Vitamin B12
 | |
| Systematic (IUPAC) name | |
|---|---|
| α-(5,6-dimethylbenzimidazolyl)cobamidcyanide | |
| Clinical data | |
| AHFS/Drugs.com | monograph |
| |
| oral, IV, IM, intranasal | |
| Pharmacokinetic data | |
| Bioavailability | Readily absorbed in distal half of the ileum |
| Protein binding |
Very high to specific transcobalamins plasma proteins Binding of hydroxocobalamin is slightly higher than cyanocobalamin. |
| Metabolism | hepatic |
| Half-life |
Approximately 6 days (400 days in the liver) |
| Excretion | Renal |
| Identifiers | |
|
68-19-9 | |
| B03BA01 | |
| PubChem | CID 5479203 |
| DrugBank |
DB00115 |
| ChemSpider |
10469504 |
| KEGG |
D00166 |
| ChEMBL |
CHEMBL2110563 |
| Chemical data | |
| Formula | C63H88CoN14O14P |
| 1355.37 g/mol | |
|
SMILES
| |
| |
| | |

Vitamin B12, vitamin B12 or vitamin B-12, also called cobalamin, is a water-soluble vitamin with a key role in the normal functioning of the brain and nervous system, and for the formation of blood. It is one of the eight B vitamins. It is normally involved in the metabolism of every cell of the human body, especially affecting DNA synthesis and regulation, but also fatty acid metabolism and amino acid metabolism.[1] Neither fungi, plants, nor animals are capable of producing vitamin B12. Only bacteria and archaea have the enzymes required for its synthesis, although many foods are a natural source of B12 because of bacterial symbiosis. The vitamin is the largest and most structurally complicated vitamin and can be produced industrially only through bacterial fermentation-synthesis.
Vitamin B12 consists of a class of chemically related compounds (vitamers), all of which have vitamin activity. It contains the biochemically rare element cobalt sitting in the center of a planar tetra-pyrrole ring called a Corrin ring. Biosynthesis of the basic structure of the vitamin is accomplished only by bacteria and archaea (which usually produce hydroxocobalamin), but conversion between different forms of the vitamin can be accomplished in the human body. A common semi-synthetic form of the vitamin is cyanocobalamin, which does not occur in nature but is produced from bacterial hydroxocobalamin. Because of its stability and lower production cost, this form is then used in many pharmaceuticals and supplements as well as a food additive. In the body it is converted to the human physiological forms methylcobalamin and 5'-deoxyadenosylcobalamin, leaving behind the cyanide ion, albeit in a minimal concentration. More recently, hydroxocobalamin, methylcobalamin, and adenosylcobalamin can be found in more expensive pharmacological products and food supplements. Their extra utility is currently debated.
Vitamin B12 was discovered from its relationship to disease pernicious anemia, which is an autoimmune disease in which parietal cells of the stomach responsible for secreting intrinsic factor are destroyed (these cells are also responsible for secreting acid in the stomach). Because intrinsic factor is crucial for the normal absorption of B12, its lack in pernicious anemia causes a vitamin B12 deficiency. Many other subtler kinds of vitamin B12 deficiency and their biochemical effects have since been elucidated.[2]
Terminology
The names vitamin B12, vitamin B12, or vitamin B-12, and the alternative name cobalamin, generally refer to all forms of the vitamin. Some medical practitioners have suggested that its use be split into two categories.
- In a broad sense, B12 refers to a group of cobalt-containing vitamer compounds known as cobalamins: these include cyanocobalamin (an artifact formed from using activated charcoal, which always contains trace cyanide, to purify hydroxycobalamin), hydroxocobalamin (another medicinal form, produced by bacteria), and finally, the two naturally occurring cofactor forms of B12 in the human body: 5'-deoxyadenosylcobalamin (adenosylcobalamin—AdoB12), the cofactor of Methylmalonyl Coenzyme A mutase (MUT), and methylcobalamin (MeB12), the cofactor of enzyme Methionine synthase, which is responsible for conversion of homocysteine to methionine and of 5-methyltetrahydrofolate to tetrahydrofolate.
