Pap test
| Pap test | |
|---|---|
| Intervention | |
 | |
| ICD-9-CM | 795.00 |
| MeSH | D014626 |
| MedlinePlus | 003911 |
The Papanicolaou test (abbreviated as Pap test, known earlier as Pap smear, cervical smear, or smear test) is a method of cervical screening used to detect potentially pre-cancerous and cancerous processes in the cervix (opening of the uterus or womb). Abnormal findings are often followed up by more sensitive diagnostic procedures, and, if warranted, interventions that aim to prevent progression to cervical cancer. The test was invented by and named after the prominent Greek doctor Georgios Papanikolaou.
A Pap smear is performed by opening the vaginal canal with a speculum, then collecting cells at the outer opening of the cervix at the transformation zone (where the outer squamous cervical cells meet the inner glandular endocervical cells). The collected cells are examined under a microscope to look for abnormalities. The test aims to detect potentially pre-cancerous changes (called cervical intraepithelial neoplasia (CIN) or cervical dysplasia; the squamous intraepithelial lesion system (SIL) is also used to describe abnormalities), which are caused human papillomaviruses, a sexually transmitted a DNA virus. The test remains an effective, widely used method for early detection of pre-cancer and cervical cancer. While the test may also detect infections and abnormalities in the endocervix and endometrium, it is not designed to do so.
In the United States, Pap smear screening is recommended starting around 21 years of age until the age of 65.[1] Guidelines on frequency vary from every three to five years.[1][2][3] If results are abnormal, and depending on the nature of the abnormality, the test may need to be repeated in six to twelve months.[4] If the abnormality requires closer scrutiny, the person may be referred for detailed inspection of the cervix by colposcopy. The person may also be referred for HPV DNA testing, which can serve as an adjunct to Pap testing. Additional biomarkers which may be applied as ancillary tests with the Pap test are evolving.[5]
Medical uses
| Summary of reasons for testing | ||
|---|---|---|
| person's characteristic | indication | rationale |
| never had sexual contact | no test | HPV usually transmitted by sexual contact[6] |
| under age 21, regardless of sexual history | no test | more harms than benefits[7][8] |
| age 20–25 until age 50–60 | test every 3–5 years if results normal | broad recommendation[6][9] |
| over age 65; history of normal tests | no further testing | recommendation of USPSTF, ACOG, ACS and ASCP;[2][6][10][11] |
| had total hysterectomy for non-cancer disease – cervix removed | no further testing | harms of screening after hysterectomy outweigh the benefits[7][8] |
| had partial hysterectomy – cervix remains | continue testing as normal | |
| has received HPV vaccine | continue testing as normal | vaccine does not cover all cancer-causing types of HPV[9] |
| history of endometrial cancer | discontinue routine testing[12] | test no longer effective and likely to give false positive[12] |
Screening guidelines vary from country to country. In general, screening starts about the age of 20 or 25 and continues until about the age of 50 or 60.[10] Screening is typically recommended every three to five years, as long as results are normal.[6][9]
Women should wait a few years after they first have intercourse before they start screening, and should not be screened before age 21. American Congress of Obstetricians and Gynecologists (ACOG) and others recommend starting screening at age 21 (since that is a few years after initial sex for most American women).[2][13] Many other countries wait until age 25 or later to start screening. For instance, some parts of Great Britain start screening at age 25. ACOG's general recommendation is that people with uteruses age 30-65 have an annual well-woman examination, that they not get annual Pap tests, and that they do get Pap tests at three-year intervals.[14]
Most people who contract HPV do so soon after becoming sexually active.[3] It takes an average of a year, but can take up to four years, for a person's immune system to control the initial infection. Screening during this period may show this immune reaction and repair as mild abnormalities, which are usually not associated with cervical cancer, but could cause the person stress and result in further tests and possible treatment. Cervical cancer usually takes time to develop, so delaying the start of screening a few years poses little risk of missing a potentially precancerous lesion. For instance, screening people under age 25 does not decrease cancer rates under age 30.[15]
There is little or no benefit to screening people who have not had sexual contact. For example, United States Preventive Services Task Force (USPSTF) recommends waiting at least three years after first sex.[6] HPV can be transmitted in sex between females, so those who have only had sex with other females should be screened, although they are at somewhat lower risk for cervical cancer.[16]
Guidelines on frequency of screening vary—typically every three to five years for those who have not had previous abnormal smears.[6][9] Some older recommendations suggested screening as frequently as every one to two years, however there is little evidence to support such frequent screening; annual screening has little benefit but leads to greatly increased cost and many unnecessary procedures and treatments.[2] It has been acknowledged since before 1980 that most people can be screened less often.[17] In some guidelines, frequency depends on age; for instance in Great Britain, screening is recommended every 3 years for women under 50, and every 5 years for those over.
