Osteoarthritis
| Osteoarthritis | |
|---|---|
 The formation of hard nobs at the middle finger joints (known as Bouchard's nodes) and at the farther away finger joint (known as Heberden's node) are a common feature of OA in the hands. | |
| Classification and external resources | |
| Synonyms | degenerative arthritis, degenerative joint disease, osteoarthrosis |
| Specialty | Rheumatology, orthopedics |
| ICD-10 | M15-M19, M47 |
| ICD-9-CM | 715 |
| OMIM | 165720 |
| DiseasesDB | 9313 |
| MedlinePlus | 000423 |
| eMedicine | med/1682 orthoped/427 pmr/93 radio/492 |
| Patient UK | Osteoarthritis |
| MeSH | D010003 |
Osteoarthritis (OA) is a type of joint disease that results from breakdown of joint cartilage and underlying bone.[1] The most common symptoms are joint pain and stiffness. Initially, symptoms may occur only following exercise, but over time may become constant. Other symptoms may include joint swelling, decreased range of motion, and when the back is affected weakness or numbness of the arms and legs. The most commonly involved joints are those near the ends of the fingers, at the base of the thumb, neck, lower back, knees, and hips. Joints on one side of the body are often more affected than those on the other. Usually the problems come on over years. It can affect work and normal daily activities. Unlike other types of arthritis, only the joints are typically affected.[2]
Causes include previous joint injury, abnormal joint or limb development, and inherited factors. Risk is greater in those who are overweight, have one leg of a different length, and have jobs that result in high levels of joint stress.[2][3] Osteoarthritis is believed to be caused by mechanical stress on the joint and low grade inflammatory processes.[4] It develops as cartilage is lost with eventually the underlying bone becoming affected.[2] As pain may make it difficult to exercise, muscle loss may occur.[3][5] Diagnosis is typically based on signs and symptoms with medical imaging and other tests occasionally used to either support or rule out other problems. Unlike in rheumatoid arthritis, which is primarily an inflammatory condition, the joints do not typically become hot or red.[2]
Treatment includes exercise, efforts to decrease joint stress, support groups, and pain medications. Efforts to decrease joint stress include resting and the use of a cane. Weight loss may help in those who are overweight. Pain medications may include paracetamol (acetaminophen). If this does not work NSAIDs such as naproxen may be used, but these medications are associated with greater side effects. Opioids if used are generally only recommended short term due to the risk of addiction.[2] If pain interferes with normal life despite other treatments, joint replacement surgery may help. An artificial joint, however, only lasts a limited amount of time.[3] Outcomes for most people with osteoarthritis are good.[2]
OA is the most common form of arthritis with disease of the knee and hip affecting about 3.8% of people as of 2010.[2][6] Among those over 60 years old about 10% of males and 18% of females are affected.[3] It is the cause of about 2% of years lived with disability.[6] In Australia about 1.9 million people are affected,[7] and in the United States about 27 million people are affected.[2] Before 45 years of age it is more common in men, while after 45 years of age it is more common in women. It becomes more common in both sexes as people become older.[2]
Signs and symptoms

The main symptom is pain, causing loss of ability and often stiffness. "Pain" is generally described as a sharp ache or a burning sensation in the associated muscles and tendons. OA can cause a crackling noise (called "crepitus") when the affected joint is moved or touched and people may experience muscle spasms and contractions in the tendons. Occasionally, the joints may also be filled with fluid.[8] Some people report increased pain associated with cold temperature, high humidity, and/or a drop in barometric pressure, but studies have had mixed results.[9]
OA commonly affects the hands, feet, spine, and the large weight bearing joints, such as the hips and knees, although in theory, any joint in the body can be affected. As OA progresses, the affected joints appear larger, are stiff, painful and may swell, but usually feel better with gentle use but worse with excessive or prolonged use, thus distinguishing it from rheumatoid arthritis.
In smaller joints, such as at the fingers, hard bony enlargements, called Heberden's nodes (on the distal interphalangeal joints) and/or Bouchard's nodes (on the proximal interphalangeal joints), may form, and though they are not necessarily painful, they do limit the movement of the fingers significantly. OA at the toes leads to the formation of bunions, rendering them red or swollen. Some people notice these physical changes before they experience any pain.
OA is the most common cause of a joint effusion of the knee.[10]
Risk factors
Damage from mechanical stress with insufficient self repair by joints is believed to be the primary cause of osteoarthritis.[11] Sources of this stress may include misalignments of bones caused by congenital or pathogenic causes; mechanical injury; excess body weight; loss of strength in the muscles supporting a joint; and impairment of peripheral nerves, leading to sudden or uncoordinated movements.[11] However exercise, including running in the absence of injury, has not been found to increase the risk.[12] Nor has cracking one's knuckles been found to play a role.[13]
Primary
A number of studies have shown that there is a greater prevalence of the disease among siblings and especially identical twins, indicating a hereditary basis.[14] Although a single factor is not generally sufficient to cause the disease, about half of the variation in susceptibility has been assigned to genetic factors.[15]
As early human ancestors evolved into bipeds, changes occurred in the pelvis, hip joint and spine which increased the risk of osteoarthritis.[16] Additionally genetic variations that increase the risk were likely not selected against because usually problems only occur after reproductive success.[17]
The development of OA is correlated with a history of previous joint injury and with obesity, especially with respect to knees.[18] Since the correlation with obesity has been observed not only for knees but also for non-weight bearing joints and the loss of body fat is more closely related to symptom relief than the loss of body weight, it has been suggested that there may be a metabolic link to body fat as opposed to just mechanical loading.[19]
Changes in sex hormone levels may play a role in the development of OA as it is more prevalent among post-menopausal women than among men of the same age.[20][21] A study of mice found natural female hormones to be protective while injections of the male hormone dihydrotestosterone reduced protection.[22]
Secondary


This type of osteoarthritis is caused by other factors but the resulting pathology is the same as for primary osteoarthritis:
- Alkaptonuria
- Congenital disorders of joints
- Diabetes doubles the risk of having a joint replacement due to OA and people with diabetes have joint replacements at a younger age than those without diabetes.[23]
- Ehlers-Danlos Syndrome
- Hemochromatosis and Wilson's disease
- Inflammatory diseases (such as Perthes' disease), (Lyme disease), and all chronic forms of arthritis (e.g., costochondritis, gout, and rheumatoid arthritis). In gout, uric acid crystals cause the cartilage to degenerate at a faster pace.
- Injury to joints or ligaments (such as the ACL), as a result of an accident or orthopedic operations.
- Ligamentous deterioration or instability may be a factor.