- The term B12 may be properly used to refer to cyanocobalamin, the principal B12 form used for foods and in nutritional supplements. This ordinarily creates no problem, except perhaps in rare cases of eye nerve damage, where the body is only marginally able to use this form due to high cyanide levels in the blood due to cigarette smoking; it thus requires cessation of smoking or B12 given in another form, for the optic symptoms to abate. However, tobacco amblyopia is a rare condition, and it is yet unclear whether it represents a peculiar B12 deficiency that is resistant to treatment with cyanocobalamin.
Finally, so-called pseudovitamin-B12 refers to B12-like analogues that are biologically inactive in humans and yet found to be present alongside B12 in humans,[3][4] many food sources (including animals[5]), and possibly supplements and fortified foods.[6][7] In most cyanobacteria, including Spirulina, and some algae, such as dried Asakusa-nori (Porphyra tenera), pseudovitamin-B12 is found to predominate.[8][9]
Medical uses
Vitamin B12 is used to treat vitamin B12 deficiency, cyanide poisoning, and hereditary deficiency of transcobalamin II.[10] It is given as part of the Schilling test for detecting pernicious anemia.[10]
For cyanide poisoning, a large amount of hydroxocobalamin may be given intravenously and sometimes in combination with sodium thiosulfate.[11] The mechanism of action is straightforward: the hydroxycobalamin hydroxide ligand is displaced by the toxic cyanide ion, and the resulting harmless B12 complex is excreted in urine. In the United States, the Food and Drug Administration approved (in 2006) the use of hydroxocobalamin for acute treatment of cyanide poisoning.[12]
High vitamin B12 level in elderly individuals may protect against brain atrophy or shrinkage associated with Alzheimer's disease and impaired cognitive function.[13]
High-dose administration of Vitamin B12 has been additionally validated to stimulate the activity of the body's TH1 suppressor T-Cells, which then down-regulates the over-production of the allergen antibody IgE in allergic individuals.[14]
Recommended intake
The dietary reference intake for an adult ranges from 2 to 3 µg per day (US),[15] and 1.5 µg per day (UK).[16] But according to a new study,[17] the DRI should be 4 to 7 µg per day. The Center for Food Safety and Applied Nutrition recommends 6 µg per day, based on a caloric intake of 2,000 calories, for adults and children four or more years of age.[18]
Vitamin B12 is believed to be safe when used orally in amounts that do not exceed the recommended dietary allowance (RDA). There have been studies that showed no adverse consequences of doses above the RDA.[19] The RDA for vitamin B12 in pregnant women is 2.6 µg per day and 2.8 µg during lactation periods.[20] There is insufficient reliable information available about the safety of consuming greater amounts of vitamin B12 during pregnancy.
The Institute of Medicine states that because 10 to 30% of older people may be unable to absorb naturally occurring vitamin B12 in foods, it is advisable for those 51 years old and older to consume B12-fortified foods or B12 supplements to meet the recommended intake.[21]
Controversial sources in algae
The UK Vegan Society, the Vegetarian Resource Group, and the Physicians Committee for Responsible Medicine, among others, recommend that vegans either consistently eat B12-fortified foods or take a daily or weekly B12 supplement to meet the recommended intake.[22][23][24]
It is important for vegans, whose food provides few sources of B12, and anyone else wishing to obtain B12 from food sources other than animals, to consume foods that contain little or no pseudovitamin-B12 and are high in biologically active B12. However, there have been no significant human trials of sufficient size to demonstrate enzymatic activity of B12 from nonbacterial sources, such as Chlorella and edible sea algae (seaweeds, such as lavers), although chemically some of these sources have been reported to contain B12 that seems chemically similar to active vitamin.[25][26] However, among these sources, only fresh sea algae such as Susabi-nori (Porphyra yezoensis)[27][28] have been reported to demonstrate vitamin B12 activity in B12 deficient rats. This has yet to be demonstrated for Chlorella, and no study in rats of any algal B12 source has yet to be confirmed by a second independent study. The possibility of algae-derived active forms of B12 presently remains an active topic of research, with no results that have yet reached consensus in the nutritional community.
