Candidiasis
| Candidiasis | |
|---|---|
 Oral candidiasis (thrush) | |
| Classification and external resources | |
| Specialty | Infectious disease |
| ICD-10 | B37 |
| ICD-9-CM | 112 |
| DiseasesDB | 1929 |
| MedlinePlus | 001511 |
| eMedicine | med/264 emerg/76 ped/312 derm/67 |
| Patient UK | Candidiasis |
| MeSH | D002177 |
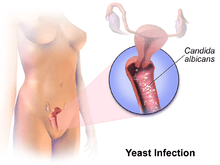
Candidiasis is a fungal infection due to any type of Candida (a type of yeast).[1] When it affects the mouth, it is commonly called thrush.[1] Signs and symptoms include white patches on the tongue or other areas of the mouth and throat.[2] Other symptoms may include soreness and problems swallowing.[2] When it affects the vagina, it is commonly called a yeast infection.[1] Signs and symptoms include genital itching, burning, and sometimes a white "cottage cheese-like" discharge from the vagina.[3] Less commonly the penis may be affected, resulting in itchiness.[2] Very rarely, the infection may become invasive spreading throughout the body, resulting in fevers along with other symptoms depending on the parts of the body affected.[4]
More than 20 types of Candida can cause infection with Candida albicans being the most common.[1] Infections of the mouth are most common among children less than one month old, the elderly, and those with weak immune systems. Conditions that result in a weak immune system include HIV/AIDS, the medications used after organ transplantation, diabetes, and the use of corticosteroids. Other risks include dentures and following antibiotic therapy.[5] Vaginal infections occur more commonly during pregnancy, in those with weak immune systems, and following antibiotic use.[6] Risk for widespread infection includes being in an intensive care unit, following surgery, low birth weight infants, and those with weak immune systems.[7]
Efforts to prevent infections of the mouth include the use of chlorhexidine mouth wash in those with poor immune function and washing out the mouth following the use of inhaled steroids.[8] Little evidence supports probiotics for either prevention or treatment even among those with frequent vaginal infections.[9][10] For infections of the mouth, treatment with topical clotrimazole or nystatin is usually effective. Oral or intravenous fluconazole, itraconazole, or amphotericin B may be used if these do not work.[8] A number of topical antifungal medications may be used for vaginal infections including clotrimazole.[11] In those with widespread disease, a number of weeks of intravenous amphotericin B is often used.[12] In certain groups at very high risk antifungal medications may be used preventatively.[7]
Infections of the mouth occur in about 6% of babies less than a month old. About 20% of those receiving chemotherapy for cancer and 20% of those with AIDS also develop the disease.[13] About three-quarters of women have at least one yeast infection at some time during their lives.[14] Widespread disease is rare except in those who have risk factors.[15] These diseases are also known technically as candidosis, moniliasis, and oidiomycosis.[16]
Signs and symptoms


Signs and symptoms of candidiasis vary depending on the area affected.[17] Most candidal infections result in minimal complications such as redness, itching, and discomfort, though complications may be severe or even fatal if left untreated in certain populations. In immunocompetent persons, candidiasis is usually a very localized infection of the skin or mucosal membranes, including the oral cavity (thrush), the pharynx or esophagus, the gastrointestinal tract, the rectum, anus, perianal/perirectal or ano-rectal area (in men as well as women),[18] the perineum, the urinary bladder, the fingernails or toenails (onychomycosis), and the genitalia (vagina, penis, etc.).[19]
Candidiasis is a very common cause of vaginal irritation, or vaginitis, and can also occur on the male genitals. In immunocompromised patients, Candida infections can affect the esophagus with the potential of becoming systemic, causing a much more serious condition, a fungemia called candidemia.[20][21]
Thrush is commonly seen in infants. It is not considered abnormal in infants unless it lasts longer than a few weeks.[22]
Infection of the vagina or vulva may cause severe itching, burning, soreness, irritation, and a whitish or whitish-gray cottage cheese-like discharge. These symptoms are also present in the more common bacterial vaginosis.[23] In a 2002 study, only 33% of women who were self-treating for a yeast infection actually had a such an infection, while most had either bacterial vaginosis or a mixed-type infection.[24] Symptoms of infection of the male genitalia (balanitis thrush) include red skin around the head of the penis, swelling, irritation, itchiness and soreness of the head of the penis, thick, lumpy discharge under the foreskin, unpleasant odour, difficulty retracting the foreskin (phimosis), and pain when passing urine or during sex.[25]