Screening should stop about age 65 unless there is a recent abnormal tests or disease. There is probably no benefit screening people aged 60 or over whose previous tests have been negative.[11] If a person's last three Pap results were normal, she can stop at age 65, according to the USPSTF, ACOG, ACS and ASCP;[2][6] England's NHS says 64. There is no need to continue screening after a complete hysterectomy for benign disease.
Pap smear screening is still recommended for those who have been vaccinated against HPV,[9] since the vaccines do not cover all of the HPV types that can cause cervical cancer. Also, the vaccine does not protect against HPV exposure before vaccination.
Those with a history of endometrial cancer should discontinue routine Pap tests.[12] Further tests are unlikely to detect recurrence of cancer but do bring the risk of giving false positive results, which would lead to unnecessary further testing.[12]
More frequent Pap smears may be needed to follow-up after an abnormal Pap smear, or after treatment for abnormal Pap or biopsy results, or after treatment for cancer.
Effectiveness
The Pap test, when combined with a regular program of screening and appropriate follow-up, can reduce cervical cancer deaths by up to 80%.[9]
Failure of prevention of cancer by the Pap test can occur for many reasons, including not getting regular screening, lack of appropriate follow up of abnormal results, and sampling and interpretation errors.[18] In the US, over half of all invasive cancers occur in females that have never had a Pap smear; an additional 10 to 20% of cancers occur in those that have not had a Pap smear in the preceding five years. About one-quarter of US cervical cancers were in people that had an abnormal Pap smear, but did not get appropriate follow-up (person did not return for care, or clinician did not perform recommended tests or treatment).
Adenocarcinoma of the cervix has not been shown to be prevented by Pap tests.[18] In the UK, which has a Pap smear screening program, Adenocarcinoma accounts for about 15% of all cervical cancers[19]
Estimates of the effectiveness of the United Kingdom's call and recall system vary widely, but it may prevent about 700 deaths per year in the UK. A medical practitioner performing 200 tests each year would prevent a death once in 38 years, while seeing 152 people with abnormal results, referring 79 for investigation, obtaining 53 abnormal biopsy results, and seeing 17 persisting abnormalities lasting longer than two years. At least one person during the 38 years would die from cervical cancer despite being screened.[20]
Since the population of the UK is about 61 million, the maximum number of people who could be receiving Pap smears in the UK is around 15 million to 20 million (eliminating the percentage of the population under 20 and over 65). This would indicate that the use of Pap smear screening in the UK saves the life of 1 person for every approximately 20,000 people tested (assuming 15,000,000 are being tested yearly). If only 10,000,000 are actually tested each year, then it would save the life of 1 person for every approximately 15,000 people tested.
Results
In screening a general or low-risk population, most Pap results are normal.
In the United States, about 2–3 million abnormal Pap smear results are found each year.[21] Most abnormal results are mildly abnormal (ASC-US (typically 2–5% of Pap results) or low-grade squamous intraepithelial lesion (LSIL) (about 2% of results)), indicating HPV infection. Although most low-grade cervical dysplasias spontaneously regress without ever leading to cervical cancer, dysplasia can serve as an indication that increased vigilance is needed.
In a typical scenario, about 0.5% of Pap results are high-grade SIL (HSIL), and less than 0.5% of results indicate cancer; 0.2 to 0.8% of results indicate Atypical Glandular Cells of Undetermined Significance (AGC-NOS).
