392.
- ↑ US/FDA DepoMedrol DataSheet 2010
- ↑ Dermot R. Fitzgibbon, MD | ASA Closed Claims Project | Anesthesiology | year = 2004
- ↑ Lima, Navarro, "et al." Clinical And Histological Effects of Intrathecal Administration of MPA in Dogs | year = 2010 | Pain Physician
- ↑ authors = D A Nelson, W M Landau | Neurol Neurosurgery Psychiatry | year = 2001 | Intraspinal Steroids: History, Efficacy, Accidentality, and Controversy with Review of United States Food & Drug Administration Reports
- ↑ Brammah TB, Jayson MI (November 1994). "Syringomyelia as a complication of spinal arachnoiditis". Spine 19 (22): 2603–5. doi:10.1097/00007632-199411001-00019. PMID 7855688.
- ↑ Georgy B. A.; et al. (1996). "MR imaging of spinal nerve roots: techniques, enhancement patterns, and imaging findings". AJR Am. J. Roentgenol 166 (1): 173–9. doi:10.2214/ajr.166.1.8571871. PMID 8571871.
- ↑ Gero B, et al. (1991). "MR imaging of intradural inflammatory diseases of the spine". AJNR Am. J. Neuroradiol 12 (5): 1009–19. PMID 1950896.
- ↑ Gupta R. K.; et al. (1994). "MRI in intraspinal tuberculosis". Neuroradiology 36 (1): 39–43. doi:10.1007/BF00599194. PMID 8107996.
- ↑ Johnson CE, Sze G (1990). "Benign lumbar arachnoiditis: MR imaging with gadopentetate dimeglumine". AJNR Am J Neuroradiol 11 (4): 763–70. PMID 2114765.
- ↑ Muñoz A, Hinojosa J, Esparza J (May 2007). "Cisternography and ventriculography gadopentate dimeglumine-enhanced MR imaging in pediatric patients: preliminary report". AJNR Am J Neuroradiol 28 (5): 889–94. PMID 17494664.
- ↑ Sharma A, et al. (1997). "MR imaging of tubercular spinal arachnoiditis". AJR Am. J. Roentgenol 168 (3): 807–12. doi:10.2214/ajr.168.3.9057539. PMID 9057539.
- ↑ Tali E. T.; et al. (2002). "Intrathecal gadolinium (gadopentetate dimeglumine) enhanced magnetic resonance myelography and cisternography: results of a multicenter study". Invest. Radiol 37 (3): 152–9. doi:10.1097/00004424-200203000-00008. PMID 11882795.
- ↑ Yong H. K.; et al. (1980). "Prevention of nerve root adhesions after laminectomy". Spine 5 (1): 59–64. doi:10.1097/00007632-198001000-00011. PMID 7361199.
- ↑ Onesti S. T. (2004). "Failed back syndrome". Neurologist 10 (5): 259–64. doi:10.1097/01.nrl.0000138733.09406.39. PMID 15335443.
- ↑ Rhodin A, et al. (2006). "Methadone treatment of chronic non-malignant pain and opioid dependence--a long-term follow-up". Eur. J. Pain 10 (3): 271–8. doi:10.1016/j.ejpain.2005.05.003. PMID 15972261.
- ↑ Brown R, et al. (2004). "Methadone: applied pharmacology and use as adjunctive treatment in chronic pain". Postgrad. Med. J. 80 (949): 654–9. doi:10.1136/pgmj.2004.022988. PMC 1743125. PMID 15537850.
- ↑ Gardner-Nix J. S. (1996). "Oral methadone for managing chronic nonmalignant pain". J. Pain Symptom Manage 11 (5): 321–8. doi:10.1016/0885-3924(95)00191-3. PMID 8636630.
- ↑ Mercandante S, et al. (2008). "Sustained-release oral morphine versus transdermal fentanyl and oral methadone in cancer pain management". Eur. J. Pain 12 (8): 1040–6. doi:10.1016/j.ejpain.2008.01.013. PMID 18353696.