Perianal candidiasis can cause pruritis ani. The lesion can be erythematous, papular, or ulcerative in appearance, and it is not considered to be a sexually transmissible disease.[26]
Esophageal candidiasis can cause difficulty swallowing, or less commonly painful swallowing.[27]
Abnormal proliferation of the candida in the gut may lead to dysbiosis.[28] While it is not yet clear, this alteration may be the source of symptoms generally described as the irritable bowel syndrome,[29][30] and other gastrointestinal diseases.[31][32]
Causes
Candida yeasts are generally present in healthy humans, frequently part of the human body's normal oral and intestinal flora, and particularly on the skin; however, their growth is normally limited by the human immune system, by competition of other microorganisms, such as bacteria occupying the same locations in the human body.[33] Candida requires moisture for growth, notably on the skin.[34] For example, wearing wet swimwear for long periods of time is believed to be a risk factor.[35] In extreme cases, superficial infections of the skin or mucous membranes may enter into the bloodstream and cause systemic Candida infections.
Diseases that increase the risk of candidiasis include HIV/AIDS, mononucleosis, cancer treatments, steroids, stress, antibiotics, diabetes, and nutrient deficiency. Hormone replacement therapy and infertility treatments may also be predisposing factors.[36] Treatment with antibiotics can lead to eliminating the yeast's natural competitors for resources in the oral and intestinal flora; thereby increasing the severity of the condition.[37] A weakened or undeveloped immune system or metabolic illnesses are significant predisposing factors of candidiasis.[38] Almost 15% of people with weakened immune systems develop a systemic illness caused by Candida species.[39] Diets high in simple carbohydrates have been found to affect rates of oral candidiases.[40]
C. albicans was isolated from the vaginas of 19% of apparently healthy women, i.e., those who experienced few or no symptoms of infection. External use of detergents or douches or internal disturbances (hormonal or physiological) can perturb the normal vaginal flora, consisting of lactic acid bacteria, such as lactobacilli, and result in an overgrowth of Candida cells, causing symptoms of infection, such as local inflammation.[41] Pregnancy and the use of oral contraceptives have been reported as risk factors.[42] Diabetes mellitus and the use of antibiotics are also linked to increased rates of yeast infections.[42]
In penile candidiasis, the causes include sexual intercourse with an infected individual, low immunity, antibiotics, and diabetes. Male genital yeast infections are less common, and incidences of infection are only a fraction of those in women; however, yeast infection on the penis from direct contact via sexual intercourse with an infected partner is not uncommon.[43]
Diagnosis


_PAS_stain.jpg)
Diagnosis of a yeast infection is done either via microscopic examination or culturing. For identification by light microscopy, a scraping or swab of the affected area is placed on a microscope slide. A single drop of 10% potassium hydroxide (KOH) solution is then added to the specimen. The KOH dissolves the skin cells, but leaves the Candida cells intact, permitting visualization of pseudohyphae and budding yeast cells typical of many Candida species.
For the culturing method, a sterile swab is rubbed on the infected skin surface. The swab is then streaked on a culture medium. The culture is incubated at 37 °C for several days, to allow development of yeast or bacterial colonies. The characteristics (such as morphology and colour) of the colonies may allow initial diagnosis of the organism causing disease symptoms.[44]
Classification
Candidiasis may be divided into these types:[16]
- Mucosal candidiasis
- Oral candidiasis (thrush, oropharyngeal candidiasis)
- Pseudomembranous candidiasis
- Erythematous candidiasis
- Hyperplastic candidiasis
- Denture-related stomatitis — Candida organisms are involved in about 90% of cases
- Angular stomatitis — Candida species are responsible for about 20% of cases, mixed infection of C. albicans and Staphylococcus aureus for about 60% of cases.
