Central giant-cell granuloma
| Central giant-cell granuloma | |
|---|---|
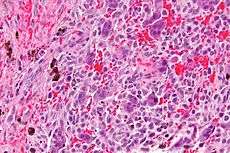 Micrograph of a central giant cell granuloma showing the characteristic giant cells with surrounding cells that have nuclei that are dissimilar to those in the giant cells. H&E stain. | |
| Classification and external resources | |
| Specialty | gastroenterology |
| ICD-10 | K10.1 |
| ICD-9-CM | 526.3 |
Central giant-cell granuloma (CGCG) is a benign condition of the jaws. It is twice as likely to affect women and is more likely to occur in 20- to 40-year-old people. Central giant-cell granulomas are more common in the mandible and often cross the midline.
Overview
CGCG lesions are found more commonly in the anterior of the maxilla and the mandible in younger people (before age 20). They are characterized by large lesions that expand the cortical plate and can resorb roots and move teeth. They are composed of multi-nucleated giant cells. CGCG has a slight predilection for females.
Radiographically it appears as multilocular radiolucencies of bone.
There are two types of CGCG's, non-aggressive and aggressive. The former has a slow rate of growth and thus less likely to resorb roots and perforate the cortical plate. The aggressive form has rapid growth and thus is much more likely to resorb roots and perforate the cortical plate. It also has a high rate for recurrence and can be painful and cause paresthesia.
Differential diagnosis to include: odontogenic keratocyst (OKC), ameloblastoma, odontogenic myxoma, hemangioma, central odontogenic fibroma, hyperparathyroid tumor, and cherubism.
Histology
The histology of CGCG is one that is composed of many multinucleated giant cells. There is evidence that these giant cells represent osteoclasts (bone-eating cells); others suggest they are more like macrophages. The giant cells may be diffusely located throughout the lesion or focally aggregate in the lesion. The giant cells are typically either large and round, or small and irregular, and can vary greatly in size and shape. Close examination may reveal some hemosiderin deposits as well.
Treatment
The treatment for CGCG is thorough curettage. A referral is made to an oral surgeon. Recurrence ranges from 15%–20%. In aggressive tumors, three alternatives to surgery are undergoing investigation:
- corticosteroids;
- calcitonin (salmon calcitonin);
- interferon α-2a.
These therapeutic approaches provide positive possible alternatives for large lesions. The long term prognosis of giant-cell granulomas is good and metastases do not develop.
References
- Kahn, Michael A. Basic Oral and Maxillofacial Pathology. Volume 1. 2001.
- Neville, Brad et al. Oral and Maxillofacial Pathology, second edition. 2002.