Equianalgesic
An equianalgesic (or opioid) chart is a conversion chart that lists equivalent doses of analgesics (drugs used to relieve pain). Equianalgesic charts are used for calculation of an equivalent dose (a dose which would offer an equal amount of analgesia) between different analgesics.[1]
Format
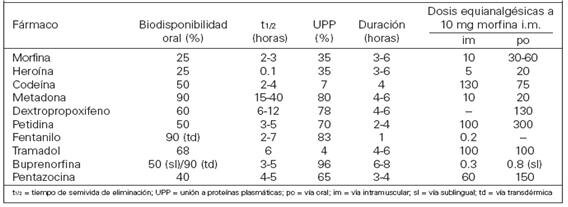
Equianalgesic tables are available in different formats, such as pocket-sized cards for ease of reference.[1] A frequently-seen format has the drug names in the left column, the route of administration in the center columns and any notes in the right column.[2]
Purpose
There are several reasons for switching a patient to a different pain medication. These include practical considerations such as lower cost or unavailability of a drug at the patient's preferred pharmacy, or medical reasons such as lack of effectiveness of the current drug or to minimize adverse effects. Some patients request to be switched to a different narcotic due to stigma associated with a particular drug (e.g. a patient refusing methadone due to its association with opioid addiction treatment).[3] Equianalgesic charts are also used when calculating an equivalent dosage of the same drug, but with a different route of administration.
Precautions
Equianalgesic chart is a useful tool, but the user must take care to correct for all relevant variables such as route of administration, cross tolerance, half-life and the bioavailability of a drug.[4] For example, the narcotic levorphanol is 4–8 times stronger than morphine, but also has a much longer half-life. Simply switching the patient from 40 mg of morphine to 10 mg of levorphanol would be dangerous due to dose accumulation, and hence frequency of administration should also be taken into account.
There are other concerns about equianalgesic charts. Many charts derive their data from studies conducted on opioid-naïve patients. Patients with chronic (rather than acute) pain may respond to analgesia differently. Repeated administration of a medication is also different from single dosing, as many drugs have active metabolites that can build up in the body.[5] Patient variables such as sex, age, and organ function may also influence the effect of the drug on the system. These variables are rarely included in equianalgesic charts.[6]
Opioid-Equivalency Chart
Opioids are a class of compounds that elicit analgesic (pain killing) effects in humans and animals by binding to the μ-opioid receptor within the central nervous system. The following table lists commonly used opioid drugs and their relative potencies. Values for the potencies of opioids listed on this table are given as taken orally unless another route of administration is provided. As such, their bioavailabilities differ, and they may be more potent when taken intravenously. Methadone is different from most opioids considering its potency can vary depending on how long it is taken. Acute use; 1–3 days, yields a potency about 1.5 × stronger than that of morphine and chronic use (7 days+) yields a potency about 2.5 to 5× that of morphine due to methadone being stored in fat tissue, thus giving higher serum levels with longer use. Similarly, the effect of tramadol increases after consecutive dosing due to the accumulation of its active metabolite and an increase of the oral bioavailability in chronic use, this effect becomes less significant again with even longer use as tolerance develops.
| <span style:"font-size:x-large;">Opioid Equivalency Table <span style=font-size:large;">(morphine, PO) | ||||
| Analgesic | Strength (relative) |
Equivalent dose (10 mg Oral morphine) |
Bioavailability | Half-life of active metabolites (hours) |
|---|---|---|---|---|
| Aspirin (non-opioid) | 1⁄360 | 3600 mg | 100% | 3.1–9 |
| Ibuprofen[7] (NSAID, non-opioid) | 1⁄222 | 2220 mg | 87-100% | 1.3-3 |
| Diflunisal (NSAID, non-opioid) | 1⁄160 | 1600 mg | 80–90% | 8–12 |
| Naproxen[7] (NSAID, non-opioid) | 1⁄138 | 1380 mg | 95% | 12-24 |
| Dextropropoxyphene[8] | 1⁄13 to 1⁄20 | 130–200 mg | ||
| Codeine | 1⁄10 | 180 mg (PO) | ≈90% | 2.5–3 (C6G 1.94;[9] morphine 2–3) |
| Tramadol | 1⁄10 | >200 mg | 75% (IR), 85-90% (ER) | 5.5–7 (≈9) |
| Tapentadol | 3⁄10[10] | 32 mg | 32% (fasting) | |
| Tilidine | 1⁄5 | 50 mg | ||
| Dihydrocodeine | 1⁄5 | 50 mg | 20% | 4 |
