Ezetimibe
 | |
| Systematic (IUPAC) name | |
|---|---|
|
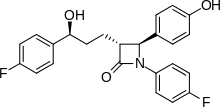
(3R,4S)-1-(4-fluorophenyl)-3-[(3S)-3-(4-fluorophenyl)-3-hydroxypropyl]-4-(4-hydroxyphenyl)azetidin-2-one | |
| Clinical data | |
| Trade names | Zetia |
| AHFS/Drugs.com | monograph |
| MedlinePlus | a603015 |
| Pregnancy category | |
| Legal status | |
| Routes of administration | Oral |
| Pharmacokinetic data | |
| Bioavailability | 35–65% |
| Protein binding | >90% |
| Metabolism | Intestinal wall, hepatic |
| Biological half-life | 19–30 hours |
| Excretion | Renal 11%, faecal 78% |
| Identifiers | |
| CAS Number |
163222-33-1 |
| ATC code | C10AX09 |
| PubChem | CID 150311 |
| IUPHAR/BPS | 6816 |
| DrugBank |
DB00973 |
| ChemSpider |
132493 |
| UNII |
EOR26LQQ24 |
| KEGG |
D01966 |
| ChEBI |
CHEBI:49040 |
| ChEMBL |
CHEMBL1138 |
| Chemical data | |
| Formula | C24H21F2NO3 |
| Molar mass | 409.4 g·mol−1 |
| |
| |
| Physical data | |
| Melting point | 164 to 166 °C (327 to 331 °F) |
| (verify) | |
Ezetimibe /ɛˈzɛtᵻmɪb/ is a drug that lowers plasma cholesterol levels. It acts by decreasing cholesterol absorption in the small intestine. It may be used alone (marketed as Zetia or Ezetrol), when other cholesterol-lowering medications are not tolerated, or together with statins (e.g., ezetimibe/simvastatin, marketed as Vytorin and Inegy) when statins alone do not control cholesterol.
Ezetimibe is recommended as second line therapy for those intolerant of statins or unable to achieve target LDL cholesterol levels on statins alone by several major medical group practice guidelines, but not by those of the American Heart Association and American College of Cardiology.
Medical uses
As of mid-2014, treatment guidelines of the American Heart Association/American College of Cardiology[1] recommend that people with dyslipidemia be treated with a statin. These guidelines recommend increasing the statin dose in certain populations, but do not recognize target serum cholesterol levels or recommend the use of non-statin cholesterol lowering drugs. Guidelines issued by the European Society of Cardiology/European Atherosclerosis Society,[2] the Japan Atherosclerosis Society,[3] the National Institute for Health and Clinical Excellence,[4] and the International Atherosclerosis Society[5] recommend ezetimibe as one of several second line treatment options for people who are intolerant of statins or who are unable to reach serum LDL goals using statins alone.
While ezetimibe reduces LDL cholesterol, it has not been shown to have an impact on outcomes such as risk of death or major cardiovascular event like heart attack or stroke.[6] Its effectiveness in reducing atherosclerosis in clinical trials has been inconsistent.[6] The question of whether ezetimibe could make a difference in major outcomes was examined in the IMPROVE-IT trial, which compared treatment with ezetimibe vs. placebo on top of a background regimen of statin therapy in people who have had recent episodes of acute coronary syndrome over a six-year period.[6] The trial results showing that ezetimibe treatment lowered the risk of experiencing a vascular event by 2%.[7]
Ezetimibe is indicated in the United States as an add-on to dietary measures to:[8]
- reduce levels of certain lipids in people with primary hyperlipidemia, alone or with a statin;
- reduce levels of certain lipids in people with mixed hyperlipidemia, in combination with fenofibrate;
- reduce levels of certain lipids in people with homozygous familial hypercholesterolemia, in combination with specific statins;
- reduce levels of certain lipids in people with homozygous sitosterolemia.