- Marfan syndrome
- Obesity
- Joint infection
Pathophysiology


While OA is a degenerative joint disease that may cause gross cartilage loss and morphological damage to other joint tissues, more subtle biochemical changes occur in the earliest stages of OA progression. The water content of healthy cartilage is finely balanced by compressive force driving water out & swelling pressure drawing water in.[25] Collagen fibres exert the compressive force, whereas the Gibbs–Donnan effect & cartilage proteoglycans create osmotic pressure which tends to draw water in.[25]
However, during onset of OA, the collagen matrix becomes more disorganized and there is a decrease in proteoglycan content within cartilage. The breakdown of collagen fibers results in a net increase in water content.[26][27][28][29][30] This increase occurs because whilst there is an overall loss of proteoglycans (and thus a decreased osmotic pull),[27][31] it is outweighed by a loss of collagen.[25][31] Without the protective effects of the proteoglycans, the collagen fibers of the cartilage can become susceptible to degradation and thus exacerbate the degeneration. Inflammation of the synovium (joint cavity lining) and the surrounding joint capsule can also occur, though often mild (compared to what occurs in rheumatoid arthritis). This can happen as breakdown products from the cartilage are released into the synovial space, and the cells lining the joint attempt to remove them.
Other structures within the joint can also be affected.[32] The ligaments within the joint become thickened and fibrotic and the menisci can become damaged and wear away.[33] Menisci can be completely absent by the time a person undergoes a joint replacement. New bone outgrowths, called "spurs" or osteophytes, can form on the margins of the joints, possibly in an attempt to improve the congruence of the articular cartilage surfaces in the absence of the menisci. The subchondral bone volume increases and becomes less mineralized (hypomineralization).[34] All these changes can cause problems functioning. The pain in an osteoarthritic joint has been related to thickened synovium[35] and subchondral bone lesions.[36]
Diagnosis
Diagnosis is made with reasonable certainty based on history and clinical examination.[37][38] X-rays may confirm the diagnosis. The typical changes seen on X-ray include: joint space narrowing, subchondral sclerosis (increased bone formation around the joint), subchondral cyst formation, and osteophytes.[39] Plain films may not correlate with the findings on physical examination or with the degree of pain.[40] Usually other imaging techniques are not necessary to clinically diagnose OA.
In 1990, the American College of Rheumatology, using data from a multi-center study, developed a set of criteria for the diagnosis of hand OA based on hard tissue enlargement and swelling of certain joints.[41] These criteria were found to be 92% sensitive and 98% specific for hand OA versus other entities such as rheumatoid arthritis and spondyloarthropathies.[42]
Related pathologies whose names may be confused with OA include pseudo-arthrosis. This is derived from the Greek words pseudo, meaning "false", and arthrosis, meaning "joint." Radiographic diagnosis results in diagnosis of a fracture within a joint, which is not to be confused with OA which is a degenerative pathology affecting a high incidence of distal phalangeal joints of female patients. A polished ivory-like appearance may also develop on the bones of the affected joints, reflecting a change called eburnation.[43]
-

Severe osteoarthritis and osteopenia of the carpal joint and 1st carpometacarpel joint.
-

MRI of osteoarthritis in the knee, with characteristic narrowing of the joint space.
-

Primary osteoarthritis of the left knee. Note the osteophytes, narrowing of the joint space (arrow), and increased subchondral bone density (arrow).
-

Damaged cartilage from sows. (a) cartilage erosion (b)cartilage ulceration (c)cartilage repair (d)osteophyte (bone spur) formation.
-
_at_knee_joint.jpg)
Histopathology of osteoarthrosis of a knee joint in an elderly female.
-
_at_knee_joint.jpg)
Histopathology of osteoarthrosis of a knee joint in an elderly female.
-
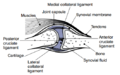
In a healthy joint, the ends of bones are encased in smooth cartilage. Together, they are protected by a joint capsule lined with a synovial membrane that produces synovial fluid. The capsule and fluid protect the cartilage, muscles, and connective tissues.
-

With osteoarthritis, the cartilage becomes worn away. Spurs grow out from the edge of the bone, and synovial fluid increases. Altogether, the joint feels stiff and sore.
-

Osteoarthritis
Classification
A number of classification systems are used for gradation of osteoarthritis:
OA can be classified into either primary or secondary depending on whether or not there is an identifiable underlying cause.
Both primary generalized nodal OA and erosive OA (EOA, also called inflammatory OA) are sub-sets of primary OA. EOA is a much less common, and more aggressive inflammatory form of OA which often affects the distal interphalangeal joints of the hand and has characteristic articular erosive changes on x-ray.[44]
Management

Lifestyle modification (such as weight loss and exercise) and analgesics are the mainstays of treatment. Acetaminophen (also known as paracetamol) is recommended first line with NSAIDs being used as add on therapy only if pain relief is not sufficient.[45] This is due to the relative greater safety of acetaminophen.[45]
Lifestyle modification
For overweight people, weight loss may be an important factor.[46] Patient education has been shown to be helpful in the self-management of arthritis.[46] It decreases pain, improves function, reduces stiffness and fatigue, and reduces medical usage.[46] Patient education can provide on average 20% more pain relief when compared to NSAIDs alone in patients with hip OA.[46]
Physical measures
Moderate exercise is beneficial with respect to pain and function in those with osteoarthritis of the knee and hip.[47][48] These exercises should occur at least three times per week.[49] While some evidence supports certain physical therapies, evidence for a combined program is limited.[50] There is not enough evidence to determine the effectiveness of massage therapy.[51] The evidence for manual therapy is inconclusive.[52] Functional, gait, and balance training have been recommended to address impairments of position sense, balance, and strength in individuals with lower extremity arthritis as these can contribute to a higher rate of falls in older individuals.[53]
Lateral wedge insoles and neutral insoles do not appear to be useful in osteoarthritis of the knee.[54][55][56] Knee braces may help[57] but their usefulness has also been disputed.[56] For pain management heat can be used to relieve stiffness, and cold can relieve muscle spasms and pain.[58]
Medication
| Treatment recommendations by risk factors | ||
|---|---|---|
| GI risk | Stroke and heart risk | Option |
| Low | Low | NSAID, or paracetamol[59] |
| Moderate | Low | Paracetamol, or low dose NSAID with antacid[59] |
| Low | Moderate | Paracetamol, or low dose aspirin with an antacid[59] |
| Moderate | Moderate | Low dose paracetamol, aspirin, and antacid. Monitoring for abdominal pain or black stool.[59] |
The analgesic acetaminophen is the first line treatment for OA.[45][60] However, a 2015 review found acetaminophen to only have a small short term benefit.[61] For mild to moderate symptoms effectiveness is similar to non-steroidal anti-inflammatory drugs (NSAIDs), though for more severe symptoms NSAIDs may be more effective.[45] NSAIDs such as naproxen while more effective in severe cases are associated with greater side effects such as gastrointestinal bleeding.[45] Another class of NSAIDs, COX-2 selective inhibitors (such as celecoxib) are equally effective to NSAIDs with lower rates of adverse gastrointestinal effects but higher rates of cardiovascular disease such as myocardial infarction.[62] They are also more expensive than non-specific NSAIDs.[63] Oral opioids, including both weak opioids such as tramadol and stronger opioids, are also often prescribed. Their appropriateness is uncertain and opioids are often recommended only when first line therapies have failed or are contraindicated.[64][65] This is due to a small benefit and relatively large risk of side effects.[66] Oral steroids are not recommended in the treatment of OA.[60]