- Median rhomboid glossitis
- Candidal vulvovaginitis (vaginal yeast infection)[45]
- Candidal balanitis, infection of the glans penis, almost exclusively occurring in uncircumcised males[46]
- Esophageal candidiasis (candidal esophagitis)[27]
- Oral candidiasis (thrush, oropharyngeal candidiasis)
- Cutaneous candidiasis
- Onychomycosis (nail infection) caused by Candida[47]
- Invasive candidiasis
- Systemic candidiasis (one organ system involved)
- Disseminated candidiasis (multiple system involvement, e.g. "hepatosplenic candidiasis", which sometimes follows neutropenia; or "candidemia", a form of septicemia).[48] Ultrasound of liver shows wheel inside wheel sign (a central hypoechoic area (necrosis containing fungi) surrounded by an echogenic zone (inflammatory cells).
- Antibiotic candidiasis (iatrogenic candidiasis)
- Dysbiosis of the gut mycobiota [28]
Prevention
A diet that supports the immune system and is not high in simple carbohydrates contributes to a healthy balance of the oral and intestinal flora.[33][40] While yeast infections are associated with diabetes, the level of blood sugar control may not affect the risk.[49] Wearing cotton underwear may help to reduce the risk of developing skin and vaginal yeast infections, along with not wearing wet clothes for long periods of time.[6][35]
Oral hygiene can help prevent oral candidiasis when people have a weakened immune system.[5] For people undergoing cancer treatment, chlorhexidine mouthwash can prevent or reduce thrush.[5] People who use inhaled corticosteroids can reduce the risk of developing oral candidiasis by rinsing the mouth with water or mouthwash after using the inhaler.[5]
For women who experience recurrent yeast infections, there is limited evidence that oral or intravaginal probiotics help to prevent future infections.[9][50] This includes either as pills or as yogurt.[9]
Treatment
Candidiasis is commonly treated with antimycotics; these antifungal drugs include topical clotrimazole, topical nystatin, fluconazole, and topical ketoconazole.
Localized infection
Mouth and throat candidiasis are treated with antifungal medication. Oral candidiasis usually responds to topical treatments; otherwise, systemic antifungal medication may be needed for oral infections. Candida esophagitis may be treated orally or intravenously; for severe or azole-resistant esophageal candidiasis, treatment with amphotericin B may be necessary.[8]
A one-time dose of fluconazole is 90% effective in treating a vaginal yeast infection.[51] Local treatment may include vaginal suppositories or medicated douches. Other types of yeast infections require different dosing. Gentian violet can be used for thrush in breastfeeding babies. C. albicans can develop resistance to fluconazole, this being more of an issue in those with HIV/AIDS who are often treated with multiple courses of fluconazole for recurrent oral infections.[52]
For vaginal yeast infection in pregnancy, topical imidazole or triazole antifungals are considered the therapy of choice owing to available safety data.[53] Systemic absorption of these topical formulations is minimal, posing little risk of transplacental transfer.[53] In vaginal yeast infection in pregnancy, treatment with topical azole antifungals is recommended for 7 days instead of a shorter duration.[53]
No benefit from probiotics has been found for active infections.[10]
Blood infection
Systemic candidiasis occurs when Candida yeast enters the bloodstream and may spread (becoming disseminated candidiasis) to other organs, including the central nervous system, kidneys, liver, bones, muscles, joints, spleen, or eyes. Treatment typically consists of oral or intravenous antifungal medications.[54] In candidal infections of the blood, intravenous fluconazole or an echinocandin such as caspofungin may be used.[55] Amphotericin B is another option.[55]
Prognosis
Among individuals being treated in intensive care units, the mortality rate is about 30-50% when systemic candidiasis develops.[56]
Epidemiology
Oral candidiasis is the most common fungal infection of the mouth,[57] and it also represents the most common opportunistic oral infection in humans.[58] In the Western Hemisphere, about 75% of females are affected at some time in their lives with a vaginal yeast infection.
