Chromosome 15 (human)
| Chromosome 15 (human) | |
|---|---|
 Pair of human chromosome 15 (after G-banding). One is from mother, one is from father. | |
 Chromosome 15 pair in human male karyogram. | |
| Features | |
| Length (bp) | 101,991,189 bp |
| Number of genes | 1,428 |
| Type | Autosome |
| Centromere position | Acrocentric [1] |
| Identifiers | |
| RefSeq | NC_000015 |
| GenBank | CM000677 |
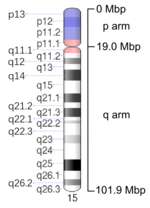
Chromosome 15 is one of the 23 pairs of chromosomes in humans. People normally have two copies of this chromosome. Chromosome 15 spans about 101 million base pairs (the building material of DNA) and represents between 3% and 3.5% of the total DNA in cells.
Identifying genes on each chromosome is an active area of genetic research. Because researchers use different approaches to predict the number of genes on each chromosome, the estimated number of genes varies. Chromosome 15 likely contains between 700 and 900 genes.
Genes
The human leukocyte antigen gene for β2-microglobulin is found at chromosome 15. The following are some of the genes located on chromosome 15:
- CAPN3: Calpain 3 (limb-girdle muscular dystrophy type 2A)
- CHP: Calcium binding protein P22
- FAH: fumarylacetoacetate hydrolase (fumarylacetoacetase)
- FBN1: fibrillin 1 (Marfan syndrome)
- HEXA: hexosaminidase A (alpha polypeptide)(Tay-Sachs disease)
- IVD: isovaleryl Coenzyme A dehydrogenase
- MCPH4: microcephaly, primary autosomal recessive 4
- OCA2: oculocutaneous albinism II (pink-eye dilution homolog, mouse)
- RAD51: RAD51 homolog (RecA homolog, E. coli) (S. cerevisiae)
- STRC: stereocilin
- UBE3A: ubiquitin protein ligase E3A (human papilloma virus E6-associated protein, Angelman syndrome)
- PML: promyelocytic leukemia protein (involved in t(15,17) with RARalpha, predominant cause of acute promyelocytic leukemia.
- SLC24A5: the gene responsible for at least 1/3 of the skin color differences between races, expressed in the brain and the nervous system
- EYCL3 Eye color 3, BROWN - location: 15q11-q15 (note eye colour is a polygenic trait)
- EYCL2 Eye color 2, Determines the positioning of melanocytes on the iris (note eye colour is a polygenic trait)
Chromosomal conditions
The following conditions are caused by mutations in chromosome 15. Two of the conditions (Angelman syndrome and Prader-Willi syndrome) involve a loss of gene activity in the same part of chromosome 15, the 15q11.2-q13.1 region. This discovery provided the first evidence in humans that something beyond genes could determine how the genes are expressed.[2]
Angelman syndrome
The main characteristics of Angelman syndrome are severe mental retardation, ataxia, lack of speech, and excessively happy demeanor. Angelman syndrome results from a loss of gene activity in a specific part of chromosome 15, the 15q11-q13 region. This region contains a gene called UBE3A that, when mutated or absent, likely causes the characteristic features of this condition. People normally have two copies of the UBE3A gene, one from each parent. Both copies of this gene are active in many of the body's tissues. In the brain, however, only the copy inherited from a person's mother (the maternal copy) is active. If the maternal copy is lost because of a chromosomal change or a gene mutation, a person will have no working copies of the UBE3A gene in the brain.
In most cases (about 70%), people with Angelman syndrome have a deletion in the maternal copy of chromosome 15. This chromosomal change deletes the region of chromosome 15 that includes the UBE3A gene. Because the copy of the UBE3A gene inherited from a person's father (the paternal copy) is normally inactive in the brain, a deletion in the maternal chromosome 15 results in no active copies of the UBE3A gene in the brain.