There are several NSAIDs available for topical use including diclofenac. Topical and oral diclofenac work equally well with topical having a greater risk of mild skin reactions but no greater risk of gastrointestinal adverse effects.[67] Transdermal opioid pain medications are not typically recommended in the treatment of osteoarthritis.[68] Topical capsaicin is controversial with some reviews finding benefit[69][70] and others not.[71]
Joint injections of glucocorticoids (such as hydrocortisone) leads to short term pain relief that may last between a few weeks and a few months.[72] Injections of hyaluronic acid have not been found to lead to much improvement compared to placebo when the knee joint is affected[73][74] but have been associated with harm.[74] This may stand true for hip osteoarthiritis. In ankle osteoarthritis evidence is unclear.[75] The effectiveness of injections of platelet-rich plasma is unclear; there are suggestions that such injections improve function but not pain and are associated with increased risk.[76][77]
Surgery
If problems are significant and more conservative management is ineffective, joint replacement surgery or resurfacing may be recommended. Evidence supports joint replacement for both knees and hips as it is both clinically effective,[78][79] and cost-effective.[80][81] Surgery to transfer articular cartilage from a non-weight-bearing area to the damaged area is one possible procedure that has some success but there are problems getting the transferred cartilage to integrate well with the existing cartilage at the transfer site.[82]
Osteotomy may be useful in people with knee osteoarthritis but has not been well studied.[83] Arthroscopic surgery is largely not recommended as it does not improve outcomes in knee osteoarthritis.[84][85] Additionally arthroscopy may result in harm.[86]
Alternative medicine
Many dietary supplements are sold as treatments for OA. Since glucosamine is a precursor for a component of cartilage, it has been studied for prevention and treatment. The effectiveness of glucosamine is controversial.[87][88] Most recent reviews found it to be equal to[89][90] or only slight better than placebo.[91][92] A difference may exist between glucosamine sulfate and glucosamine hydrochloride, with glucosamine sulfate showing a benefit and glucosamine hydrochloride not.[93] The evidence for glucosamine sulfate having an effect on OA progression is somewhat unclear and if present likely modest.[94] The Osteoarthritis Research Society International recommends that glucosamine be discontinued if no effect is observed after six months[95] and the National Institute of Clinical Excellence no longer recommends its use.[5] Despite the difficulty in determining the efficacy of glucosamine, it remains a viable treatment option.[96] Its use as a therapy for osteoarthritis is usually safe.[96]
Phytodolor,[69] SAMe,[97] and SKI 306X (a Chinese herbal mixture)[70] may be effective in improving pain, and there is some evidence to support the use of cat's claw as an anti-inflammatory.[98] There is tentative evidence to support avocado/soybean unsaponifiables (ASU),[70][99] methylsulfonylmethane,[69] and rose hip.[69] A few high-quality studies of Boswellia serrata show consistent, but small, improvements in pain and function among people with osteoarthritis.[100]
There is little evidence supporting benefits for some supplements, including: the Ayurvedic herbal preparations with brand names Articulin F and Eazmov, collagen, devil's claw, Duhuo Jisheng Wan (a Chinese herbal preparation), fish liver oil, ginger, the herbal preparation gitadyl, glucosamine, hyaluronic acid, omega-3 fatty acids, the brand-name product Reumalax, stinging nettle, turmeric, vitamins A, C, and E in combination, vitamin E alone, vitamin K and willow bark. There is insufficient evidence to make a recommendation about the safety and efficacy of these treatments.[69][98]
While acupuncture leads to improvements in pain relief, this improvement is small and may be of questionable importance. Waiting list-controlled trials for peripheral joint osteoarthritis do show clinically relevant benefits, but these may be due to placebo effects.[101] Acupuncture does not seem to produce long-term benefits.[102] While electrostimulation techniques such as TENS have been used for twenty years to treat osteoarthritis in the knee, there is no conclusive evidence to show that it reduces pain or disability.[103]
A Cochrane review of low level laser therapy found unclear evidence of benefit.[104] Another review found short term pain relief for osteoarthritic knees.[105]
Epidemiology

no data
≤ 200
200–220
220–240
240–260
260–280
280–300
|
300–320
320–340
340–360
360–380
380–400
≥ 400
|
Globally approximately 250 million people have osteoarthritis of the knee (3.6% of the population).[107] OA affects nearly 27 million people in the United States, accounting for 25% of visits to primary care physicians, and half of all NSAID prescriptions. It is estimated that 80% of the population have radiographic evidence of OA by age 65, although only 60% of those will have symptoms.[108]
As of 2004, OA globally causes moderate to severe disability in 43.4 million people.[109]
In the United States, there were approximately 964,000 hospitalizations for osteoarthritis in 2011, a rate of 31 stays per 10,000 population.[110] With an aggregate cost of $14.8 billion ($15,400 per stay), it was the second-most expensive condition seen in U.S. hospital stays in 2011. By payer, it was the second-most costly condition billed to Medicare and private insurance.[111][112]
History
Evidence for OA found in the fossil record is studied by paleopathologists, specialists in ancient disease and injury. OA has been reported in fossils of the large carnivorous dinosaur Allosaurus fragilis.[113]
Etymology
OA is derived from the Greek word part osteo-, meaning "of the bone", combined with arthritis: arthr-, meaning "joint", and -itis, the meaning of which has come to be associated with inflammation.[114] The -itis of OA could be considered misleading as inflammation is not a conspicuous feature. Some clinicians refer to this condition as osteoarthosis to signify the lack of inflammatory response.
Research
There are ongoing efforts to determine if there are agents that modify outcomes in OA. Sprifermin is one candidate drug. There is also tentative evidence that strontium ranelate may decrease degeneration in OA and improve outcomes.[115][116]
As well as attempting to find disease-modifying agents for OA, there is emerging evidence that a system-based approach is necessary to find the causes of OA.[117] Changes may occur before clinical disease is evident due to abnormalities in biomechanics, biology and/or structure of joints that predispose them to develop clinical disease. Research is thus focusing on defining these early pre-OA changes using biological, mechanical, and imaging markers of OA risk, emphasising multi-disciplinary approaches, and looking into personalized interventions that can reverse OA risk in healthy joints before the disease becomes evident.
Gene transfer strategies aim to target the disease process rather than the symptoms.[118]
Biomarkers
Guidelines outlining requirements for inclusion of soluble biomarkers in OA clinical trials were published in 2015,[119] but as yet, there are no validated biomarkers for OA. A 2015 systematic review of biomarkers for OA looking for molecules that could be used for risk assessments found 37 different biochemical markers of bone and cartilage turnover in 25 publications.[120] The strongest evidence was for urinary C-terminal telopeptide of collagen type II (uCTX-II) as a prognostic marker for knee OA progression and serum cartilage oligomeric protein (COMP) levels as a prognostic marker for incidence of both knee and hip OA. A review of biomarkers in hip OA also found associations with uCTXII.[121]
One problem with using a specific collagen type II biomarker from the breakdown of articular cartilage is that the amount of cartilage is reduced (worn away) over time with progression of the disease so a patient can eventually have very advanced OA with none of this biomarker detectable in their urine. Another problem with a systemic biomarker is that a patient can have OA in multiple joints at different stages of disease at the same time, so the biomarker source cannot be determined. Some other collagen breakdown products in the synovial fluid correlated with each other after acute injuries (a known cause of secondary OA) but did not correlate with the severity of the injury.[122]
References
- ↑ Atlas of Osteoarthritis. Springer. 2015. p. 21. ISBN 9781910315163.