- ↑ Spengler D. M.; et al. (1980). "Low-back pain following multiple lumbar spine procedures. Failure of initial selection?". Spine 5 (4): 356–60. doi:10.1097/00007632-198007000-00008. PMID 6450449.
- ↑ Wiltse LL, Rocchio PD (1975). "Preoperative psychological tests as predictors of success of chemonucleolysis in the treatment of the low-back syndrome" (PDF). J. Bone Joint Surg. 57A (4): 478–83. PMID 124736.
- ↑ Weir BK (March 1979). "Prospective study of 100 lumbosacral discectomies". J. Neurosurg. 50 (3): 283–9. doi:10.3171/jns.1979.50.3.0283. PMID 422980.
- ↑ Oaklnader, A. L., and North, R. B. "Failed back surgery syndrome" In Loeser, J. D., et al., eds. Bonica's Management of Pain, Philadelphia, Lippincott Williams & Williams, 2001
- ↑ Haider TT, Kishino ND, Gray TP, Tomlin MA, Daubert HB (1998). "Functional restoration: Comparison of surgical and nonsurgical spine patients". J. Occup. Rehabil 8 (4): 247–253. ISSN 1053-0487.
- ↑ Tandon V; Campbell, F; Ross, ER (1999). "Posterior lumbar interbody fusion. Association between disability and psychological disturbance in noncompensation patients". Spine 24 (17): 1833–1838. doi:10.1097/00007632-199909010-00013. PMID 10488514.
- ↑ Turner J, et al. (1992). "Patient outcomes after lumbar spinal fusions". JAMA 268 (7): 907–911. doi:10.1001/jama.268.7.907. PMID 1640622.
- ↑ Malter A. D.; et al. (1996). "Cost-effectiveness of lumbar discectomy for the treatment of herniated intervertebral disc". Spine 21 (9): 1048–1055. doi:10.1097/00007632-199605010-00011. PMID 8724089.
- ↑ Dvorak J, et al. (1988). "The outcome of surgery for lumbar disc herniation. I. A 4-17 years' follow-up with emphasis on somatic aspects". Spine 13 (12): 1418–1422. doi:10.1097/00007632-198812000-00015. PMID 3212575.
- ↑ Deyo R, et al. (1992). "Morbidity and mortality in association with operations on the lumbar spine. The influence of age, diagnosis, and procedure". J. Bone Joint Surg. 74A (4): 536–543. PMID 1583048.
- ↑ Gervitz R. N.; et al. (1996). "Psychophysiologic treatment of chronic lower back pain". Prof. Psychol. Res. Pract 27 (6): 561–566. doi:10.1037/0735-7028.27.6.561.
- ↑ Graver V, Haaland AK, Magnaes B, Loeb M (April 1999). "Seven-year clinical follow-up after lumbar disc surgery: results and predictors of outcome". Br J Neurosurg 13 (2): 178–84. doi:10.1080/02688699943952. PMID 10616588.
- ↑ De Groot K. I.; et al. (1997). "The influence of psychological variables on postoperative anxiety and physical complaints in patients undergoing lumbar surgery". Pain 69 (1–2): 19–25. doi:10.1016/S0304-3959(96)03228-9. PMID 9060008.
- ↑ Schade V, et al. (1999). "The impact of clinical, morphological, psychosocial and work-related factors on the outcome of lumbar discectomy". Pain 80 (1–2): 239–249. doi:10.1016/S0304-3959(98)00210-3. PMID 10204736.
- ↑ Rosenstiel A., Keefe F. (1983). "The use of coping strategies in chronic low back pain patients: Relationship to patient characteristics and current adjustment". Pain 17 (1): 33–40. doi:10.1016/0304-3959(83)90125-2. PMID 6226916.