Deficiency
Vitamin B12 deficiency can potentially cause severe and irreversible damage, especially to the brain and nervous system. At levels only slightly lower than normal, a range of symptoms such as fatigue, depression, and poor memory may be experienced.[2]
Vitamin B12 deficiency can also cause symptoms of mania and psychosis.[29][30] Vitamin B12 deficiency is most commonly caused by low intakes, but can also result from mal-absorption, certain intestinal disorders, low presence of binding proteins, and using of certain medications. Vitamin B12 is rare from plant sources, so vegetarians will be the vulnerable populations most likely to suffer from vitamin B12 deficiency. Infants are at a higher risk of vitamin B12 deficiency if they were born to vegetarian mothers. The elderly who have diets with limited meat or animal products are vulnerable populations as well.[31] Vitamin B12 deficiency can manifest itself as anemia and in some cases cause permanent neurological damage. Recent studies showed depression is associated with vitamin B12 deficiency; sufficient vitamin B12 level was independently associated with a decreased risk of depression and better cognitive performance adjusted for confounders. Vitamin B12 is a co-substrate of various cell reactions involved in methylation synthesis of nucleic acid and neurotransmitters. Synthesis of the trimonoamine neurotransmitters can enhance the effects of a traditional antidepressant.[32] The intracellular concentrations of vitamin B12 can be inferred through the total plasma concentration of homocysteine, which can be converted to methionine through an enzymatic reaction that uses 5-methyletetrahydrofolate as the methyl donor group. Consequently, the plasma concentration of homocysteine falls as the intracellular concentration of vitamin B12 rises. The active metabolite of vitamin B12 is required for the methylation of homocysteine in the production of methionine, which is involved in a number of biochemical processes including the monoamine neurotransmitters. Thus, a deficiency in vitamin B12 may impact the production and function of those neurotransmitters.[33]
Imerslund-Gräsbeck syndrome is a rare disease where there is selective malabsorption of cobalamine with proteinuria caused due to defect in ileal receptor.
Sources
Foods
Ultimately, animals must obtain vitamin B12 directly or indirectly from bacteria, and these bacteria may inhabit a section of the gut that is distal to the section where B12 is absorbed. Thus, herbivorous animals must either obtain B12 from bacteria in their rumens or (if fermenting plant material in the hindgut) by reingestion of cecotrope feces.
Vitamin B12 is found in most animal derived foods, including fish and shellfish, meat (especially liver), poultry, eggs, milk, and milk products.[2] However, the binding capacity of egg yolks and egg whites is markedly diminished after heat treatment.[34] An NIH Fact Sheet lists a variety of animal food sources of B12.[2]
Besides certain fermented foods,[35][36] there are currently only a few non-animal food sources of biologically active B12 suggested, and none of these have been subjected to human trials.
A Japanese fermented black tea known as Batabata-cha has been found to contain biologically active B12.[37] Unlike kombucha, which is made by fermenting already prepared tea, Batabata-cha is fermented while still in the tea leaf state.
Chlorella,[25][26][38] a fresh-water single cell green algae, has been suggested as a vitamin B12 source but not proven by any live animal assay. Algae are thought to acquire B12 through a symbiotic relationship with heterotrophic bacteria, in which the bacteria supply B12 in exchange for fixed carbon.[39][40] Spirulina and dried Asakusa-nori (Porphyra tenera) have been found to contain mostly pseudovitamin-B12 (see Terminology) instead of biologically active B12.[8][9] While Asakusa-nori (Porphyra tenera) contains mostly pseudovitamin-B12 in the dry state, it has been reported to contain mostly biologically active B12 in the fresh state,[9] but even its fresh state vitamin activity has not been verified by animal enzyme assay.