- 1 2 3 4 5 6 7 8 9 "Osteoarthritis". National Institute of Arthritis and Musculoskeletal and Skin Diseases. April 2015. Retrieved 13 May 2015.
- 1 2 3 4 Glyn-Jones, S; Palmer, AJ; Agricola, R; Price, AJ; Vincent, TL; Weinans, H; Carr, AJ (3 March 2015). "Osteoarthritis.". Lancet 386: 376–87. doi:10.1016/S0140-6736(14)60802-3. PMID 25748615.
- ↑ Berenbaum F (2013). "Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!)". Osteoarthritis and Cartilage 21 (1): 16–21. doi:10.1016/j.joca.2012.11.012. PMID 23194896.
- 1 2 Conaghan P (2014). "Osteoarthritis — Care and management in adults" (PDF).
- 1 2 March, L; Smith, EU; Hoy, DG; Cross, MJ; Sanchez-Riera, L; Blyth, F; Buchbinder, R; Vos, T; Woolf, AD (June 2014). "Burden of disability due to musculoskeletal (MSK) disorders.". Best practice & research. Clinical rheumatology 28 (3): 353–66. doi:10.1016/j.berh.2014.08.002. PMID 25481420.
- ↑ Elsternwick (2013). "A problem worth solving.". Arthritis and Osteoporosis Victoria.
- ↑ MedlinePlus Encyclopedia Osteoarthritis
- ↑ de Figueiredo EC, Figueiredo GC, Dantas RT (December 2011). "Influência de elementos meteorológicos na dor de pacientes com osteoartrite: Revisão da literatura" [Influence of meteorological elements on osteoarthritis pain: a review of the literature]. Rev Bras Reumatol (in Portuguese) 51 (6): 622–8. doi:10.1590/S0482-50042011000600008. PMID 22124595.
- ↑ "Water on the knee". MayoClinic.com.
- 1 2 Brandt KD, Dieppe P, Radin E (January 2009). "Etiopathogenesis of osteoarthritis". Med. Clin. North Am. 93 (1): 1–24, xv. doi:10.1016/j.mcna.2008.08.009. PMID 19059018.
- ↑ Bosomworth NJ (September 2009). "Exercise and knee osteoarthritis: benefit or hazard?". Can Fam Physician 55 (9): 871–8. PMC 2743580. PMID 19752252.
- ↑ Deweber K, Olszewski M, Ortolano R (2011). "Knuckle cracking and hand osteoarthritis". J Am Board Fam Med 24 (2): 169–74. doi:10.3122/jabfm.2011.02.100156. PMID 21383216.
- ↑ Valdes AM, Spector TD (August 2008). "The contribution of genes to osteoarthritis". Rheum. Dis. Clin. North Am. 34 (3): 581–603. doi:10.1016/j.rdc.2008.04.008. PMID 18687274.
- ↑ Spector TD, MacGregor AJ (2004). "Risk factors for osteoarthritis: genetics". Osteoarthr. Cartil. 12 Suppl A: S39–44. doi:10.1016/j.joca.2003.09.005. PMID 14698640.
- ↑ Hogervorst T, Bouma HW, de Vos J (August 2009). "Evolution of the hip and pelvis.". Acta orthopaedica. Supplementum 80 (336): 1–39. doi:10.1080/17453690610046620. PMID 19919389.
- ↑ van der Kraan PM, van den Berg WB (April 2008). "Osteoarthritis in the context of ageing and evolution. Loss of chondrocyte differentiation block during ageing.". Ageing Research Reviews 7 (2): 106–13. doi:10.1016/j.arr.2007.10.001. PMID 18054526.
- ↑ Coggon D, Reading I, Croft P, McLaren M, Barrett D, Cooper C (May 2001). "Knee osteoarthritis and obesity". Int. J. Obes. Relat. Metab. Disord. 25 (5): 622–7. doi:10.1038/sj.ijo.0801585. PMID 11360143.
- ↑ Pottie P, Presle N, Terlain B, Netter P, Mainard D, Berenbaum F (November 2006). "Obesity and osteoarthritis: more complex than predicted!". Ann. Rheum. Dis. 65 (11): 1403–5. doi:10.1136/ard.2006.061994. PMC 1798356. PMID 17038451.
- ↑ Linn S, Murtaugh B, Casey E (May 2012). "Role of sex hormones in the development of osteoarthritis". PM&R 4 (5 Suppl): S169–73. doi:10.1016/j.pmrj.2012.01.013. PMID 22632696.
- ↑ Tanamas SK, Wijethilake P, Wluka AE, Davies-Tuck ML, Urquhart DM, Wang Y, Cicuttini FM (June 2011). "Sex hormones and structural changes in osteoarthritis: a systematic review". Maturitas 69 (2): 141–56. doi:10.1016/j.maturitas.2011.03.019. PMID 21481553.
- ↑ Ma HL, Blanchet TJ, Peluso D, Hopkins B, Morris EA, Glasson SS (June 2007). "Osteoarthritis severity is sex dependent in a surgical mouse model". Osteoarthr. Cartil. 15 (6): 695–700. doi:10.1016/j.joca.2006.11.005. PMID 17207643.
- ↑ King KB, Rosenthal AK (2015). "The adverse effects of diabetes on osteoarthritis: update on clinical evidence and molecular mechanisms". Osteoarthritis Cartilage 23 (6): 841–50. doi:10.1016/j.joca.2015.03.031. PMID 25837996.
- ↑ "OpenStax CNX". cnx.org. Retrieved 2015-10-14.
- 1 2 3 Maroudas AI (April 1976). "Balance between swelling pressure and collagen tension in normal and degenerate cartilage". Nature 260 (5554): 808–9. doi:10.1038/260808a0. PMID 1264261.
- ↑ Bollet AJ, Nance JL (July 1966). "Biochemical Findings in Normal and Osteoarthritic Articular Cartilage. II. Chondroitin Sulfate Concentration and Chain Length, Water, and Ash Content". J. Clin. Invest. 45 (7): 1170–7. doi:10.1172/JCI105423. PMC 292789. PMID 16695915.
- 1 2 Brocklehurst R, Bayliss MT, Maroudas A, Coysh HL, Freeman MA, Revell PA, Ali SY (January 1984). "The composition of normal and osteoarthritic articular cartilage from human knee joints. With special reference to unicompartmental replacement and osteotomy of the knee". J Bone Joint Surg Am 66 (1): 95–106. PMID 6690447.
- ↑ Chou MC, Tsai PH, Huang GS, Lee HS, Lee CH, Lin MH, Lin CY, Chung HW (April 2009). "Correlation between the MR T2 value at 4.7 T and relative water content in articular cartilage in experimental osteoarthritis induced by ACL transection". Osteoarthr. Cartil. 17 (4): 441–7. doi:10.1016/j.joca.2008.09.009. PMID 18990590.