- ↑ Keane GP (1997). "Failed low back surgery syndrome". In Herring SA, Cole AJ. The low back pain handbook: a practical guide for the primary care clinician. Philadelphia: Hanley & Belfus. pp. 269–81. ISBN 1-56053-152-5.
- ↑ Chatterjee S, Foy PM, Findlay GF (Mar 1995). "Report of a controlled clinical trial comparing automated percutaneous lumbar discectomy and microdiscectomy in the treatment of contained lumbar disc herniation". Spine 20 (6): 734–8. doi:10.1097/00007632-199503150-00016. PMID 7604351.
- ↑ Fritzell P, et al. (2001). "2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group". Spine 26 (23): 2521–32. doi:10.1097/00007632-200112010-00002. PMID 11725230.
- ↑ LeHuec J. C.; et al. (2005). "Clinical results of Maverick lumbar total disc replacement: two-year prospective follow-up". Orthop. Clin. North Am. 36 (3): 315–22. doi:10.1016/j.ocl.2005.02.001. PMID 15950691.
- ↑ Guyer RD, McAfee PC, Hochschuler SH, et al. (2004). "Prospective randomized study of the Charite artificial disc: data from two investigational centers". Spine J 4 (6 Suppl): 252S–259S. doi:10.1016/j.spinee.2004.07.019. PMID 15541674.
- ↑ Blumenthal S, McAfee PC, Guyer RD, et al. (July 2005). "A prospective, randomized, multicenter Food and Drug Administration investigational device exemptions study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part I: evaluation of clinical outcomes". Spine 30 (14): 1565–75; discussion E387–91. doi:10.1097/01.brs.0000170587.32676.0e. PMID 16025024.
- ↑ McAfee PC, Cunningham B, Holsapple G, et al. (July 2005). "A prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of lumbar total disc replacement with the CHARITE artificial disc versus lumbar fusion: part II: evaluation of radiographic outcomes and correlation of surgical technique accuracy with clinical outcomes". Spine 30 (14): 1576–83; discussion E388–90. doi:10.1097/01.brs.0000170561.25636.1c. PMID 16025025.
- 1 2 Zeegers W. S.; et al. (1999). "Artificial disc replacement with the modular type SB Charité III: 2-year results in 50 prospectively studied patients". Eur. Spine J. 8 (3): 210–17. doi:10.1007/s005860050160. PMID 10413347.
- ↑ Putzier M, Funk JF, Schneider SV, et al. (February 2006). "Charité total disc replacement--clinical and radiographical results after an average follow-up of 17 years". Eur Spine J 15 (2): 183–95. doi:10.1007/s00586-005-1022-3. PMC 3489410. PMID 16254716.
- ↑ Patel A. A.; et al. (2008). "Revision strategies in lumbar total disc arthroplasty". Spine 33 (11): 1276–1283. doi:10.1097/BRS.0b013e3181714a1d. PMID 18469704.
- 1 2 3 Zindrick M. R.; et al. (2008). "An evidence-based medicine approach in determining factors that may affect outcome in lumbar total disc replacement". Spine 33 (11): 1262–1269. doi:10.1097/BRS.0b013e318171454c. PMID 18469702.
- ↑ Straus, S., et al. "Evidence Based Medicine, 3rd ed." London; Elsevier Churchill Livingstone, 2005
- ↑ Sackett, D. L., et al., "Evidence-Based Medicine. How to Practice and Teach EBM", New York:: Churchill Livingstone, 2000
- ↑ Lemaire J. P.; et al. (2005). "Clinical and radiological outcomes with the Charité artificial disc: a 10-year minimum follow-up". J. Spinal Disord. Tech. 18 (4): 353–9. doi:10.1097/01.bsd.0000172361.07479.6b. PMID 16021017.
- ↑ Huang R. C.; et al. (2004). "The prevalence of contraindications to total disc replacement in a cohort of lumbar surgical patients". Spine 29 (22): 2538–41. doi:10.1097/01.brs.0000144829.57885.20. PMID 15543070.