One group of researchers has reported that the purple laver seaweed known as Susabi-nori (Pyropia yezoensis).[27][28] in its fresh state contains B12 activity in the rat model, which implies that source would be active in humans. These results have not been confirmed.
A single commensal bacteria present in the gut of many mammals has demonstrated an ability to perform all steps necessary to synthesize B12 from common metabolically available products.[41]
Foods fortified with B12 are also sources of the vitamin, although they cannot be regarded as true food sources of B12 since the vitamin is added in supplement form, from commercial bacterial production sources, such as cyanocobalamin. Examples of B12-fortified foods include fortified breakfast cereals, fortified soy products, fortified energy bars, and fortified nutritional yeast. The UK Vegan Society, the Vegetarian Resource Group, and the Physicians Committee for Responsible Medicine, among others, recommend that every vegan who is not consuming B12 foods fortify with supplements.[42][23][24] Not all of these may contain labeled amounts of vitamin activity. Supplemental B12 added to beverages in one study was found to degrade to contain varying levels of pseudovitamin-B12. One report has found B12 analogues present in varying amounts in some multivitamins.[6][7]
Unconventional natural sources of B12 also exist, but their utility as food sources of B12 are doubtful. For example, plants pulled from the ground and not washed may contain remnants of B12 from the bacteria present in the surrounding soil.[43] B12 is also found in lakes if the water has not been sanitized.[44] Certain insects such as termites contain B12 produced by their gut bacteria, in a way analogous to ruminant animals.[45] The human intestinal tract itself may contain B12-producing bacteria in the small intestine,[46] but it is unclear whether sufficient amounts of the vitamin could be produced to meet nutritional needs.
Supplements

Vitamin B12 is provided as a supplement in many processed foods, and is also available in vitamin pill form, including multi-vitamins. Vitamin B12 can be supplemented in healthy subjects also by liquid, transdermal patch, nasal spray, or injection and is available singly or in combination with other supplements. It is a common ingredient in energy drinks and energy shots, usually at many times the minimum recommended daily allowance of B12. Vitamin B12 supplements are effective for preventing deficiencies, especially in vegetarians, and are often marketed as weight loss supplements. However, no scientific studies have shown that B12 is effective for weight loss.
Cyanocobalamin is converted to its active forms, first hydroxocobalamin and then methylcobalamin and adenosylcobalamin in the liver.
The sublingual route, in which B12 is presumably or supposedly taken in more directly under the tongue, has not proven to be necessary or helpful, even though a number of lozenges, pills, and even a lollipop designed for sublingual absorption, are being marketed. A 2003 study found no significant difference in absorption for serum levels from oral vs. sublingual delivery of 0.5 mg of cobalamin.[47] Sublingual methods of replacement are effective only because of the typically high doses (0.5 mg), which are swallowed, not because of placement of the tablet. As noted below, such very high doses of oral B12 may be effective as treatments, even if gastro-intestinal tract absorption is impaired by gastric atrophy (pernicious anemia).
Injection and patches are sometimes used if digestive absorption is impaired, but there is evidence that this course of action may not be necessary with modern high potency oral supplements (such as 0.5 to 1 mg or more). Even pernicious anemia can be treated entirely by the oral route.[48][49][50] These supplements carry such large doses of the vitamin that 1% to 5% of high oral doses of free crystalline B12 is absorbed along the entire intestine by passive diffusion.