In 3% to 7% of cases, Angelman syndrome occurs when a person has two copies of the paternal chromosome 15 instead of one copy from each parent. This phenomenon is called paternal uniparental disomy (UPD). People with paternal UPD for chromosome 15 have two copies of the UBE3A gene, but they are both inherited from the father and are therefore inactive in the brain.
About 10% of Angelman syndrome cases are caused by a mutation in the UBE3A gene, and another 3% result from a defect in the DNA region that controls the activation of the UBE3A gene and other genes on the maternal copy of chromosome 15. In a small percentage of cases, Angelman syndrome may be caused by a chromosomal rearrangement called a translocation or by a mutation in a gene other than UBE3A. These genetic changes can abnormally inactivate the UBE3A gene.
Angelman syndrome can be hereditary, as evidenced by one case where a patient became pregnant with a daughter who also had the condition.[3]
Prader-Willi syndrome
The main characteristics of this condition include polyphagia (extreme, insatiable appetite), mild to moderate developmental delay, hypogonadism resulting in delayed to no puberty, and hypotonia. Prader-Willi syndrome is caused by the loss of active genes in a specific part of chromosome 15, the 15q11-q13 region. People normally have two copies of this chromosome in each cell, one copy from each parent. Prader-Willi syndrome occurs when the paternal copy is partly or entirely missing.
In about 70% of cases, Prader-Willi syndrome occurs when the 15q11-q13 region of the paternal chromosome 15 is deleted. The genes in this region are normally active on the paternal copy of the chromosome and are inactive on the maternal copy. Therefore, a person with a deletion in the paternal chromosome 15 will have no active genes in this region.
In about 25% of cases, a person with Prader-Willi syndrome has two maternal copies of chromosome 15 in each cell instead of one copy from each parent. This phenomenon is called maternal uniparental disomy. Because some genes are normally active only on the paternal copy of this chromosome, a person with two maternal copies of chromosome 15 will have no active copies of these genes.
In a small percentage of cases, Prader-Willi syndrome is not caused by a chromosomal rearrangement called a trans location. Rarely, the condition is caused by an abnormality in the DNA region that controls the activity of genes on the paternal chromosome 15. Because patients almost always have difficulty reproducing, Prader-Willi syndrome is generally not hereditary.
Isodicentric chromosome 15
A specific chromosomal change called an isodicentric chromosome 15 (previously called an inverted duplication 15) can affect growth and development. The patient possesses an "extra" or "marker" chromosome. This small extra chromosome is made up of genetic material from chromosome 15 that has been abnormally duplicated (copied) and attached end-to-end. In some cases, the extra chromosome is very small and has no effect on a person's health. A larger isodicentric chromosome 15 can result in weak muscle tone (hypotonia), mental retardation, seizures, and behavioral problems. Signs and symptoms of autism (a developmental disorder that affects communication and social interaction) have also been associated with the presence of an isodicentric chromosome 15.
Other chromosomal conditions
Other changes in the number or structure of chromosome 15 can cause mental retardation, delayed growth and development, hypotonia, and characteristic facial features. These changes include an extra copy of part of chromosome 15 in each cell (partial trisomy 15) or a missing segment of the chromosome in each cell (partial monosomy 15). In some cases, several of the chromosome's DNA building blocks (nucleotides) are deleted or duplicated.
The following diseases are some of those related to genes on chromosome 15:
- Bloom syndrome
- Breast cancer
- Isovaleric acidemia
- Loeys-Dietz, type 3 (SMAD3 gene)
- Marfan syndrome
- Nonsyndromic deafness
- Tay-Sachs disease
- Tyrosinemia
References
Specific references:
- ↑ "Table 2.3: Human chromosome groups". Human Molecular Genetics (2nd ed.). Garland Science. 1999.
- ↑ "Teacher's Guide". Ghost in Your Genes (season 35). Nova (TV series). October 16, 2007. Retrieved 2009-09-26.