Esophageal candidiasis is the most common esophageal infection in persons with AIDS, and accounts for about 50% of all esophageal infections, often coexisting with other esophageal diseases. About two-thirds of people with AIDS and esophageal candidiasis also have oral candidiasis.[27]
Candidal sepsis is rare.[59] Candida is the fourth most common cause of bloodstream infections among hospital patients in the United States.[60]
History
Descriptions of what sounds like oral thrush go back to the time of Hippocrates circa 460 - 370 BCE.[17]
Vulvovaginal candidiasis was first described in 1849 by Wilkinson.[61] In 1875, Haussmann demonstrated the causative organism in both vulvovaginal and oral candidiasis is the same.[61]
With the advent of antibiotics following World War II, the rates of candidiasis increased. The rates then decreased in the 1950s following the development of nystatin.[62]
The colloquial term "thrush" refers to the resemblance of the white flecks present in some forms of candidiasis (e.g. pseudomembranous candidiasis) with the breast of the bird of the same name.[63] The term candidosis is largely used in British English, and candidiasis in American English.[61] Candida is also pronounced differently, in American English, the stress is on the "i", whereas in British English the stress is on the first syllable.
The genus Candida and species C. albicans were described by botanist Christine Marie Berkhout in her doctoral thesis at the University of Utrecht in 1923. Over the years, the classification of the genera and species has evolved. Obsolete names for this genus include Mycotorula and Torulopsis. The species has also been known in the past as Monilia albicans and Oidium albicans. The current classification is nomen conservandum, which means the name is authorized for use by the International Botanical Congress (IBC).[64]
The genus Candida includes about 150 different species; however, only a few are known to cause human infections. C. albicans is the most significant pathogenic species. Other species pathogenic in humans include C. tropicalis, C. glabrata, C. krusei, C. parapsilosis, C. dubliniensis, and C. lusitaniae.
The name Candida was proposed by Berkhout. It is from the Latin word toga candida, referring to the white toga (robe) worn by candidates for the Senate of the ancient Roman republic.[61] The specific epithet albicans also comes from Latin, albicare meaning "to whiten".[61] These names refer to the generally white appearance of Candida species when cultured.
Alternative medicine
What has been described as "a large pseudoscientific cult"[65] has developed around the topic of Candida, with claims up to one in three people are affected by conditions with terms such as systemic candidiasis, "candidiasis hypersensitivity", fungal type dysbiosis, Candida-related complex, the yeast syndrome, yeast allergy, yeast overgrowth, or simply "Candida" or "yeast problem".[66] Some practitioners of alternative medicine have promoted these purported conditions and sold dietary supplements as supposed cures; a number of them have been prosecuted.[67][68]
In 1990, alternative health vendor Nature's Way signed an FTC consent agreement not to misrepresent in advertising any self-diagnostic test concerning yeast conditions or to make any unsubstantiated representation concerning any food or supplement's ability to control yeast conditions, with a fine of $30,000 payable to the National Institutes of Health for research in genuine candidiasis.[68]
References
- 1 2 3 4 "Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- 1 2 3 "Symptoms of Oral Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- ↑ "Symptoms of Genital / Vulvovaginal Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- ↑ "Symptoms of Invasive Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- 1 2 3 4 "Risk & Prevention". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- 1 2 "People at Risk for Genital / Vulvovaginal Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- 1 2 "People at Risk for Invasive Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- 1 2 3 "Treatment & Outcomes of Oral Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- 1 2 3 Jurden L, Buchanan M, Kelsberg G, Safranek S (June 2012). "Clinical inquiries. Can probiotics safely prevent recurrent vaginitis?". The Journal of family practice 61 (6): 357, 368. PMID 22670239.
- 1 2 Abad CL, Safdar N (June 2009). "The role of lactobacillus probiotics in the treatment or prevention of urogenital infections--a systematic review.". Journal of chemotherapy (Florence, Italy) 21 (3): 243–52. doi:10.1179/joc.2009.21.3.243. PMID 19567343.
- ↑ "Treatment & Outcomes of Genital / Vulvovaginal Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- ↑ "Treatment & Outcomes of Invasive Candidiasis". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- ↑ "Oral Candidiasis Statistics". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- ↑ "Genital / vulvovaginal candidiasis (VVC)". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- ↑ "Invasive Candidiasis Statistics". cdc.gov. February 13, 2014. Retrieved 28 December 2014.