As liquid based preparations (LBPs) become a common medium for testing, atypical result rates have increased. The median rate for all preparations with low-grade squamous intraepithelial lesions using LBPs was 2.9% compared with a 2003 median rate of 2.1%. Rates for high-grade squamous intraepithelial lesions (median, 0.5%) and atypical squamous cells have changed little.[22]
Abnormal results are reported according to the Bethesda system.[23] They include:
- Squamous cell abnormalities (SIL)
- Atypical squamous cells of undetermined significance (ASC-US)
- Atypical squamous cells – cannot exclude HSIL (ASC-H)
- Low-grade squamous intraepithelial lesion (LGSIL or LSIL)
- High-grade squamous intraepithelial lesion (HGSIL or HSIL)
- Squamous cell carcinoma
- Glandular epithelial cell abnormalities
- Atypical Glandular Cells not otherwise specified (AGC or AGC-NOS)
Endocervical and endometrial abnormalities can also be detected, as can a number of infectious processes, including yeast, herpes simplex virus and trichomoniasis. However it is not very sensitive at detecting these infections, so absence of detection on a Pap does not mean absence of the infection.
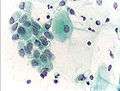
-

Micrograph of a Pap test showing a low-grade intraepithelial lesion (LSIL) and benign endocervical mucosa. Pap stain.
-

Micrograph of a Pap test showing trichomoniasis. Trichomonas organism seen in the upper right. Pap stain.
-

Micrograph of a Pap test showing changes of herpes simplex virus. Pap stain.
-

Endocervical adenocarcinoma on a pap test.
-

Candida organisms on a pap test.
-
Viral cytopathic effect consistent with herpes simplex virus on a pap test.
-

Normal squamous epithelial cells in premenopausal women
-

Atrophic squamous cells in postmenopausal women
-
Normal endocervical cells should be present into the slide, as a proof of a good quality sampling
-

the cytoplasms of squamous epithelial cells melted out; many Döderlein bacilli can be seen
-

Infestation by Trichomonas vaginalis
-

An obviously atypical cell can be seen
Pregnancy
Pap tests can usually be performed during pregnancy up to at least 24 weeks of gestational age.[24] Pap tests during pregnancy have not been associated with increased risk of miscarriage. [24] An inflammatory component is commonly seen on Pap smears from pregnant people,[25] and does not appear to be a risk for subsequent preterm birth.[26]
After childbirth, it is recommended to wait 12 weeks before taking a pap test because inflammation of the cervix caused by the birth interferes with test interpretation.[27]
Procedure

For best results, a Pap test should not occur when a person is menstruating, partly because the additional cells can obscure cervical cells, and partly because this part of the menstrual cycle is when the female organs are most inflamed/LINK/. However, Pap smears can be performed during a person's menstrual period, especially if the physician is using a liquid-based test; if bleeding is extremely heavy, endometrial cells can obscure cervical cells, and it is therefore inadvisable to have a Pap smear if bleeding is excessive.
Obtaining a pap smear should not cause much pain,[28] but it can if the person has certain untreated vaginal problems such as cervical stenosis or vaginismus, or if the person performing it is too harsh, or uses the wrong size speculum.
Yet it's not comfortable, for two reasons which work together: the cervix is full of nociceptors,[29] and the brush used to collect cells has to be stiff enough to scrape them off of the surrounding tissue. So it can be uncomfortable, but it's generally quick, and the information obtained may be critical.
People with underlying pain or tissue diseases that can react to nociceptors (pain nerves) being scraped or to excessive cold in the mucous membranes should take appropriate precautions and discuss the process ahead of time with their providers, in writing if necessary. A smaller speculum, lidocaine gel, and warming the instruments and lubricant ahead of time, along with extra time in the exam room and gentle technique, can all contribute to reducing the risk to manageable levels. These are reasonable accommodations to ask for and are aligned with good practice.
Many people experience spotting or mild diarrhea afterward. The spotting is usually from the scrape on the cervix and the diarrhea may be due to indirect stimulation of the lower intestine during the exam.