The program...recounts how one scientist determined how the deletion of a key sequence of DNA on human chromosome 15 could lead to two different syndromes depending on whether the deletion originated from the mother or the father [and] explains that this was the first human evidence that something other than genes themselves could determine how genes are expressed.
- ↑ Lossie A, Driscoll D (1999). "Transmission of Angelman syndrome by an affected mother". Genet Med 1 (6): 262–6. doi:10.1097/00125817-199909000-00004. PMID 11258627.
General references:
- Bittel DC, Butler MG (2005). "Prader-Willi syndrome: clinical genetics, cytogenetics and molecular biology". Expert Rev Mol Med 7 (14): 1–20. doi:10.1017/S1462399405009531. PMID 16038620.
- Bittel DC, Kibiryeva N, Talebizadeh Z, Butler MG (2003). "Microarray analysis of gene/transcript expression in Prader-Willi syndrome: deletion versus UPD". J Med Genet 40 (8): 568–574. doi:10.1136/jmg.40.8.568. PMC 1735542. PMID 12920063.
- Bittel DC, Kibiryeva N, Talebizadeh Z, Driscoll DJ, Butler MG (2005). "Microarray analysis of gene/transcript expression in Angelman syndrome: deletion versus UPD". Genomics 85 (1): 85–91. doi:10.1016/j.ygeno.2004.10.010. PMID 15607424.
- Borgatti R, Piccinelli P, Passoni D, Dalpra L, Miozzo M, Micheli R, Gagliardi C, Balottin U (2001). "Relationship between clinical and genetic features in "inverted duplicated chromosome 15" patients". Pediatr Neurol 24 (2): 111–116. doi:10.1016/S0887-8994(00)00244-7. PMID 11275459.
- Butler MG, Bittel DC, Kibiryeva N, Talebizadeh Z, Thompson T (2004). "Behavioral differences among subjects with Prader-Willi syndrome and type I or type II deletion and maternal disomy". Pediatrics 113 (3 Pt 1): 565–573. doi:10.1542/peds.113.3.565. PMID 14993551.
- Cassidy SB, Dykens E, Williams CA (2000). "Prader-Willi and Angelman syndromes: sister imprinted disorders". Am J Med Genet 97 (2): 136–146. doi:10.1002/1096-8628(200022)97:2<136::AID-AJMG5>3.0.CO;2-V. PMID 11180221.
- Clayton-Smith J, Laan L (2003). "Angelman syndrome: a review of the clinical and genetic aspects". J Med Genet 40 (2): 87–95. doi:10.1136/jmg.40.2.87. PMC 1735357. PMID 12566516.
- Gilbert F (1999). "Disease genes and chromosomes: disease maps of the human genome. Chromosome 15". Genet Test 3 (3): 309–322. doi:10.1089/109065799316653. PMID 10495933.
- Lee S, Wevrick R (2000). "Identification of novel imprinted transcripts in the Prader-Willi syndrome and Angelman syndrome deletion region: further evidence for regional imprinting control". Am J Hum Genet 66 (3): 848–858. doi:10.1086/302817. PMC 1288168. PMID 10712201.
- Rineer S, Finucane B, Simon EW (1998). "Autistic symptoms among children and young adults with isodicentric chromosome 15". Am J Med Genet 81 (5): 428–433. doi:10.1002/(SICI)1096-8628(19980907)81:5<428::AID-AJMG12>3.0.CO;2-E. PMID 9754629.
- Zollino M, Tiziano F, Di Stefano C, Neri G (1999). "Partial duplication of the long arm of chromosome 15: confirmation of a causative role in craniosynostosis and definition of a 15q25-qter trisomy syndrome". Am J Med Genet 87 (5): 391–394. doi:10.1002/(SICI)1096-8628(19991222)87:5<391::AID-AJMG4>3.0.CO;2-O. PMID 10594876.
| Wikimedia Commons has media related to Human chromosome 15. |
| ||||||||||