- ↑ Grushko G, Schneiderman R, Maroudas A (1989). "Some biochemical and biophysical parameters for the study of the pathogenesis of osteoarthritis: a comparison between the processes of ageing and degeneration in human hip cartilage". Connect. Tissue Res. 19 (2–4): 149–76. doi:10.3109/03008208909043895. PMID 2805680.
- ↑ Mankin HJ, Thrasher AZ (January 1975). "Water content and binding in normal and osteoarthritic human cartilage". J Bone Joint Surg Am 57 (1): 76–80. PMID 1123375.
- 1 2 Venn M, Maroudas A (April 1977). "Chemical composition and swelling of normal and osteoarthrotic femoral head cartilage. I. Chemical composition". Ann. Rheum. Dis. 36 (2): 121–9. doi:10.1136/ard.36.2.121. PMC 1006646. PMID 856064.
- ↑ Madry H, Luyten FP, Facchini A (2012). "Biological aspects of early osteoarthritis". Knee Surg. Sports Traumatol. Arthrosc. 20 (3): 407–22. doi:10.1007/s00167-011-1705-8. PMID 22009557.
- ↑ Englund M, Roemer FW, Hayashi D, Crema MD, Guermazi A (2012). "Meniscus pathology, osteoarthritis and the treatment controversy". Nat. Rev. Rheumatol. 8 (7): 412–9. doi:10.1038/nrrheum.2012.69. PMID 22614907.
- ↑ Li G, Yin J, Gao J, Cheng TS, Pavlos NJ, Zhang C, Zheng MH (2013). "Subchondral bone in osteoarthritis: insight into risk factors and microstructural changes". Arthritis Research & Therapy 15 (6): 223. doi:10.1186/ar4405. PMID 24321104.
- ↑ Hill CL, Gale DG, Chaisson CE, Skinner K, Kazis L, Gale ME, Felson DT (2001). "Knee effusions, popliteal cysts, and synovial thickening: association with knee pain in osteoarthritis". J. Rheumatol. 28 (6): 1330–7. PMID 11409127.
- ↑ Felson DT, Chaisson CE, Hill CL, Totterman SM, Gale ME, Skinner KM, Kazis L, Gale DR (2001). "The association of bone marrow lesions with pain in knee osteoarthritis". Ann Intern Med. 2001 Apr 3;134(7):541-9 134 (7): 541–9. doi:10.7326/0003-4819-134-7-200104030-00007. PMID 11281736.
- ↑ Zhang W, Doherty M, Peat G, Bierma-Zeinstra MA, Arden NK, Bresnihan B, Herrero-Beaumont G, Kirschner S, Leeb BF, Lohmander LS, Mazières B, Pavelka K, Punzi L, So AK, Tuncer T, Watt I, Bijlsma JW (March 2010). "EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis". Ann. Rheum. Dis. 69 (3): 483–9. doi:10.1136/ard.2009.113100. PMID 19762361.
- ↑ Bierma-Zeinstra SM, Oster JD, Bernsen RM, Verhaar JA, Ginai AZ, Bohnen AM (August 2002). "Joint space narrowing and relationship with symptoms and signs in adults consulting for hip pain in primary care". J. Rheumatol. 29 (8): 1713–8. PMID 12180735.
- ↑ Osteoarthritis (OA): Joint Disorders at Merck Manual of Diagnosis and Therapy Professional Edition
- ↑ Phillips CR, Brasington RD (2010). "Osteoarthritis treatment update: Are NSAIDs still in the picture?". Journal of Musculoskeletal Medicine 27 (2).
- ↑ Kalunian KC (2013). "Patient information: Osteoarthritis symptoms and diagnosis (Beyond the Basics)". UpToDate. Retrieved 15 February 2013.
- ↑ Altman R, Alarcón G, Appelrouth D, Bloch D, Borenstein D, Brandt K, Brown C, Cooke TD, Daniel W, Gray R (November 1990). "The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hand". Arthritis Rheum. 33 (11): 1601–10. doi:10.1002/art.1780331101. PMID 2242058.
- ↑ Vasan N, Tao L, Vikas B (2010). First Aid for the USMLE Step 1, 2010 (First Aid USMLE). McGraw-Hill Medical. p. 378. ISBN 0-07-163340-5.
- ↑ Punzi L, Ramonda R, Sfriso P (October 2004). "Erosive osteoarthritis". Best Pract Res Clin Rheumatol 18 (5): 739–58. doi:10.1016/j.berh.2004.05.010. PMID 15454130.
- 1 2 3 4 5 Flood J (March 2010). "The role of acetaminophen in the treatment of osteoarthritis". Am J Manag Care 16 (Suppl Management): S48–54. PMID 20297877.

- 1 2 3 4 Cibulka MT, White DM, Woehrle J, Harris-Hayes M, Enseki K, Fagerson TL, Slover J, Godges JJ (April 2009). "Hip pain and mobility deficits—hip osteoarthritis: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association". J Orthop Sports Phys Ther 39 (4): A1–25. doi:10.2519/jospt.2009.0301. PMID 19352008.
- ↑ Hagen KB, Dagfinrud H, Moe RH, Østerås N, Kjeken I, Grotle M, Smedslund G (2012). "Exercise therapy for bone and muscle health: an overview of systematic reviews". BMC Med 10: 167. doi:10.1186/1741-7015-10-167. PMC 3568719. PMID 23253613.
- ↑ Fransen M, McConnell S, Hernandez-Molina G, Reichenbach S (2014). "Exercise for osteoarthritis of the hip.". Cochrane Database Syst Rev 4 (4): CD007912. doi:10.1002/14651858.CD007912.pub2. PMID 24756895.
- ↑ Juhl C, Christensen R, Roos EM, Zhang W, Lund H (Mar 2014). "Impact of exercise type and dose on pain and disability in knee osteoarthritis: a systematic review and meta-regression analysis of randomized controlled trials.". Arthritis & rheumatology (Hoboken, N.J.) 66 (3): 622–36. doi:10.1002/art.38290. PMID 24574223.
- ↑ Wang SY, Olson-Kellogg B, Shamliyan TA, Choi JY, Ramakrishnan R, Kane RL (November 2012). "Physical therapy interventions for knee pain secondary to osteoarthritis: a systematic review". Annals of Internal Medicine 157 (9): 632–44. doi:10.7326/0003-4819-157-9-201211060-00007. PMID 23128863.
- ↑ De Luigi AJ (May 2012). "Complementary and alternative medicine in osteoarthritis". PM&R 4 (5 Suppl): S122–33. doi:10.1016/j.pmrj.2012.01.012. PMID 22632691.
- ↑ French HP, Brennan A, White B, Cusack T (2011). "Manual therapy for osteoarthritis of the hip or knee — a systematic review". Man Ther 16 (2): 109–117. doi:10.1016/j.math.2010.10.011. PMID 21146444.
- ↑ Sturnieks DL, Tiedemann A, Chapman K, Munro B, Murray SM, Lord SR (November 2004). "Physiological risk factors for falls in older people with lower limb arthritis". J. Rheumatol. 31 (11): 2272–9. PMID 15517643.