Many health care providers are under the false impression that only sterile water, or no lubricant at all, should be used to lubricate the speculum. This may result in unnecessary discomfort. A number of studies have shown that using a small amount of water-based gel lubricant does not interfere with, obscure, or distort the PAP smear. Further, cytology is not affected nor some STD testing.[30]
The health care worker begins by inserting a speculum into the woman's vagina, which spreads the vagina open and allows access to the cervix. The health care provider then collects a sample of cells from the outer opening or os of the cervix by scraping it with an Aylesbury spatula. An endocervical brush is rotated in the central opening of the cervix. The cells are placed on a glass slide and taken to the laboratory to be checked for abnormalities.
A plastic-fronded broom is sometimes used in place of the spatula and brush. The broom is not as good a collection device, since it is much less effective at collecting endocervical material than the spatula and brush.[31] The broom is used more frequently with the advent of liquid-based cytology, although either type of collection device may be used with either type of cytology.
The sample is stained using the Papanicolaou technique, in which tinctorial dyes and acids are selectively retained by cells. Unstained cells cannot be seen with a light microscope. Papanicolaou chose stains that highlighted cytoplasmic keratinization, which actually has almost nothing to do with the nuclear features used to make diagnoses now.
In some cases, a computer system may prescreen the slides, indicating those that do not need examination by a person or highlighting areas for special attention. The sample is then usually screened by a specially trained and qualified cytotechnologist using a light microscope. The terminology for who screens the sample varies according to the country; in the UK, the personnel are known as cytoscreeners, biomedical scientists (BMS), advanced practitioners and pathologists. The latter two take responsibility for reporting the abnormal sample which may require further investigation.
Automated analysis
In the last decade, there have been successful attempts to develop automated, computer image analysis systems for screening.[32] Although, on the available evidence automated cervical screening could not be recommended for implementation into a national screening program, a recent NHS Health technology appraisal concluded that the 'general case for automated image analysis ha(d) probably been made'.[33] Automation may improve sensitivity and reduce unsatisfactory specimens.[34] Two systems have been approved by the FDA and function in high-volume reference laboratories, with human oversight.
Types of screening
- Conventional Pap—In a conventional Pap smear, samples are smeared directly onto a microscope slide after collection.
- Liquid based cytology—The sample of (epithelial) cells is taken from the Transitional Zone; the squamo-columnar junction of the cervix, between the ecto and endocervix. Liquid-based cytology uses an arrow-shaped brush, rather than the conventional spatula. The cells taken are suspended in a bottle of preservative for transport to the laboratory, where using Pap stains it is analysed.
Pap Tests commonly look for epithelial abnormalities/ metaplasia/ dysplasia/ borderline changes, all of which may be indicative of CIN. Nuclei will stain dark blue, squamous cells will stain green and keratinised cells will stain pink/ orange. Koilocytes may be observed where there is some dyskaryosis (of epithelium). The nucleus in koilocytes is typically irregular, indicating possible cause for concern; requiring further confirmatory screens and tests.
In addition, Human Papilloma Virus (HPV) test may be performed either as indicated for abnormal Pap results, or in some cases dual testing is done, where both a Pap smear and HPV test are done at the same time (also called Pap co-testing).
Practical aspects
The endocervix may be partially sampled with the device used to obtain the ectocervical sample, but, due to the anatomy of this area, consistent and reliable sampling cannot be guaranteed. As abnormal endocervical cells may be sampled, those examining them are taught to recognize them.
The endometrium is not directly sampled with the device used to sample the ectocervix. Cells may exfoliate onto the cervix and be collected from there, so as with endocervical cells, abnormal cells can be recognised if present but the Pap Test should not be used as a screening tool for endometrial malignancy.