- ↑ Wong D. A.; et al. (2007). "Incidence of contraindications to total disc arthroplasty: a retrospective review of 100 consecutive fusion patients with a specific analysis of facet arthrosis". Spine J. 7 (1): 5–11. doi:10.1016/j.spinee.2006.04.012. PMID 17197326.
- ↑ Regan J. J. (2005). "Clinical results of charité lumbar total disc replacement". Orthop. Clin. North Am. 36 (3): 323–40. doi:10.1016/j.ocl.2005.03.005. PMID 15950692.
- ↑ Siepe C. J.; et al. (2007). "Total lumbar disc replacement: different results for different levels". Spine 32 (7): 782–90. doi:10.1097/01.brs.0000259071.64027.04. PMID 17414914.
- ↑ Siepe CJ, Mayer HM, Wiechert K, Korge A (August 2006). "Clinical results of total lumbar disc replacement with ProDisc II: three-year results for different indications". Spine 31 (17): 1923–32. doi:10.1097/01.brs.0000228780.06569.e8. PMID 16924209.
- ↑ Le Huec JC, Basso Y, Aunoble S, Friesem T, Bruno MB (June 2005). "Influence of facet and posterior muscle degeneration on clinical results of lumbar total disc replacement: two-year follow-up". J Spinal Disord Tech 18 (3): 219–23. PMID 15905763.
- 1 2 3 Tropiano P, et al. (2005). "Lumbar Total Disc Replacement. Seven to Eleven-Year Follow-Up". J. Bone Joint Surg. 87A (3): 490–6. doi:10.2106/JBJS.C.01345. PMID 15741612.
- ↑ Sott A. H., Harrison D. J. (2000). "Increasing age does not affect good outcome after lumbar disc replacement". Int Orthop 24 (1): 50–3. doi:10.1007/s002640050013. PMID 10774864.
- ↑ Chung S. S.; et al. (2006). "Lumbar total disc replacement using ProDisc II: a prospective study with a 2-year minimum follow-up". J. Spinal. Disord. Tech. 19 (6): 411–5. doi:10.1097/00024720-200608000-00007. PMID 16891976.
- ↑ Bertagnoli R, et al. (2006). "Lumbar total disc arthroplasty in patients older than 60 years of age: a prospective study of the ProDisc prosthesis with 2-year minimum follow-up period". J Neurosurg. Spine 4 (2): 85–90. doi:10.3171/spi.2006.4.2.85. PMID 16506473.
- ↑ Tropiano P, et al. (2003). "Lumbar disc replacement: preliminary results with ProDisc II after a minimum follow-up period of 1 year". J. Spinal Disord. Tech. 16 (4): 362–8. doi:10.1097/00024720-200308000-00008. PMID 12902952.
- ↑ Bertagnoli R, et al. (2006). "Lumbar total disc arthroplasty in patients older than 60 years of age: a prospective study of the ProDisc prosthesis with 2-year minimum follow-up period". J. Neurosurg. Spine 4 (2): 85–90. doi:10.3171/spi.2006.4.2.85. PMID 16506473.
- ↑ David T (2007). "Long-term results of one-level lumbar arthroplasty: minimum 10-year follow-up of the CHARITE artificial disc in 106 patients". Spine 32 (6): 661–6. doi:10.1097/01.brs.0000257554.67505.45. PMID 17413471.
- ↑ Cinotti G, et al. (1996). "Results of disc prosthesis after a minimum follow-up period of 2 years". Spine 21 (8): 995–1000. doi:10.1097/00007632-199604150-00015. PMID 8726204.
- ↑ Bertagnoli; et al. (2005). "The treatment of disabling multilevel lumbar discogenic low back pain with total disc arthroplasty utilizing the ProDisc prosthesis: a prospective study with 2-year minimum follow-up". Spine 30 (19): 2192–9. doi:10.1097/01.brs.0000181061.43194.18. PMID 16205346.