- ↑ Penny P, Geere J, Smith TO (October 2013). "A systematic review investigating the efficacy of laterally wedged insoles for medial knee osteoarthritis". Rheumatol. Int. 33 (10): 2529–38. doi:10.1007/s00296-013-2760-x. PMID 23612781.
- ↑ Parkes MJ, Maricar N, Lunt M, LaValley MP, Jones RK, Segal NA, Takahashi-Narita K, Felson DT (August 2013). "Lateral wedge insoles as a conservative treatment for pain in patients with medial knee osteoarthritis: a meta-analysis". JAMA 310 (7): 722–30. doi:10.1001/jama.2013.243229. PMID 23989797.
- 1 2 Duivenvoorden, T; Brouwer, RW; van Raaij, TM; Verhagen, AP; Verhaar, JA; Bierma-Zeinstra, SM (16 March 2015). "Braces and orthoses for treating osteoarthritis of the knee.". The Cochrane database of systematic reviews 3: CD004020. PMID 25773267.
- ↑ Page CJ, Hinman RS, Bennell KL (2011). "Physiotherapy management of knee osteoarthritis". Int J Rheum Dis 14 (2): 145–152. doi:10.1111/j.1756-185X.2011.01612.x. PMID 21518313.
- ↑ "Osteoarthritis Lifestyle and home remedies". Diseases and Conditions. Mayo Clinic.
- 1 2 3 4 Consumer Reports Health Best Buy Drugs (July 2013), "The Nonsteroidal Anti-Inflammatory Drugs: Treating Osteoarthritis and Pain. Comparing effectiveness, safety, and price." (PDF), NSAIDs, Yonkers, New York: Consumer Reports, retrieved 12 February 2014
- 1 2 Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M, Dougados M, Hochberg M, Hunter DJ, Kwoh K, Lohmander LS, Tugwell P (September 2007). "OARSI recommendations for the management of hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidence". Osteoarthr. Cartil. 15 (9): 981–1000. doi:10.1016/j.joca.2007.06.014. PMID 17719803.
- ↑ Machado, GC; Maher, CG; Ferreira, PH; Pinheiro, MB; Lin, CW; Day, RO; McLachlan, AJ; Ferreira, ML (31 March 2015). "Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis of randomised placebo controlled trials.". BMJ (Clinical research ed.) 350: h1225. doi:10.1136/bmj.h1225. PMID 25828856.
- ↑ Chen YF, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, Taylor RS (April 2008). "Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation". Health Technol Assess 12 (11): 1–278, iii. doi:10.3310/hta12110. PMID 18405470.
- ↑ Wielage, RC; Myers, JA; Klein, RW; Happich, M (December 2013). "Cost-effectiveness analyses of osteoarthritis oral therapies: a systematic review.". Applied Health Economics and Health Policy 11 (6): 593–618. doi:10.1007/s40258-013-0061-x. PMID 24214160.
- ↑ McAlindon, TE; Bannuru, RR; Sullivan, MC; Arden, NK; Berenbaum, F; Bierma-Zeinstra, SM; Hawker, GA; Henrotin, Y; Hunter, DJ; Kawaguchi, H; Kwoh, K; Lohmander, S; Rannou, F; Roos, EM; Underwood, M (March 2014). "OARSI guidelines for the non-surgical management of knee osteoarthritis.". Osteoarthritis and cartilage / OARS, Osteoarthritis Research Society 22 (3): 363–88. doi:10.1016/j.joca.2014.01.003. PMID 24462672.
- ↑ Hochberg, MC; Altman, RD; April, KT; Benkhalti, M; Guyatt, G; McGowan, J; Towheed, T; Welch, V; Wells, G; Tugwell, P; American College of, Rheumatology (April 2012). "American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee.". Arthritis care & research 64 (4): 465–74. doi:10.1002/acr.21596. PMID 22563589.
- ↑ da Costa, BR; Nüesch, E; Kasteler, R; Husni, E; Welch, V; Rutjes, AW; Jüni, P (17 September 2014). "Oral or transdermal opioids for osteoarthritis of the knee or hip.". The Cochrane database of systematic reviews 9: CD003115. doi:10.1002/14651858.CD003115.pub4. PMID 25229835.
- ↑ Derry S, Moore RA, Rabbie R (2012). "Topical NSAIDs for chronic musculoskeletal pain in adults". The Cochrane Library 9: CD007400. doi:10.1002/14651858.CD007400.pub2. PMID 22972108.
- ↑ da Costa BR, Nüesch E, Kasteler R, Husni E, Welch V, Rutjes AW, Jüni P (2014). "Oral or transdermal opioids for osteoarthritis of the knee or hip.". The Cochrane database of systematic reviews 9: CD003115. doi:10.1002/14651858.CD003115.pub4. PMID 25229835.
- 1 2 3 4 5 De Silva V, El-Metwally A, Ernst E, Lewith G, Macfarlane GJ (May 2011). "Evidence for the efficacy of complementary and alternative medicines in the management of osteoarthritis: a systematic review". Rheumatology (Oxford) 50 (5): 911–20. doi:10.1093/rheumatology/keq379. PMID 21169345.
- 1 2 3 Cameron M, Gagnier JJ, Little CV, Parsons TJ, Blümle A, Chrubasik S (November 2009). "Evidence of effectiveness of herbal medicinal products in the treatment of arthritis. Part I: Osteoarthritis". Phytother Res 23 (11): 1497–515. doi:10.1002/ptr.3007. PMID 19856319.
- ↑ Altman R, Barkin RL (March 2009). "Topical therapy for osteoarthritis: clinical and pharmacologic perspectives". Postgrad Med 121 (2): 139–47. doi:10.3810/pgm.2009.03.1986. PMID 19332972.
- ↑ Arroll B, Goodyear-Smith F (April 2004). "Corticosteroid injections for osteoarthritis of the knee: meta-analysis". BMJ 328 (7444): 869. doi:10.1136/bmj.38039.573970.7C. PMC 387479. PMID 15039276.
- ↑ Colen, S; van den Bekerom, MP; Mulier, M; Haverkamp, D (1 August 2012). "Hyaluronic acid in the treatment of knee osteoarthritis: a systematic review and meta-analysis with emphasis on the efficacy of different products.". BioDrugs 26 (4): 257–68. doi:10.2165/11632580-000000000-00000. PMID 22734561.
- 1 2 Rutjes AW, Jüni P, da Costa BR, Trelle S, Nüesch E, Reichenbach S (August 2012). "Viscosupplementation for osteoarthritis of the knee: a systematic review and meta-analysis". Annals of Internal Medicine 157 (3): 180–91. doi:10.7326/0003-4819-157-3-201208070-00473. PMID 22868835.
- ↑ Witteveen, AG; Hofstad, CJ; Kerkhoffs, GM (17 October 2015). "Hyaluronic acid and other conservative treatment options for osteoarthritis of the ankle.". The Cochrane database of systematic reviews 10: CD010643. PMID 26475434.