However, if the patient has inborn errors in the methyltransfer pathway (cobalamin C disease, combined methylmalonic aciduria and homocystinuria), treatment with intravenous, intramuscular hydroxocobalamin or transdermal B12 is needed.[51][52][53][54][55]
Non-cyano forms as supplements
Recently sublingual methylcobalamin has become available in 5 mg tablets. The metabolic fate and biological distribution of methylcobalamin are expected to be similar to that of other sources of vitamin B12 in the diet.[56] No cyanide is released with methylcobalamin, although the amount of cyanide (2% of the weight, or 20 micrograms cyanide in a 1 mg cyanocobalamin tab) is far less than ingested in many natural foods. Although the safety of cyanocobalamin has long been proven, the safety of the other types is also well established.[57]
Adverse effects
- Hematologic:Peripheral vascular thrombosis has been reported. Treatment of vitamin B12 deficiency can unmask polycythemia vera, which is characterized by an increase in blood volume and the number of red blood cells. The correction of megaloblastic anemia with vitamin B12 can result in fatal hypokalemia and gout in susceptible individuals, and it can obscure folate deficiency in megaloblastic anemia.
- Leber's disease: Vitamin B12 in the form of cyanocobalamin is contraindicated in early Leber's disease, which is hereditary optic nerve atrophy. Cyanocobalamin can cause severe and swift optic atrophy, but other forms of vitamin B12 are available. However, the sources of this statement are not clear, while an opposing view[58] concludes: "The clinical picture of optic neuropathy associated with vitamin B12 deficiency shows similarity to that of Leber's disease optic neuropathy. Both involve the nerve fibers of the papillomacular bundle. The present case reports suggest that optic neuropathy in patients carrying a primary LHON mtDNA mutation may be precipitated by vitamin B12 deficiency. Therefore, known carriers should take care to have an adequate dietary intake of vitamin B12 and malabsorption syndromes like those occurring in familial pernicious anaemia or after gastric surgery should be excluded."
Allergies
Vitamin B12 supplements in theory should be avoided in people sensitive or allergic to cobalamin, cobalt, or any other product ingredients. However, direct allergy to a vitamin or nutrient is extremely rare, and if reported, other causes should be sought.
Interactions
- Alcohol (ethanol): Excessive alcohol intake lasting longer than two weeks can decrease vitamin B12 absorption from the gastrointestinal tract.
- Aminosalicylic acid (para-aminosalicylic acid, PAS, Paser): Aminosalicylic acid can reduce oral vitamin B12 absorption, possibly by as much as 55%, as part of a general malabsorption syndrome. Megaloblastic changes, and occasional cases of symptomatic anemia have occurred, usually after doses of 8 to 12 g/day for several months. Vitamin B12 levels should be monitored in people taking aminosalicylic acid for more than one month.
- Antibiotics: An increased bacterial load can bind significant amounts of vitamin B12 in the gut, preventing its absorption. In people with bacterial overgrowth of the small bowel, antibiotics such as metronidazole (Flagyl) can actually improve vitamin B12 status. The effects of most antibiotics on gastrointestinal bacteria are unlikely to have clinically significant effects on vitamin B12 levels.
- Hormonal contraception: The data regarding the effects of oral contraceptives on vitamin B12 serum levels are conflicting. Some studies have found reduced serum levels in oral contraceptive users, but others have found no effect despite use of oral contraceptives for up to 6 months. When oral contraceptive use is stopped, normalization of vitamin B12 levels usually occurs. Lower vitamin B12 serum levels seen with oral contraceptives probably are not clinically significant.
- Chloramphenicol (Chloromycetin): Limited case reports suggest that chloramphenicol can delay or interrupt the reticulocyte response to supplemental vitamin B12 in some patients. Blood counts should be monitored closely if this combination cannot be avoided.
- Cobalt irradiation: Cobalt irradiation of the small bowel can decrease gastrointestinal (GI) absorption of vitamin B12.
- Colchicine: Colchicine in doses of 1.9 to 3.9 mg/day can disrupt normal intestinal mucosal function, leading to malabsorption of several nutrients, including vitamin B12. Lower doses do not seem to have a significant effect on vitamin B12 absorption after 3 years of colchicine therapy. The significance of this interaction is unclear. Vitamin B12 levels should be monitored in people taking large doses of colchicine for prolonged periods.