- 1 2 James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: clinical Dermatology. Saunders Elsevier. pp. 308–311. ISBN 0-7216-2921-0.
- 1 2 Dolin, [edited by] Gerald L. Mandell, John E. Bennett, Raphael (2010). Mandell, Douglas, and Bennett's principles and practice of infectious diseases (7th ed.). Philadelphia, PA: Churchill Livingstone/Elsevier. pp. Chapter 250. ISBN 978-0-443-06839-3.
- ↑ Corno F.; Caldart M.; Toppino M.; Tapparo A.; Capozzi MP.; Goitre M.; Forte M.; Forcheri V.; Cervetti O (1989-11-15). "[Ano-rectal candidiasis.] [La candidosi ano-rettale.]". PubMed/MEDLINE (in English [Original Article in Italian]). National Library of Medicine: Minerva Chirurgica. p. 1. Archived from the original on Nov 15, 1989. Retrieved 30 January 2015.
- ↑ Walsh TJ, Dixon DM (1996). "Deep Mycoses". In Baron S eds.; et al. Baron's Medical Microbiology (4th ed.). Univ of Texas Medical Branch. ISBN 0-9631172-1-1.
- ↑ Fidel PL (2002). "Immunity to Candida". Oral Dis. 8: 69–75. doi:10.1034/j.1601-0825.2002.00015.x. PMID 12164664.
- ↑ Pappas PG (2006). "Invasive candidiasis". Infect. Dis. Clin. North Am. 20 (3): 485–506. doi:10.1016/j.idc.2006.07.004. PMID 16984866.
- ↑ "Thrush". 2011. Retrieved 2011-04-08.
- ↑ Terri Warren, RN (2010). "Is It a Yeast Infection?". Retrieved 2011-02-23.
- ↑ Ferris DG, Nyirjesy P, Sobel JD, Soper D, Pavletic A, Litaker MS (March 2002). "Over-the-counter antifungal drug misuse associated with patient-diagnosed vulvovaginal candidiasis". Obstetrics and Gynecology 99 (3): 419–425. doi:10.1016/S0029-7844(01)01759-8. PMID 11864668.
- ↑ NHS: Symptoms of thrush in men (balanitis thrush)
- ↑ Bruce G. Wolff et al., eds. (2007). The ASCRS textbook of colon and rectal surgery. New York: Springer. pp. 241, 242, 245. ISBN 0-387-24846-3.
- 1 2 3 Yamada T, Alpers DH; et al. (2009). Textbook of gastroenterology (5th ed.). Chichester, West Sussex: Blackwell Pub. p. 814. ISBN 978-1-4051-6911-0.
- 1 2 Mukherjee, PK; Sendid, B; Hoarau, G; Colombel, JF; Poulain, D; Ghannoum, MA (February 2015). "Mycobiota in gastrointestinal diseases.". Nature reviews. Gastroenterology & hepatology 12 (2): 77–87. doi:10.1038/nrgastro.2014.188. PMID 25385227.
- ↑ Santelmann, H; Howard, JM (January 2005). "Yeast metabolic products, yeast antigens and yeasts as possible triggers for irritable bowel syndrome.". European journal of gastroenterology & hepatology 17 (1): 21–6. doi:10.1097/00042737-200501000-00005. PMID 15647635.
- ↑ Collins, SM (August 2014). "A role for the gut microbiota in IBS.". Nature reviews. Gastroenterology & hepatology 11 (8): 497–505. doi:10.1038/nrgastro.2014.40. PMID 24751910.
- ↑ Wang, ZK; Yang, YS; Stefka, AT; Sun, G; Peng, LH (April 2014). "Review article: fungal microbiota and digestive diseases.". Alimentary pharmacology & therapeutics 39 (8): 751–66. doi:10.1111/apt.12665. PMID 24612332.
- ↑ Gouba; Drancourt (2015). "Digestive tract mycobiota: a source of infection.". Médecine et Maladies Infectieuses 45: 9–16. doi:10.1016/j.medmal.2015.01.007. PMID 25684583.
- 1 2 Mulley, A. G.; Goroll, A. H. (2006). Primary Care Medicine: office evaluation and management of the adult patient. Philadelphia: Wolters Kluwer Health. pp. 802–3. ISBN 0-7817-7456-X. Retrieved 2008-11-23.