- ↑ Tropiano P, et al. (2003). "Lumbar disc replacement: preliminary results with ProDisc II after a minimum follow-up period of 1 year". J. Spinal Disord. Tech. 16 (4): 362–8. doi:10.1097/00024720-200308000-00008. PMID 12902952.
- ↑ Le Huec J. C. (2005). "Influence of facet and posterior muscle degeneration on clinical results of lumbar total disc replacement: two-year follow-up". J. Spinal Disord. Tech. 18 (3): 219–23. PMID 15905763.
- ↑ Lemaire J. P.; et al. (1997). "Intervertebral Disc Prosthesis: Results and Prospects for the Year 2000". Clin Orthop. Rel. Res. 337: 64–76. doi:10.1097/00003086-199704000-00009.
- ↑ Siepe C. J.; et al. (2006). "Clinical results of total lumbar disc replacement with ProDisc II: three-year results for different indications". Spine 31 (17): 1923–32. doi:10.1097/01.brs.0000228780.06569.e8. PMID 16924209.
- ↑ Chung S. S.; et al. (2006). "Lumbar total disc replacement using ProDisc II: a prospective study with a 2-year minimum follow-up". J. Spinal. Disord. Tech. 19 (6): 411–5. doi:10.1097/00024720-200608000-00007. PMID 16891976.
- ↑ Bertagnoli R, Yue JJ, Shah RV, et al. (October 2005). "The treatment of disabling multilevel lumbar discogenic low back pain with total disc arthroplasty utilizing the ProDisc prosthesis: a prospective study with 2-year minimum follow-up". Spine 30 (19): 2192–9. doi:10.1097/01.brs.0000181061.43194.18. PMID 16205346.
- ↑ Mayer H. M.; et al. (2002). "Minimally invasive total disc replacement: surgical technique and preliminary clinical results". Eur. Spine J. 11 (Suppl 2): S124–30. doi:10.1007/s00586-002-0446-2. PMID 12384733.
- ↑ Zeegers W. S.; et al. (1999). "Artificial disc replacement with the modular type SB Charité III: 2-year results in 50 prospectively studied patients". Eur. Spine J. 8 (3): 210–7. doi:10.1007/s005860050160. PMID 10413347.
- ↑ Wang JK (January 1976). "Stimulation-produced analgesia". Mayo Clin. Proc. 51 (1): 28–30. PMID 765636.
- ↑ de la Porte C, Siegfried J (September 1983). "Lumbosacral spinal fibrosis (spinal arachnoiditis). Its diagnosis and treatment by spinal cord stimulation". Spine 8 (6): 593–603. doi:10.1097/00007632-198309000-00005. PMID 6228017.
- ↑ Social Security; "Disability Evaluation Under Social Security", June 2006
- ↑ http://www.ssa.gov/disability/professionals/bluebook/adultlistings.pdf
- ↑ Waddell G, et al. (1979). "Failed lumbar disc surgery and repeat surgery following industrial injuries". J. Bone Joint Surgery 61A (2): 201–206. PMID 422604.
- ↑ Waddell G. (1998). The Back Pain Revolution (1st ed.). London: Churchill Livingstone. ISBN 978-0-443-06039-7.
- ↑ Litton S., van Tulder M. (2001). "A Picture is Worth a Thousand Words". Spine 26 (4): 339–44. doi:10.1097/00007632-200102150-00007.
- ↑ Mielenz T. J.; et al. (2008). "Association of psychosocial work characteristics with low back pain outcomes". Spine 33 (11): 1270–1275. doi:10.1097/BRS.0b013e31817144c3. PMID 18469703.
- ↑ Hoogendoorn W. E.; et al. (2000). "Systematic review of psychosocial factors at work and private life as risk factors for back pain". Spine 25 (16): 2114–25. doi:10.1097/00007632-200008150-00017. PMID 10954644.