- Colestipol (Colestid), cholestyramine (Questran): These resins used for sequestering bile acids to decrease cholesterol, can decrease gastrointestinal (GI) absorption of vitamin B12. It is unlikely this interaction will deplete body stores of vitamin B12 unless there are other factors contributing to deficiency. In a group of children treated with cholestyramine for up to 2.5 years, there was not any change in serum vitamin B12 levels. Routine supplements are not necessary.
- H2-receptor antagonists: include cimetidine (Tagamet), famotidine (Pepcid), nizatidine (Axid), and ranitidine (Zantac). Reduced secretion of gastric acid and pepsin produced by H2 blockers can reduce absorption of protein-bound (dietary) vitamin B12, but not of supplemental vitamin B12. Gastric acid is needed to release vitamin B12 from protein for absorption. Clinically significant vitamin B12 deficiency and megaloblastic anemia are unlikely, unless H2 blocker therapy is prolonged (2 years or more), or the person's diet is poor. It is also more likely if the person is rendered achlorhydric(with complete absence of gastric acid secretion), which occurs more frequently with proton pump inhibitors than H2 blockers. Vitamin B12 levels should be monitored in people taking high doses of H2 blockers for prolonged periods.
- Metformin (Glucophage): Metformin may reduce serum folic acid and vitamin B12 levels. Long-term use of metformin substantially increases the risk of B12 deficiency and (in those patients who become deficient) hyperhomocysteinemia, which is "an independent risk factor for cardiovascular disease, especially among individuals with type 2 diabetes."[59] There are also rare reports of megaloblastic anemia in people who have taken metformin for five years or more. Reduced serum levels of vitamin B12 occur in up to 30% of people taking metformin chronically.[60][61] However, clinically significant deficiency is not likely to develop if dietary intake of vitamin B12 is adequate. Deficiency can be corrected with vitamin B12 supplements even if metformin is continued. The metformin-induced malabsorption of vitamin B12 is reversible by oral calcium supplementation.[62] The general clinical significance of metformin upon B12 levels is as yet unknown.[63]
- Neomycin: Absorption of vitamin B12 can be reduced by neomycin, but prolonged use of large doses is needed to induce pernicious anemia. Supplements are not usually needed with normal doses.
- Nicotine: Nicotine can reduce serum vitamin B12 levels. The need for vitamin B12 supplementation in smokers has not been adequately studied.
- Nitrous oxide: Nitrous oxide inactivates the cobalamin form of vitamin B12 by oxidation. Symptoms of vitamin B12 deficiency, including sensory neuropathy, myelopathy, and encephalopathy, can occur within days or weeks of exposure to nitrous oxide anesthesia in people with subclinical vitamin B12 deficiency. Symptoms are treated with high doses of vitamin B12, but recovery can be slow and incomplete. People with normal vitamin B12 levels have sufficient vitamin B12 stores to make the effects of nitrous oxide insignificant, unless exposure is repeated and prolonged (such as recreational use). Vitamin B12 levels should be checked in people with risk factors for vitamin B12 deficiency prior to using nitrous oxide anesthesia. Chronic nitrous oxide B12 poisoning (usually from use of nitrous oxide as a recreational drug), however, may result in B12 functional deficiency even with normal measured blood levels of B12.[64]
- Phenytoin (Dilantin), phenobarbital, primidone (Mysoline): These anticonvulsants have been associated with reduced vitamin B12 absorption, and reduced serum and cerebrospinal fluidlevels in some patients. This may contribute to the megaloblastic anemia, primarily caused by folate deficiency, associated with these drugs. It is also suggested that reduced vitamin B12 levels may contribute to the neuropsychiatric side effects of these drugs. Patients should be encouraged to maintain adequate dietary vitamin B12 intake. Folate and vitamin B12 status should be checked if symptoms of anemia develop.