- ↑ Goehring, Richard V. (2008). Mims' medical microbiology. (4th ed.). Philadelphia, PA: Mosby Elsevier. p. 656. ISBN 978-0-323-04475-2.
- 1 2 MedlinePlus Encyclopedia Vaginal yeast infection
- ↑ Nwokolo NC, Boag FC (May 2000). "Chronic vaginal candidiasis. Management in the postmenopausal patient". Drugs Aging 16 (5): 335–9. doi:10.2165/00002512-200016050-00003. PMID 10917071.
- ↑ Bassetti M, Mikulska M, Viscoli C (December 2010). "Bench-to-bedside review: therapeutic management of invasive candidiasis in the intensive care unit.". Critical Care 14 (6): 244. doi:10.1186/cc9239. PMID 21144007.
- ↑ Odds FC (1987). "Candida infections: an overview". Crit. Rev. Microbiol. 15 (1): 1–5. doi:10.3109/10408418709104444. PMID 3319417.
- ↑ Choo ZW, Chakravarthi S, Wong SF, Nagaraja HS, Thanikachalam PM, Mak JW, Radhakrishnan A, Tay A (2010). "A comparative histopathological study of systemic candidiasis in association with experimentally induced breast cancer". Oncology Letters 1 (1): 215–222. doi:10.3892/ol_00000039. ISSN 1792-1082. PMC 3436220. PMID 22966285.
- 1 2 Akpan A, Morgan R (August 2002). "Oral candidiasis". Postgraduate Medical Journal 78 (922): 455–9. doi:10.1136/pmj.78.922.455. PMC 1742467. PMID 12185216.
- ↑ Mårdh PA, Novikova N, Stukalova E (October 2003). "Colonisation of extragenital sites by Candida in women with recurrent vulvovaginal candidosis". BJOG 110 (10): 934–7. doi:10.1111/j.1471-0528.2003.01445.x. PMID 14550364.
- 1 2 Schiefer HG (1997). "Mycoses of the urogenital tract". Mycoses 40 (Suppl 2): 33–6. doi:10.1111/j.1439-0507.1997.tb00561.x. PMID 9476502.
- ↑ David LM, Walzman M, Rajamanoharan S (October 1997). "Genital colonisation and infection with candida in heterosexual and homosexual males". Genitourin Med 73 (5): 394–6. doi:10.1136/sti.73.5.394. PMC 1195901. PMID 9534752.
- ↑ Srikumar Chakravarthi, Nagaraja HS (2010). "A comprehensive review of the occurrence and management of systemic candidiasis as an opportunistic infection". Microbiology Journal 1 (2): 1–5. ISSN 2153-0696.
- ↑ Mastromarino, Paola; Vitali, Beatrice; Mosca, Luciana (2013). "Bacterial vaginosis: a review on clinical trials with probiotics" (PDF). New Microbiologica 36: 229–238. PMID 23912864.
- ↑ Nyirjesy P, Sobel JD (May 2013). "Genital mycotic infections in patients with diabetes.". Postgraduate Medicine 125 (3): 33–46. doi:10.3810/pgm.2013.05.2650. PMID 23748505.
- ↑ Nolting S, Brautigam M, Weidinger G (1994). "Terbinafine in onychomycosis with involvement by non-dermatophytic fungi". The British journal of dermatology. 130 Suppl 43: 16–21. doi:10.1111/j.1365-2133.1994.tb06088.x. PMID 8186136.
- ↑ Errol Reiss, H. Jean Shadomy, G. Marshall Lyon (2011). "Chapter 11". Fundamental medical mycology. Hoboken, N.J.: John Wiley & Sons. ISBN 978-1-118-10176-6.
- ↑ Mobley, David P. Cappelli, Connie C. (2008). Prevention in clinical oral health care. St. Louis, Mo.: Mosby Elsevier. p. 254. ISBN 9780323036955.
- ↑ Falagas, ME; Betsi, GI; Athanasiou, S (August 2006). "Probiotics for prevention of recurrent vulvovaginal candidiasis: a review.". The Journal of antimicrobial chemotherapy 58 (2): 266–72. doi:10.1093/jac/dkl246. PMID 16790461.