- ↑ Davis K., Heaney C. (2000). "The relationship between psychosocial work characteristics and low back pain: underlying methodological issues". Clin. Biomech 15 (6): 389–406. doi:10.1016/S0268-0033(99)00101-1.
- ↑ Linton S, et al. (1994). "Psychological factors related to health, back pain, and dysfunction". J. Occup. Rehab 4 (1): 1–10. doi:10.1007/BF02109992.
- ↑ Herno A, et al. (1996). "Pre- and postoperative factors associated with return to work following surgery for lumbar spinal stenosis". Am. J. Ind. Med. 30 (4): 473–8. doi:10.1002/(SICI)1097-0274(199610)30:4<473::AID-AJIM13>3.0.CO;2-1. PMID 8892553.
- ↑ Airaksinen O, et al. (1994). "Surgical treatment of lumbar spinal stenosis: patients' postoperative disability and working capacity". Eur Spine J. 3 (5): 261–4. doi:10.1007/BF02226576. PMID 7866848.
- ↑ Donceel P, Du Bois M, Lahaye D (May 1999). "Return to work after surgery for lumbar disc herniation. A rehabilitation-oriented approach in insurance medicine". Spine 24 (9): 872–6. doi:10.1097/00007632-199905010-00007. PMID 10327508.
- ↑ Franklin GM, Haug J, Heyer NJ, McKeefrey SP, Picciano JF (September 1994). "Outcome of lumbar fusion in Washington State workers' compensation". Spine 19 (17): 1897–903; discussion 1904. doi:10.1097/00007632-199409000-00005. PMID 7997921.
- ↑ Turner JA, Ersek M, Herron L, et al. (August 1992). "Patient outcomes after lumbar spinal fusions". JAMA 268 (7): 907–11. doi:10.1001/jama.268.7.907. PMID 1640622.
- ↑ Maghout-Juratli S, et al. (2006). "Lumbar fusion outcomes in Washington State workers' compensation". Spine 31 (23): 2715–2723. doi:10.1097/01.brs.0000244589.13674.11. PMID 17077741.
- ↑ Romano P. S.; et al. (2002). "Can administrative data be used to ascertain clinically significant postoperative complications?". Am. J. Med. Qual. 17 (4): 145–54. doi:10.1177/106286060201700404. PMID 12153067.
- ↑ Murphy P. L., Volinn E. (1999). "Is occupational low back pain on the rise?". Spine 24 (7): 691–7. doi:10.1097/00007632-199904010-00015. PMID 10209800.
- ↑ Greenough C. G., Fraser R. D. (1989). "The effects of compensation on recovery from low-back injury". Spine 14 (9): 947–55. doi:10.1097/00007632-198909000-00006. PMID 2528824.
- ↑ Sommer C, Schäfers M, Marziniak M, Toyka KV (June 2001). "Etanercept reduces hyperalgesia in experimental painful neuropathy". Journal of the Peripheral Nervous System 6 (2): 67–72. doi:10.1046/j.1529-8027.2001.01010.x. PMID 11446385.
- ↑ Olmarker K, Rydevik B (Apr 2001). "Selective inhibition of tumor necrosis factor-alpha prevents nucleus pulposus-induced thrombus formation, intraneural edema, and reduction of nerve conduction velocity: possible implications for future pharmacologic treatment strategies of sciatica". Spine 26 (8): 863–9. doi:10.1097/00007632-200104150-00007. PMID 11317106.
- ↑ Murata Y, Onda A, Rydevik B, Takahashi K, Olmarker K (Nov 2004). "Selective inhibition of tumor necrosis factor-alpha prevents nucleus pulposus-induced histologic changes in the dorsal root ganglion". Spine 29 (22): 2477–84. doi:10.1097/01.brs.0000144406.17512.ea. PMID 15543058.
- ↑ U.S. Patent 6,537,549 and others
- 1 2 3 Tobinick EL, Britschgi-Davoodifar S (Mar 2003). "Perispinal TNF-alpha inhibition for discogenic pain". Swiss Med Wkly 133 (11–12): 170–7. PMID 12715286.