In the United States, a pap test itself costs $20 to $30, but the costs for pap test visits can cost over $1,000, largely because additional tests are added that may or may not be necessary.[35]
History
The test was invented by and named after the prominent Greek doctor Georgios Papanikolaou who started his research in 1923. Aurel Babeş of Romania independently made similar discoveries in 1927.[36] However, it should be noted that Babeş method was radically different from Papanicolaou's.[37]
Papanicolaou's name was repeatedly submitted to the Nobel Committee and rejected every time. The Nobel Committee delegated the in-depth investigation of Papanicolaou's merits and demerits to the late Professor Santesson, who was at that time the head of pathology at the Stockholm Cancer Institute (the Radiumhemmet). The investigator discovered Babeş' contributions that had never been cited by Papanicolaou and duly reported this fact to the Committee, which then rejected Papanicolaou's Nobel award.[38]
Experimental techniques
In the developed world, cervical biopsy guided by colposcopy is considered the "gold standard" for diagnosing cervical abnormalities after an abnormal pap smear. The procedure requires a trained colposcopist and can be expensive to perform. However, Pap smears are very sensitive and some negative biopsy results may represent undersampling of the lesion in the biopsy, so negative biopsy with positive cytology requires careful follow up.[39]
Experimental visualization techniques use broad-band light (e.g., direct visualization, speculoscopy, cervicography, visual inspection with acetic acid or with Lugol's, and colposcopy) and electronic detection methods (e.g., Polarprobe and in-vivo Spectroscopy). These techniques are less expensive and can be performed with significantly less training. They do not perform as well as Pap smear screening and colposcopy. At this point, these techniques have not been validated by large-scale trials and are not in general use.
Access
In Taiwan most middle and upper-class people have access to the Pap test and can choose to have one done annually. On the other hand, poor people, like those in the southern US study, may not always have access to the Pap test.[40][41][42]
Coccoid bacteria
The finding of coccoid bacteria on a pap test is of no consequence with otherwise normal test findings and no infectious symptoms. However, if there is enough inflammation to obscure the detection of pre-cancerous and cancerous processes, it may indicate treatment with a broad-spectrum antibiotic for streptococci and anaerobic bacteria (such as metronidazole and amoxicillin) before repeating the smear. Alternatively, the test will be repeated at an earlier time than it would otherwise.[43] If there are symptoms of vaginal discharge, bad odor or irritation, the presence of coccoid bacteria also may indicate treatment with antibiotics as per above.[43]
References
- Notes
- 1 2 Moyer, VA; U.S. Preventive Services Task, Force (Jun 19, 2012). "Screening for cervical cancer: U.S. Preventive Services Task Force recommendation statement.". Annals of Internal Medicine 156 (12): 880–91, W312. doi:10.7326/0003-4819-156-12-201206190-00424. PMID 22711081.
- 1 2 3 4 5 Saslow, D; et al. (2012). "American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology Screening Guidelines for the Prevention and Early Detection of Cervical Cancer" (PDF). Journal of Lower Genital Tract Disease 16 (3).
- 1 2 American Cancer Society. (2010). Detailed Guide: Cervical Cancer. Can cervical cancer be prevented? Retrieved August 8, 2011.
- ↑ The American College of Obstetricians and Gynecologists (2009). "ACOG Education Pamphlet AP085 – The Pap Test". Washington, DC. Retrieved June 5, 2010.
- ↑ Shidham VB, Mehrotra R, Varsegi G, D'Amore KL, Hunt B, Narayan R. p16 INK4a immunocytochemistry on cell blocks as an adjunct to cervical cytology: Potential reflex testing on specially prepared cell blocks from residual liquid-based cytology specimens. CytoJournal [serial online] 2011 [cited 2011 Apr 17];8:1. Available from: http://www.cytojournal.com/text.asp?2011/8/1/1/76379
- 1 2 3 4 5 6 7 U.S. Preventive Services Task Force (2003). "Screening for Cervical Cancer: Recommendations and Rationale. AHRQ Publication No. 03-515A.". Rockville, MD.: Agency for Healthcare Research and Quality. Retrieved June 5, 2010.
- 1 2 U.S. Preventive Services Task Force (March 2012). "Screening for Cervical Cancer: Clinical Summary of USPSTF Recommendation". uspreventiveservicestaskforce.org. Retrieved 31 July 2012.