It is unclear if there is a benefit or harm for HA as treatment for ankle OA
- ↑ Khoshbin A, Leroux T, Wasserstein D, Marks P, Theodoropoulos J, Ogilvie-Harris D, Gandhi R, Takhar K, Lum G, Chahal J (December 2013). "The efficacy of platelet-rich plasma in the treatment of symptomatic knee osteoarthritis: a systematic review with quantitative synthesis". Arthroscopy 29 (12): 2037–48. doi:10.1016/j.arthro.2013.09.006. PMID 24286802.
- ↑ Rodriguez-Merchan, EC (September 2013). "Intraarticular Injections of Platelet-rich Plasma (PRP) in the Management of Knee Osteoarthritis". Archives of bone and joint surgery 1 (1): 5–8. PMC 4151401. PMID 25207275.
- ↑ Santaguida PL, Hawker GA, Hudak PL, Glazier R, Mahomed NN, Kreder HJ, Coyte PC, Wright JG (December 2008). "Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: a systematic review". Can J Surg 51 (6): 428–36. PMC 2592576. PMID 19057730.
- ↑ Carr AJ, Robertsson O, Graves S, Price AJ, Arden NK, Judge A, Beard DJ (April 2012). "Knee replacement". Lancet 379 (9823): 1331–40. doi:10.1016/S0140-6736(11)60752-6. PMID 22398175.
- ↑ Jenkins PJ, Clement ND, Hamilton DF, Gaston P, Patton JT, Howie CR (2013). "Predicting the cost-effectiveness of total hip and knee replacement: A health economic analysis". The bone & joint journal 95–B (1): 115–21. doi:10.1302/0301-620X.95B1.29835. PMID 23307684.
- ↑ Daigle ME, Weinstein AM, Katz JN, Losina E (2012). "The cost-effectiveness of total joint arthroplasty: A systematic review of published literature". Best practice & research. Clinical rheumatology 26 (5): 649–58. doi:10.1016/j.berh.2012.07.013. PMC 3879923. PMID 23218429.
- ↑ Hunziker EB, Lippuner K, Keel MJ, Shintani N (2015). "An educational review of cartilage repair: precepts & practice – myths & misconceptions – progress & prospects". Osteoarthritis Cartilage 23 (3): 334–50. doi:10.1016/j.joca.2014.12.011. PMID 25534362.
- ↑ Brouwer, RW; Huizinga, MR; Duivenvoorden, T; van Raaij, TM; Verhagen, AP; Bierma-Zeinstra, SM; Verhaar, JA (13 December 2014). "Osteotomy for treating knee osteoarthritis.". The Cochrane database of systematic reviews 12: CD004019. doi:10.1002/14651858.CD004019.pub4. PMID 25503775.
- ↑ Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM (2014). "A systematic review of recommendations and guidelines for the management of osteoarthritis: The Chronic Osteoarthritis Management Initiative of the U.S. Bone and Joint Initiative". Seminars in arthritis and rheumatism 43 (6): 701–12. doi:10.1016/j.semarthrit.2013.11.012. PMID 24387819.
- ↑ Katz, JN; Brownlee, SA; Jones, MH (February 2014). "The role of arthroscopy in the management of knee osteoarthritis.". Best practice & research. Clinical rheumatology 28 (1): 143–56. doi:10.1016/j.berh.2014.01.008. PMID 24792949.
- ↑ Thorlund, JB.; Juhl, CB.; Roos, EM.; Lohmander, LS. (2015). "Arthroscopic surgery for degenerative knee: systematic review and meta-analysis of benefits and harms". BMJ 350: h2747. doi:10.1136/bmj.h2747. PMC 4469973. PMID 26080045.
- ↑ The effects of Glucosamine Sulphate on OA of the knee joint. BestBets.
- ↑ Burdett N, McNeil JD (Sep 2012). "Difficulties with assessing the benefit of glucosamine sulphate as a treatment for osteoarthritis.". International journal of evidence-based healthcare 10 (3): 222–6. doi:10.1111/j.1744-1609.2012.00279.x. PMID 22925619.
- ↑ Wandel S, Jüni P, Tendal B, Nüesch E, Villiger PM, Welton NJ, Reichenbach S, Trelle S (Sep 16, 2010). "Effects of glucosamine, chondroitin, or placebo in patients with osteoarthritis of hip or knee: network meta-analysis.". BMJ (Clinical research ed.) 341: c4675. doi:10.1136/bmj.c4675. PMC 2941572. PMID 20847017.
- ↑ Wu D, Huang Y, Gu Y, Fan W (Jun 2013). "Efficacies of different preparations of glucosamine for the treatment of osteoarthritis: a meta-analysis of randomised, double-blind, placebo-controlled trials.". International journal of clinical practice 67 (6): 585–94. doi:10.1111/ijcp.12115. PMID 23679910.
- ↑ Chou R, McDonagh MS, Nakamoto E, Griffin J (Oct 2011). "Analgesics for Osteoarthritis: An Update of the 2006 Comparative Effectiveness Review". PMID 22091473.
- ↑ Miller KL, Clegg DO (February 2011). "Glucosamine and chondroitin sulfate". Rheum. Dis. Clin. North Am. 37 (1): 103–18. doi:10.1016/j.rdc.2010.11.007. PMID 21220090.
The best current evidence suggests that the effect of these supplements, alone or in combination, on OA pain, function, and radiographic change is marginal at best.
- ↑ Rovati LC, Girolami F, Persiani S (Jun 2012). "Crystalline glucosamine sulfate in the management of knee osteoarthritis: efficacy, safety, and pharmacokinetic properties.". Therapeutic advances in musculoskeletal disease 4 (3): 167–80. doi:10.1177/1759720X12437753. PMC 3400104. PMID 22850875.
- ↑ Gregory, PJ; Fellner, C (June 2014). "Dietary supplements as disease-modifying treatments in osteoarthritis: a critical appraisal.". P & T : a peer-reviewed journal for formulary management 39 (6): 436–52. PMID 25050057.
- ↑ Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, Bierma-Zeinstra S, Brandt KD, Croft P, Doherty M, Dougados M, Hochberg M, Hunter DJ, Kwoh K, Lohmander LS, Tugwell P (February 2008). "OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines" (PDF). Osteoarthr. Cartil. 16 (2): 137–62. doi:10.1016/j.joca.2007.12.013. PMID 18279766. Archived from the original (PDF) on July 21, 2011.
- 1 2 Henrotin Y, Mobasheri A, Marty M (Jan 30, 2012). "Is there any scientific evidence for the use of glucosamine in the management of human osteoarthritis?". Arthritis Research & Therapy 14 (1): 201. doi:10.1186/ar3657. PMC 3392795. PMID 22293240.
- ↑ Lopez HL (May 2012). "Nutritional interventions to prevent and treat osteoarthritis. Part II: focus on micronutrients and supportive nutraceuticals". PM&R 4 (5 Suppl): S155–68. doi:10.1016/j.pmrj.2012.02.023. PMID 22632695.
- 1 2 Rosenbaum CC, O'Mathúna DP, Chavez M, Shields K (2010). "Antioxidants and antiinflammatory dietary supplements for osteoarthritis and rheumatoid arthritis". Altern Ther Health Med 16 (2): 32–40. PMID 20232616.