- ↑ Tobinick E, Davoodifar S (Jul 2004). "Efficacy of etanercept delivered by perispinal administration for chronic back and/or neck disc-related pain: a study of clinical observations in 143 patients". Curr Med Res Opin 20 (7): 1075–85. doi:10.1185/030079903125004286. PMID 15265252.
- ↑ Myers RR, Campana WM, Shubayev VI (Jan 2006). "The role of neuroinflammation in neuropathic pain: mechanisms and therapeutic targets". Drug Discov. Today 11 (1–2): 8–20. doi:10.1016/S1359-6446(05)03637-8. PMID 16478686.
- ↑ Uceyler N, Sommer C (2007). "Cytokine-induced Pain: Basic Science and Clinical Implications". Reviews in Analgesia 9 (2): 87–103. doi:10.3727/000000007783992807.
- ↑ Fredman B, Nun MB, Zohar E, et al. (Feb 1999). "Epidural steroids for treating "failed back surgery syndrome": is fluoroscopy really necessary?". Anesth Analg. 88 (2): 367–72. doi:10.1097/00000539-199902000-00027. PMID 9972758.
- ↑ Landau WM, Nelson DA, Armon C, Argoff CE, Samuels J, Backonja MM (Aug 2007). "Assessment: use of epidural steroid injections to treat radicular lumbosacral pain: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology". Neurology 69 (6): 614; author reply 614–5. doi:10.1212/01.wnl.0000278878.51713.c8. PMID 17679685.
- ↑ Abbasi A, Malhotra G, Malanga G, Elovic EP, Kahn S (Sep 2007). "Complications of interlaminar cervical epidural steroid injections: a review of the literature". Spine 32 (19): 2144–51. doi:10.1097/BRS.0b013e318145a360. PMID 17762818.
- ↑ Bell GK, Kidd D, North RB (May 1997). "Cost-effectiveness analysis of spinal cord stimulation in treatment of failed back surgery syndrome". J Pain Symptom Manage 13 (5): 286–95. doi:10.1016/S0885-3924(96)00323-5. PMID 9185434.
- ↑ Kumar K, Taylor RS, Jacques L, et al. (Nov 2007). "Spinal cord stimulation versus conventional medical management for neuropathic pain: a multicentre randomised controlled trial in patients with failed back surgery syndrome". Pain 132 (1–2): 179–88. doi:10.1016/j.pain.2007.07.028. PMID 17845835.
- ↑ Robaina-Padrón FJ (October 2007). "Controversias de la cirugía instrumentada y el tratamiento del dolor lumbar por enfermedad degenerativa. Resultados de la evidencia científica" [Controversies about instrumented surgery and pain relief in degenerative lumbar spine pain. Results of scientific evidence] (PDF). Neurocirugia (Astur) (in Spanish) 18 (5): 406–13. doi:10.4321/s1130-14732007000500004. PMID 18008014.
- ↑ Stromquist B, et al. (2001). "The Swedish National Register for Lumbar Spine Surgery: Swedish Society for Spinal Surgery". Acta Orhop. Scand 72 (2): 99–106. doi:10.1080/000164701317323327.
- ↑ Cherkin D. C.; et al. (1994). "An international comparison of back surgery rates". Spine 19 (11): 1201–1206. doi:10.1097/00007632-199405310-00001. PMID 8073310.
- ↑ Bunker J. P. (1970). "Surgical manpower. A comparison of operations and surgeons in the United States and in England and Wales". N. Engl. J. Med. 282 (3): 135–144. doi:10.1056/NEJM197001152820306. PMID 5409538.
- ↑ Lewis C. E. (1969). "Variations in the Incidence of Surgery". N. Engl. J. Med. 281 (16): 880–994. doi:10.1056/NEJM196910162811606. PMID 5812257.