- Proton pump inhibitors (PPIs): The PPIs include omeprazole (Prilosec, Losec), lansoprazole (Prevacid), rabeprazole (Aciphex), pantoprazole (Protonix, Pantoloc), and esomeprazole (Nexium). The reduced secretion of gastric acid and pepsin produced by PPIs can reduce absorption of protein-bound (dietary) vitamin B12, but not supplemental vitamin B12. Gastric acid is needed to release vitamin B12 from protein for absorption. Reduced vitamin B12 levels may be more common with PPIs than with H2-blockers, because they are more likely to produce achlorhydria (complete absence of gastric acid secretion). However, clinically significant vitamin B12 deficiency is unlikely, unless PPI therapy is prolonged (2 years or more) or dietary vitamin intake is low. Vitamin B12 levels should be monitored in people taking high doses of PPIs for prolonged periods.
- Zidovudine (AZT, Combivir, Retrovir): Reduced serum vitamin B12 levels may occur when zidovudine therapy is started. This adds to other factors that cause low vitamin B12 levels in people with HIV, and might contribute to the hematological toxicity associated with zidovudine. However, the data suggest vitamin B12 supplements are not helpful for people taking zidovudine.
- Folic acid: Folic acid, particularly in large doses, can mask vitamin B12 deficiency by completely correcting hematological abnormalities. In vitamin B12 deficiency, folic acid can produce complete resolution of the characteristic megaloblastic anemia, while allowing potentially irreversible neurological damage (from continued inactivity of methylmalonyl mutase) to progress. Thus, vitamin B12 status should be determined before folic acid is given as monotherapy.[65]
- Potassium: Potassium supplements can reduce absorption of vitamin B12 in some people. This effect has been reported with potassium chloride and, to a lesser extent, with potassium citrate. Potassium might contribute to vitamin B12 deficiency in some people with other risk factors, but routine supplements are not necessary.[66]
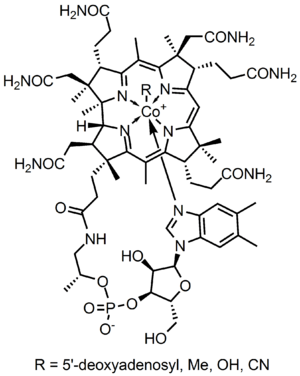
Structure
B12 is the most chemically complex of all the vitamins. The structure of B12 is based on a corrin ring, which is similar to the porphyrin ring found in heme, chlorophyll, and cytochrome. The central metal ion is cobalt. Four of the six coordination sites are provided by the corrin ring, and a fifth by a dimethylbenzimidazole group. The sixth coordination site, the center of reactivity, is variable, being a cyano group (-CN), a hydroxyl group (-OH), a methyl group (-CH3) or a 5'-deoxyadenosyl group (here the C5' atom of the deoxyribose forms the covalent bond with Co), respectively, to yield the four B12 forms mentioned below. Historically, the covalent C-Co bond is one of first examples of carbon-metal bonds to be discovered in biology. The hydrogenases and, by necessity, enzymes associated with cobalt utilization, involve metal-carbon bonds.[67]
Vitamin B12 is a generic descriptor name referring to a collection of cobalt and corrin ring molecules which are defined by their particular vitamin function in the body. All of the substrate cobalt-corrin molecules from which B12 is made, must be synthesized by bacteria. However, after this synthesis is complete, except in rare cases, the human body has the ability to convert any form of B12 to an active form, by means of enzymatically removing certain prosthetic chemical groups from the cobalt atom, and replacing them with others.
The four forms (vitamers) of B12 are all deeply red colored crystals and water solutions, due to the color of the cobalt-corrin complex.
Cyanocobalamin is one such form, i.e. "vitamer", of B12 because it can be metabolized in the body to an active co-enzyme form. However, the cyanocobalamin form of B12 does not occur in nature normally, but is a byproduct of the fact that other forms of B12 are avid binders of cyanide (-CN) which they pick up in the process of activated charcoal purification of the vitamin after it is made by bacteria in the commercial process. Since the cyanocobalamin form of B12 is easy to crystallize and is not sensitive to air-oxidation, it is typically used as a form of B12 for food additives and in many common multivitamins. Pure cyanocobalamin possesses the deep pink color associated with most octahedral cobalt(II) complexes and the crystals are well formed and easily grown up to millimeter size.