- 1 2 American Academy of Family Physicians. "Five Things Physicians and Patients Should Question" (PDF). Choosing Wisely: an initiative of the ABIM Foundation (American Academy of Family Physicians). Retrieved August 14, 2012{{inconsistent citations}}
- 1 2 3 4 5 6 Arbyn M, Anttila A, Jordan J, Ronco G, Schenck U, Segnan N, Wiener H, Herbert A, von Karsa L (2010). "European Guidelines for Quality Assurance in Cervical Cancer Screening. Second Edition—Summary Document". Annals of Oncology 21 (3): 448–458. doi:10.1093/annonc/mdp471. PMC 2826099. PMID 20176693.
- 1 2 Strander B (2009). "At what age should cervical screening stop?". Brit Med J 338: 1022–23. doi:10.1136/bmj.b809. PMID 19395422.
- 1 2 Sasieni P, Adams J, Cuzick J (2003). "Benefit of cervical screening at different ages: evidence from the UK audit of screening histories". Br J Cancer 89 (1): 88–93. doi:10.1038/sj.bjc.6600974. PMC 2394236. PMID 12838306.
- 1 2 3 4 Society of Gynecologic Oncology (February 2014). "Five Things Physicians and Patients Should Question". Choosing Wisely: an initiative of the ABIM Foundation (Society of Gynecologic Oncology). Retrieved 19 February 2013{{inconsistent citations}}, which cites
- Salani R, Backes FJ, Fung MF, Holschneider CH, Parker LP, Bristow RE, Goff BA (2011). "Posttreatment surveillance and diagnosis of recurrence in women with gynecologic malignancies: Society of Gynecologic Oncologists recommendations". American Journal of Obstetrics and Gynecology 204 (6): 466–78. doi:10.1016/j.ajog.2011.03.008. PMID 21752752.
- Salani R, Nagel CI, Drennen E, Bristow RE (2011). "Recurrence patterns and surveillance for patients with early stage endometrial cancer". Gynecologic Oncology 123 (2): 205–7. doi:10.1016/j.ygyno.2011.07.014. PMID 21820709.
- Bristow RE, Purinton SC, Santillan A, Diaz-Montes TP, Gardner GJ, Giuntoli RL (2006). "Cost-effectiveness of routine vaginal cytology for endometrial cancer surveillance". Gynecologic Oncology 103 (2): 709–13. doi:10.1016/j.ygyno.2006.05.013. PMID 16797686.
- ↑ "ACOG Committee on Gynecologic Practice; Routine Pelvic Examination and Cervical Cytology Screening, Opinion #413". Obstetrics and Gynecology 113 (5): 1190–1193. 2009. doi:10.1097/AOG.0b013e3181a6d022. PMID 19384150.
- ↑ American Congress of Obstetricians and Gynecologists. "Five Things Physicians and Patients Should Question". Choosing Wisely: an initiative of the ABIM Foundation (American Congress of Obstetricians and Gynecologists). Retrieved August 1, 2013., which cites
- Boulware LE, Marinopoulos S, Phillips KA, Hwang CW, Maynor K, Merenstein D, Wilson RF, Barnes GJ, Bass EB, Powe NR, Daumit GL (2007). "Systematic review: The value of the periodic health evaluation". Annals of Internal Medicine 146 (4): 289–300. doi:10.7326/0003-4819-146-4-200702200-00008. PMID 17310053.
- Saslow D, Solomon D, Lawson HW, Killackey M, Kulasingam SL, Cain J, Garcia FA, Moriarty AT, Waxman AG, Wilbur DC, Wentzensen N, Downs LS, Spitzer M, Moscicki AB, Franco EL, Stoler MH, Schiffman M, Castle PE, Myers ER (2012). "American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer". CA Cancer J Clin 62 (3): 147–72. doi:10.3322/caac.21139. PMC 3801360. PMID 22422631.
- "Committee Opinion No. 534". Obstetrics & Gynecology 120 (2, Part 1): 421–424. 2012. doi:10.1097/AOG.0b013e3182680517. PMID 22825111.