| Anileridine[11] | 1⁄4 | 40 mg | ||
| Alphaprodine | 1⁄4–1⁄6 | 40–60 mg | ||
| Pethidine (meperidine hydrochloride) | 1⁄3 | 30 mg SC/IM/IV, 300 mg PO | 50–60% | 3–5 |
| Hydrocodone | 1 | 10 mg | ≥80% | 3.8–6 |
| Metopon | 1 | 10 mg | ||
| Pentazocine lactate (IV) [12] | 1 | 10 mg SC/IV/IM, 150 mg PO | ||
| Morphine (oral) | (1) | (10 mg) (30 mg PO) | ≈25% | |
| Oxycodone[13] | 1.5 | 6.67 mg | ≤87% | 3–4.5 |
| Morphine (IV/IM) | 3 | 3.33 mg | 100% | 2–3 |
| Clonitazene | 3 | 3.33 mg | ||
| Methadone (acute) [14][15] | 3–4 | 2.5–3.33 mg | 40–90% | 15–60 |
| Diamorphine (Heroin; IV/IM)[16] | 4–5 | 2–2.5 mg | 100% | <0.6 |
| Hydromorphone[17] | 5 | 1.5 mg SC/IV/IM, 7.5 mg PO | 62% | 2–3 |
| Oxymorphone[18] | 7 | 10 mg PO, 1 mg IV | 10% | 7.25–9.43 |
| Methadone (chronic) [15] | 2.5 to 5 | 3.33 mg | 40–90% | 15–60 |
| Levorphanol[19] | 8 | 1.3 mg | 70% | 11–16 |
| 7-Hydroxymitragynine | 17 | ≈.6 mg | ||
| Buprenorphine[8] | 40 | 0.4 mg | 35–40% (SL) | 20–70, mean 37 |
| Fentanyl | 50–100 | 0.1 mg (100 mcg) IM/IV | 33% (SL); 92% (TD) | 0.04 (IV); 7 (TD) |
| Sufentanil | 500–1,000 | 10–20 μg | 4.4 | |
| Bromadol [notes 1] | 504 | ≈ 20 µg | ||
| Etorphine [notes 1] | 1,000–3,000 | 3.3–10 μg | ||
| Etonitazene[notes 1] | 2,000 | 5.0 µg | ||
| Dihydroetorphine[notes 1] | 1,000–12,000 | 20–40 µg | ||
| Carfentanil [notes 1][19] | 10,000–100,000 | 0.1–1.0 μg | 7.7 | |
| "Strength" is defined as analgesic potency relative to morphine. Tolerance, sensitization, cross-tolerance, metabolism, and hyperalgesia may be complex factors in some individuals. Interactions caused by polypharmacy, food and drink, and other factors, may potentiate or inhibit the effectiveness of certain analgesics as well as drastically alter their halflife. Because some analgesics are prodrugs, individual variation in liver enzymes (e.g., cytochrome P450 enzyme CYP2D6) may result in significantly altered effects. | ||||
See also
- Oripavine – for more on the comparative strength of oripavine derivatives
Notes
References
- 1 2 Joishy, S. K. (1999). Palliative medicine secrets. Philadelphia PA: Hanley & Belfus. p. 97. ISBN 1-56053-304-8.
- ↑ McPherson, Mary Lynn M. (2000). Demystifying Opioid Conversion Calculations: A Guide for Effective Dosing. Bethesda MD: American Society of Health-System Pharmacists. p. 5. ISBN 1-58528-198-0.
- ↑ McPherson 2000, p. 3
- ↑ McPherson 2000, p. 4
- ↑ McPherson 2000, p. 8
- ↑ McPherson 2000, p. 9
- 1 2 http://www3.us.elsevierhealth.com/PAIN/pdf/Chart2a.pdf
- 1 2 "Ch. 4 Narcotics: Synthetic Narcotics: Dextropropoxyphene". Drugs of Abuse. Drug Enforcement Administration, U.S. Department of Justice. 2005.
- ↑ KuKanich B (February 2010). "Pharmacokinetics of acetaminophen, codeine, and the codeine metabolites morphine and codeine-6-glucuronide in healthy Greyhound dogs". J. Vet. Pharmacol. Ther. 33 (1): 15–21. doi:10.1111/j.1365-2885.2009.01098.x. PMC 2867071. PMID 20444020.
- ↑ (PDF) https://www.nhms.org/sites/default/files/Pdfs/Opioid-Comparison-Chart-Prescriber-Letter-2012.pdf. Missing or empty
|title=(help) - ↑ "Anileridine". DrugBank Version: 3.0. DrugBank.
- ↑ "TALWIN (pentazocine lactate) injection, solution". DailyMed. National Institute of Health. Retrieved 2011-12-10.
- ↑ "Equianalgesic Conversion". GlobalRPH.
- ↑ http://www.psicofarmacos.info/images/graficos/Tabla4_opiaceos.JPG
- 1 2 Manfredonia JF (March 2005). "Prescribing methadone for pain management in end-of-life care". J Am Osteopath Assoc 105 (3 Suppl 1): S18–21. PMID 18154194.
|chapter=ignored (help) - ↑ Reichle CW, Smith GM, Gravenstein JS, Macris SG, Beecher HK (April 1962). "Comparative analgesic potency of heroin and morphine in postoperative patients". J. Pharmacol. Exp. Ther. 136 (1): 43–6. PMID 14491157.
- ↑ http://www.palliative.org/PC/ClinicalInfo/PCareTips/MorphineVSHydromorphine.html (Log in required)
- ↑ "Equianalgesic Conversion". Global RPH.
- 1 2 "Levorphanol". DrugBank Version: 3.0. DrugBank.
{kind=link}
http://globalrph.com/narcoticonv.htm
External links
- Equianalgesic Charts
- American Pain Society Guidelines
- Clinical Practice Guideline for the Management of Opioid Therapy for Chronic Pain
- Online opioid equianalgesia calculator Electronic calculator that includes logic for bidirectional and dose-dependent conversions
- Opioid equianalgesic tables: are they all equally dangerous?