Contraindications
The two contraindications to taking ezetimibe are a previous allergic reaction including rash, angioedema, and anaphylaxis, and severe liver disease, especially when taken with a statin.[9]
Ezetimibe may have significant medication interactions with cyclosporine and with fibrates other than fenofibrate.[8]
Adverse effects
Common adverse drug reactions (≥1% of patients) associated with ezetimibe therapy include: headache and/or diarrhea (steatorrhea). Infrequent adverse effects (0.1–1% of patients) include: myalgia and/or raised liver function test (ALT/AST) results. Rarely (<0.1% of patients), hypersensitivity reactions (rash, angioedema) or myopathy may occur.[8] Cases of muscle problems (myalgia and rhabdomyolysis) have been reported and are included as warnings on the label for ezetimibe.[8]
Mechanism of action
Ezetimibe inhibits the absorption of cholesterol from the small intestine and decreases the amount of cholesterol normally available to liver cells, leading them to absorb more from circulation and thus lowering levels of circulating cholesterol. The exact mechanism is not known, but it appears that ezetimibe blocks the critical mediator of cholesterol absorption, the Niemann-Pick C1-like 1 (NPC1L1) protein on the gastrointestinal tract epithelial cells as well as in hepatocytes; blocks aminopeptidase N, and interrupts a Caveolin 1-Annexin A2 complex involved in trafficking cholesterol.[6]
Pharmacokinetics
Within 4–12 hours of the oral administration of a 10-mg dose to fasting adults, the attained mean ezetimibe peak plasma concentration (Cmax) was 3.4–5.5 ng/ml. Following oral administration, ezetimibe is absorbed and extensively conjugated to a phenolic glucuronide (active metabolite). Mean Cmax (45–71 ng/ml) of ezetimibe-glucuronide is attained within 1–2 h. The concomitant administration of food (high-fat vs. nonfat meals) has no effect on the extent of absorption of ezetimibe. However, coadministration with a high-fat meal increases the Cmax of ezetimibe by 38%. The absolute bioavailability cannot be determined, since ezetimibe is insoluble in aqueous media suitable for injection. Ezetimibe and its active metabolite are highly bound to human plasma proteins (90%).[8]
Ezetimibe is primarily metabolized in the liver and the small intestine via glucuronide conjugation with subsequent renal and biliary excretion. Both the parent compound and its active metabolite are eliminated from plasma with a half-life around 22 hours, allowing for once-daily dosing. Ezetimibe lacks significant inhibitor or inducer effects on cytochrome P-450 isoenzymes, which explains its limited number of drug interactions. No dose adjustment is needed in patients with renal insufficiency or mild hepatic dysfunction (Child-Pugh score 5–6). Due to insufficient data, the manufacturer does not recommend ezetimibe for patients with moderate to severe hepatic impairment (Child-Pugh score 7–15). In patients with mild, moderate, or severe hepatic impairment, the mean AUC values for total ezetimibe are increased about 1.7-fold, 3– to 4-fold, and 5– to 6-fold, respectively, compared to healthy subjects.[8]
See also
References
- ↑ Stone NJ, Robinson JG, Lichtenstein AH, et al. (June 2014). "2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines". Circulation 129 (25 Suppl 2): S1–45. doi:10.1161/01.cir.0000437738.63853.7a. PMID 24222016.
- ↑ Catapano AL, Reiner Z, De Backer G, et al. (July 2011). "ESC/EAS Guidelines for the management of dyslipidaemias The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS)". Atherosclerosis 217 (1): 3–46. doi:10.1016/j.atherosclerosis.2011.06.011. PMID 21882396.
- ↑ Teramoto T, Sasaki J, Ishibashi S, et al. (2013). "Executive summary of the Japan Atherosclerosis Society (JAS) guidelines for the diagnosis and prevention of atherosclerotic cardiovascular diseases in Japan -2012 version". J. Atheroscler. Thromb. 20 (6): 517–23. doi:10.5551/jat.15792. PMID 23665881.
- ↑ "Lipid modification: cardiovascular risk assessment and the modification of blood lipids for the primary and secondary prevention of cardiovascular disease | Guidance and guidelines | NICE".
- ↑ "An International Atherosclerosis Society Position Paper: global recommendations for the management of dyslipidemia--full report". J Clin Lipidol 8 (1): 29–60. 2014. doi:10.1016/j.jacl.2013.12.005. PMID 24528685.
- 1 2 3 4 Phan BA, Dayspring TD, Toth PP (2012). "Ezetimibe therapy: mechanism of action and clinical update". Vasc Health Risk Manag 8: 415–27. doi:10.2147/VHRM.S33664. PMC 3402055. PMID 22910633.
- ↑ Cannon, Christopher P. (June 18, 2015). "Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes". New England Journal of Medicine 372 (25): 2387–2397. doi:10.1056/NEJMoa1410489. PMID 26039521. Retrieved July 28, 2015.
- 1 2 3 4 5 6 Zetia label, Rev 23. Revised: January 2012
- ↑ U.S. National Library of Medicine, National Institutes of Health, U.S. Department of Health and Human Services. Page last updated: 27 October 2014 Medline Plus: Ezetimibe
| ||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||