- "ACOG Practice Bulletin Number 131: Screening for cervical cancer". Obstetrics and gynecology 120 (5): 1222–1238. 2012. doi:10.1097/AOG.0b013e318277c92a. PMID 23090560.
- ↑ Sasieni, P; Castanon, A; Cuzick, J; Snow, J; (2009). "Effectiveness of Cervical Screening with Age: Population based Case-Control Study of Prospectively Recorded Data". BMJ 339: 2968–2974. doi:10.1136/bmj.b2968.
- ↑ Marrazzo JM, Koutsky LA, Kiviat NB, Kuypers JM, Stine K (2001). "Papanicolaou test screening and prevalence of genital human papillomavirus among women who have sex with women". American Journal of Public Health 91 (6): 947–952. doi:10.2105/AJPH.91.6.947. PMC 1446473. PMID 11392939.
- ↑ Smith, RA; et al. (2002). "American Cancer Society Guideline for the Early Detection of Cervical Neoplasia and Cancer" 52 (1): 8–22.
ACS and others have recommended, since before 1980, that conventional cytology can be safely performed up to every three years for most women.
- 1 2 DeMay, M. (2007). Practical principles of cytopathology. Revised edition. Chicago, IL: American Society for Clinical Pathology Press. ISBN 978-0-89189-549-7.
- ↑ "Cancer Research UK website". Retrieved 2009-01-03.
- ↑ Raffle AE, Alden B, Quinn M, Babb PJ, Brett MT (2003). "Outcomes of screening to prevent cancer: analysis of cumulative incidence of cervical abnormality and modelling of cases and deaths prevented". BMJ 326 (7395): 901. doi:10.1136/bmj.326.7395.901. PMC 153831. PMID 12714468.
- ↑ "Pap Smear". Retrieved 2008-12-27.
- ↑ Eversole GM, Moriarty AT, Schwartz MR, Clayton AC, Souers R, Fatheree LA, Chmara BA, Tench WD, Henry MR, Wilbur DC (2010). "Practices of participants in the college of american pathologists interlaboratory comparison program in cervicovaginal cytology, 2006". Archives of pathology & laboratory medicine 134 (3): 331–5. doi:10.1043/1543-2165-134.3.331. PMID 20196659.
- ↑ Nayar R, Solomon D. Second edition of 'The Bethesda System for reporting cervical cytology' – Atlas, website, and Bethesda interobserver reproducibility project. CytoJournal [serial online] 2004 [cited 2011 Apr 16];1:4. Available from: http://www.cytojournal.com/text.asp?2004/1/1/4/41272
- 1 2 PapScreen Victoria > Pregnant women from Cancer Council Victoria 2014
- ↑ Michael CW (1999). "The Papanicolaou Smear and the Obstetric Patient: A Simple Test with Great Benefits". Diagnostic Cytopathology 21 (1): 1–3. doi:10.1002/(SICI)1097-0339(199907)21:1<1::AID-DC1>3.0.CO;2-0. PMID 10405797.
- ↑ Lanouette JM, Puder KS, Berry SM, Bryant DR, Dombrowski MP (1997). "Is inflammation on Papanicolaou smear a risk factor for preterm delivery?". Fetal diagnosis and therapy 12 (4): 244–247. doi:10.1159/000264477. PMID 9354886.
- ↑ "Pregnant women". papscreen.org. Cancer Council Victoria. Retrieved 2015-01-16.
- ↑ "Excerpts from Changing Bodies, Changing Lives". Our Bodies Ourselves. Retrieved 2013-07-02.
- ↑ http://journals.lww.com/co-anesthesiology/Abstract/2010/06000/Changes_in_uterine_innervation_in_pregnancy_and.3.aspx |title=Changes in uterine innervation in pregnancy and during labour |publisher=Current Opinion in Anaesthesiology |date=June 2010 |accessdate=2016-02-13
- ↑ Wright, Jessica L. (2010). "The Effect of Using Water-based Gel Lubricant During a Speculum Exam On Pap Smear Results". School of Physician Assistant Studies. Pacific University. Retrieved 4 February 2012.