- ↑ Pirotta M (September 2010). "Arthritis disease - the use of complementary therapies". Aust Fam Physician 39 (9): 638–40. PMID 20877766.
- ↑ Cameron M, Chrubasik S (May 22, 2014). "Oral herbal therapies for treating osteoarthritis". The Cochrane database of systematic reviews 5: CD002947. doi:10.1002/14651858.cd002947.pub2. PMC 4494689. PMID 24848732.
Several other medicinal plant products, including extracts of Boswellia serrata, show trends of benefits that warrant further investigation in light of the fact that the risk of adverse events appear low.
- ↑ Manheimer E, Cheng K, Linde K, Lao L, Yoo J, Wieland S, van der Windt DA, Berman BM, Bouter LM (2010). Manheimer, Eric, ed. "Acupuncture for peripheral joint osteoarthritis". Cochrane Database of Systematic Reviews (1): CD001977. doi:10.1002/14651858.CD001977.pub2. PMC 3169099. PMID 20091527.
- ↑ Wang SM, Kain ZN, White PF (February 2008). "Acupuncture analgesia: II. Clinical considerations" (PDF). Anesth. Analg. 106 (2): 611–21, table of contents. doi:10.1213/ane.0b013e318160644d. PMID 18227323.
- ↑ Rutjes AW, Nüesch E, Sterchi R, Kalichman L, Hendriks E, Osiri M, Brosseau L, Reichenbach S, Jüni P (2009). Rutjes, Anne WS, ed. "Transcutaneous electrostimulation for osteoarthritis of the knee". Cochrane Database of Systematic Reviews (4): CD002823. doi:10.1002/14651858.CD002823.pub2. PMID 19821296.
- ↑ Brosseau, L; Welch, V; Wells, G; DeBie, R; Gam, A; Harman, K; Morin, M; Shea, B; Tugwell, P (2004). "Low level laser therapy (Classes I, II and III) for treating osteoarthritis.". The Cochrane database of systematic reviews (3): CD002046. doi:10.1002/14651858.CD002046.pub2. PMID 15266461.
- ↑ Bjordal, J; Johnson, M; Lopes-Martins, R; Bogen, B; Chow, R; Ljunggren, A (2007). "Short-term efficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials.". BMC Musculoskeletal Disorders 8 (8): 51. doi:10.1186/1471-2474-8-51.
- ↑ "WHO Disease and injury country estimates". World Health Organization. 2009. Retrieved Nov 11, 2009.
- ↑ Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. (December 2012). "Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010". Lancet 380 (9859): 2163–96. doi:10.1016/S0140-6736(12)61729-2. PMID 23245607.
- ↑ Green GA (2001). "Understanding NSAIDs: from aspirin to COX-2". Clin Cornerstone 3 (5): 50–60. doi:10.1016/S1098-3597(01)90069-9. PMID 11464731.
- ↑ "Table 9: Estimated prevalence of moderate and severe disability (millions) for leading disabling conditions by age, for high-income and low- and middle-income countries, 2004". The Global Burden of Disease: 2004 Update. Geneva: World Health Organization. 2008. p. 35. ISBN 978-92-4-156371-0.
- ↑ Pfuntner A., Wier L.M., Stocks C. Most Frequent Conditions in U.S. Hospitals, 2011. HCUP Statistical Brief #162. September 2013. Agency for Healthcare Research and Quality, Rockville, Maryland.
- ↑ Torio CM, Andrews RM (August 2013). "National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011.". HCUP Statistical Brief #160. Rockville, Maryland: Agency for Healthcare Research and Quality.
- ↑ Pfuntner, A; Wier, L. M.; Steiner, C (December 2013). "Costs for Hospital Stays in the United States, 2011: Statistical Brief #168". PMID 24455786.
- ↑ Molnar, R. E. (2001). "Therapod Paleopathology: A Literature Survey". In Tanke, Darren H.; Carpenter, Kenneth; Skrepnick, Michael William. Mesozoic Vertebrate Life. Indiana University Press. pp. 337–63. ISBN 978-0-253-33907-2.
- ↑ Devaraj TL (2011). "Chapter 41: Nature cure yoga for osteoarthritis". Nature Cure for Common Diseases. New Delhi: Arya Publication. p. 368. ISBN 978-8189093747.
- ↑ Civjan N (2012). Chemical Biology: Approaches to Drug Discovery and Development to Targeting Disease. John Wiley & Sons. p. 313. ISBN 9781118437674.
- ↑ Bruyère O, Burlet N, Delmas PD, Rizzoli R, Cooper C, Reginster JY (2008). "Evaluation of symptomatic slow-acting drugs in osteoarthritis using the GRADE system". BMC Musculoskelet Disord 9: 165. doi:10.1186/1471-2474-9-165. PMC 2627841. PMID 19087296.
- ↑ Chu, CR; Andriacchi, TP (2015). "Dance between biology, mechanics, and structure: a systems-based approach to developing osteoarthritis prevention strategies". J Orthop Res 33 (7): 939–947. doi:10.1002/jor.22817. PMID 25639920.
- ↑ T. Pap, J. Schedel, G. Pap, U. Moller-Ladner, R.E. Gay, S. Gay C. Guincamp (2000). "Gene therapy in osteoarthritis". Joint Bone Spine.
- ↑ Kraus, VB; Blanco, FJ; Englund, M; Henrotin, Y; Lohmander, LS; Losina, E; Onnerfjord, P; Persiani, S (2015). "OARSI Clinical Trials Recommendations: Soluble biomarker assessments in clinical trials in osteoarthritis". Osteoarthritis Cartilage 23 (5): 686–697. doi:10.1016/j.joca.2015.03.002. PMC 4430113. PMID 25952342.
- ↑ Saberi Hosnijeh, F; Runhaar, J; van Meurs, JB; Bierma-Zeinstra, SM (2015). "Biomarkers for osteoarthritis: Can they be used for risk assessment? A systematic review". Maturitas 82 (1): 36–49. doi:10.1016/j.maturitas.2015.04.004. PMID 25963100.
- ↑ Nepple, JJ; Thomason, KM; An, TW; Harris-Hayes, M; Clohisy, JC (2015). "What is the utility of biomarkers for assessing the pathophysiology of hip osteoarthritis? A systematic review". Clin Orthop Relat Res 473 (5): 1683–1701. doi:10.1007/s11999-015-4148-6. PMID 25623593.
- ↑ Kumahashi, N; Swärd, P; Larsson, S; Lohmander, LS; Frobell, R; Struglics, A (2015). "Type II collagen C2C epitope in human synovial fluid and serum after knee injury - associations with molecular and structural markers of injury". Osteoarthritis Cartilage 23 (9): 1506–12. doi:10.1016/j.joca.2015.04.022. PMID 25937025.
External links
| Wikimedia Commons has media related to Osteoarthritis. |
- American College of Rheumatology Factsheet on OA
- Osteoarthritis The Arthritis Foundation
- National Institute of Arthritis and Musculoskeletal and Skin Diseases - US National Institute of Arthritis and Musculoskeletal and Skin Diseases
| ||||||||||||||||||||||
|