Thus, the available evidence for the use of probiotics for prevention of recurrent VVC is limited
- ↑ Moosa MY, Sobel JD, Elhalis H, Du W, Akins RA (2004). "Fungicidal Activity of Fluconazole against Candida albicans in a Synthetic Vagina-Simulative Medium". Antimicrob. Agents Chemother. 48 (1): 161–7. doi:10.1128/AAC.48.1.161-167.2004. PMC 310176. PMID 14693534.
- ↑ Morschhäuser J (Jul 18, 2002). "The genetic basis of fluconazole resistance development in Candida albicans.". Biochimica et Biophysica Acta 1587 (2-3): 240–8. doi:10.1016/s0925-4439(02)00087-x. PMID 12084466.
- 1 2 3 Soong D, Einarson A (Mar 2009). "Vaginal yeast infections during pregnancy.". Canadian family physician Medecin de famille canadien 55 (3): 255–6. PMC 2654841. PMID 19282531.
- ↑ "Systemic candidiasis". NIH.gov. U.S. DHHS, National Institute of Health. Oct 2014. Retrieved April 19, 2015.
- 1 2 Pappas PG, Kauffman CA, Andes D, Benjamin DK, Calandra TF, Edwards JE, Filler SG, Fisher JF, Kullberg BJ, Ostrosky-Zeichner L, Reboli AC, Rex JH, Walsh TJ, Sobel JD (Mar 1, 2009). "Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America.". Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 48 (5): 503–35. doi:10.1086/596757. PMID 19191635.
- ↑ Williams D, Lewis M (Jan 28, 2011). "Pathogenesis and treatment of oral candidosis.". Journal of oral microbiology 3. doi:10.3402/jom.v3i0.5771. PMC 3087208. PMID 21547018.
- ↑ Bouquot, Brad W. Neville , Douglas D. Damm, Carl M. Allen, Jerry E. (2002). Oral & maxillofacial pathology (2. ed.). Philadelphia: W.B. Saunders. pp. 189–197. ISBN 0-7216-9003-3.
- ↑ Lalla RV, Patton LL, Dongari-Bagtzoglou A (April 2013). "Oral candidiasis: pathogenesis, clinical presentation, diagnosis and treatment strategies.". Journal of the California Dental Association 41 (4): 263–8. PMID 23705242.
- ↑ Gow, Neil (8 May 2002). "Candida albicans - a fungal Dr Jekyll and Mr Hyde". Mycologist 16 (01). doi:10.1017/S0269915X02006183.
- ↑ "Candida" (PDF). CDC.gov. Center of Disease Contrl. Retrieved April 19, 2015.
- 1 2 3 4 5 Lynch DP (August 1994). "Oral candidiasis. History, classification, and clinical presentation.". Oral surgery, oral medicine, and oral pathology 78 (2): 189–93. doi:10.1016/0030-4220(94)90146-5. PMID 7936588.
- ↑ Obladen M (2012). "Thrush - nightmare of the foundling hospitals.". Neonatology 101 (3): 159–65. doi:10.1159/000329879. PMID 22024688.
- ↑ Scully, Crispian. "Mucosal Candidiasis (Medscape)". WebMD LLC. Retrieved 8 September 2013.
- ↑ International Code of Botanical Nomenclature. Königstein. 2000. ISBN 3-904144-22-7. Retrieved 2008-11-23.
- ↑ Odds, FC (1987). "Candida infections: an overview.". Critical reviews in microbiology 15 (1): 1–5. doi:10.3109/10408418709104444. PMID 3319417.
- ↑ Stephen Barrett, M.D. (October 8, 2005). "Dubious "Yeast Allergies"".
- ↑ Barrett S (2005-10-08). "Dubious "Yeast Allergies"". QuackWatch. Retrieved 2008-02-21.
- 1 2 Jarvis WT. "Candidiasis Hypersensitivity". National Council Against Health Fraud. Retrieved January 2014.
External links
| Wikimedia Commons has media related to Candidiasis. |
- Candidiasis at DMOZ
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|