- ↑ Martin-Hirsch P, Lilford R, Jarvis G, Kitchener HC (1999). "Efficacy of cervical-smear collection devices: a systematic review and meta-analysis". Lancet 354 (9192): 1763–1770. doi:10.1016/S0140-6736(99)02353-3. PMID 10577637.
- ↑ Biscotti CV, Dawson AE, Dziura B, Galup L, Darragh T, Rahemtulla A, Wills-Frank L (2005). "Assisted primary screening using the automated ThinPrep Imaging System". Am. J. Clin. Pathol. 123 (2): 281–7. doi:10.1309/AGB1MJ9H5N43MEGX. PMID 15842055.
- ↑ Willis BH, Barton P, Pearmain P, Bryan S, Hyde C, "Cervical screening programmes: can automation help? Evidence from systematic reviews, an economic analysis and a simulation modelling exercise applied to the UK". Health Technol Assess 2005 9(13).
- ↑ Davey E, d'Assuncao J, Irwig L, Macaskill P, Chan SF, Richards A, Farnsworth A (2007). "Accuracy of reading liquid based cytology slides using the ThinPrep Imager compared with conventional cytology: prospective study". BMJ 335 (7609): 31. doi:10.1136/bmj.39219.645475.55. PMC 1910624. PMID 17604301.
- ↑ Bettigole C (2013). "The Thousand-Dollar Pap Smear". New England Journal of Medicine 369 (16): 1486–1487. doi:10.1056/NEJMp1307295. PMID 24131176.
- ↑ M.J. O'Dowd, E.E. Philipp, The History of Obstetrics & Gynaecology, London, Parthenon Publishing Group, 1994, p. 547.
- ↑ Diamantis A, Magiorkinis E, Androutsos G (Jul 2010). "What's in a name? Evidence that Papanicolaou, not Babes, deserves credit for the Pap test". Diagn Cytopathol 38 (7): 473–6. doi:10.1002/dc.21226.
- ↑ Koss, Leopold G. M.D., International Journal of Gynecology Pathology, http://journals.lww.com/intjgynpathology/Fulltext/2003/01000/Aurel_Babes.20.aspx#P20
- ↑ Bewtra C, Pathan M, Hashish H. Abnormal Pap smears with negative follow-up biopsies: Improving cytohistologic correlations. http://onlinelibrary.wiley.com/doi/10.1002/dc.10329/abstract
- ↑ Fang-Hsin Leea, Chung-Yi Lic, Hsiu-Hung Wanga, Yung-Mei Yang. "The utilization of Pap tests among different female medical personnel: A nationwide study in Taiwan". Preventive Medicine 56 (6): 406–409. doi:10.1016/j.ypmed.2013.03.001. Retrieved September 20, 2013.
- ↑ http://web.ebscohost.com/ehost/pdfviewer/pdfviewer?sid=c456f9bb-cab6-4f69-a99e-d44cf337b135%40sessionmgr111&vid=2&hid=127#944 (see Tables 3 and 4)
- ↑ NB Peterson; HJ Murff; Y Cui; M Hargreaves; JH Fowke (Jul–Aug 2008). "Papanicolaou testing among women in the southern United States". Journal of Women's Health 17 (6): 939–46. doi:10.1089/jwh.2007.0576. Retrieved October 15, 2013.
- 1 2 OB-GYN 101: Introductory Obstetrics & Gynecology > Coccoid Bacteria by Michael Hughey Hughey at Texas Tech University Health Sciences Center. Retrieved Feb 2014.
External links
- The Pap Test: Questions and Answers — from the U.S.'s National Cancer Institute
- MedlinePlus: Cervical Cancer Prevention/Screening — from MedlinePlus
- NHS Cervical Screening Programme — from the UK's National Health Service
- Cervical cancer screening information – from Cancer Research UK
- Pap Smear – from Lab Tests Online
- Pap Smear — from eMedicineHealth
- PapScreen – Australian information about Pap tests (or Pap smears)
- Jo's Trust – UK's leading cervical cancer charity.
- Canadian Guidelines for Cervical Cancer Screening – Society of Obstetricians and Gynaecologists of Canada
| ||||||||||||||||||||||||||||||||||