Hydroxocobalamin is another form of B12 commonly encountered in pharmacology, but which is not normally present in the human body. Hydroxocobalamin is sometimes denoted B12a. This form of B12 is the form produced by bacteria, and is what is converted to cyanocobalmin in the commercial charcoal filtration step of production. Hydroxocobalamin has an avid affinity for cyanide ion and has been used as an antidote to cyanide poisoning. It is supplied typically in water solution for injection. Hydroxocobalamin is thought to be converted to the active enzymic forms of B12 more easily than cyanocobalamin, and since it is little more expensive than cyanocobalamin, and has longer retention times in the body, has been used for vitamin replacement in situations where added reassurance of activity is desired. Intramuscular administration of hydroxocobalamin is also the preferred treatment for pediatric patients with intrinsic cobalamin metabolic diseases, for vitamin B12 deficient patients with tobacco amblyopia (which is thought to perhaps have a component of cyanide poisoning from cyanide in cigarette smoke); and for treatment of patients with pernicious anemia who have optic neuropathy.
Adenosylcobalamin (adoB12) and methylcobalamin (MeB12) are the two enzymatically active cofactor forms of B12 that naturally occur in the body. Most of the body's reserves are stored as adoB12 in the liver. These are converted to the other methylcobalamin form as needed.
Synthesis and industrial production
Neither plants nor animals are independently capable of constructing vitamin B12.[68] Only bacteria and archaea[69] have the enzymes required for its biosynthesis. The total synthesis of B12 was reported by Robert Burns Woodward[70] and Albert Eschenmoser in 1972,[71][72] and remains one of the classic feats of organic synthesis. Species from the following genera are known to synthesize B12: Acetobacterium, Aerobacter, Agrobacterium, Alcaligenes, Azotobacter, Bacillus, Clostridium, Corynebacterium, Flavobacterium, Lactobacillus, Micromonospora, Mycobacterium, Nocardia, Propionibacterium, Protaminobacter, Proteus, Pseudomonas, Rhizobium, Salmonella, Serratia, Streptomyces, Streptococcus and Xanthomonas.
Industrial production of B12 is through fermentation of selected microorganisms.[73] Streptomyces griseus, a bacterium once thought to be a yeast, was the commercial source of vitamin B12 for many years.[74][75] The species Pseudomonas denitrificans and Propionibacterium freudenreichii subsp. shermanii are more commonly used today.[76] These are frequently grown under special conditions to enhance yield, and at least one company, Rhône-Poulenc of France, which has merged into Sanofi-Aventis, used genetically engineered versions of one or both of these species. Since a number of species of Propionibacterium produce no exotoxins or endotoxins and are generally regarded as safe (have been granted GRAS status) by the Food and Drug Administration of the United States, they are presently the FDA-preferred bacterial fermentation organisms for vitamin B12 production.[77]
The total world production of vitamin B12, by four companies (the French Sanofi-Aventis and three Chinese companies) is said to have been 35 tonnes in 2008.[78]
See cyanocobalamin for discussion of the chemical preparation of reduced-cobalt vitamin analogs and preparation of physiological forms of the vitamin such as adenosylcobalamin and methylcobalamin.
Mechanism of action

Coenzyme B12's reactive C-Co bond participates in three main types of enzyme-catalyzed reactions.[79][80]
- Isomerases
- Rearrangements in which a hydrogen atom is directly transferred between two adjacent atoms with concomitant exchange of the second substituent, X, which may be a carbon atom with substituents, an oxygen atom of an alcohol, or an amine. These use the adoB12 (adenosylcobalamin) form of the vitamin.
- Methyltransferases
- Methyl (-CH3) group transfers between two molecules. These use MeB12 (methylcobalamin) form of the vitamin.
- Dehalogenases
- Reactions in which a halogen atom is removed from an organic molecule. Enzymes in this class have not been identified in humans.
In humans, two major coenzyme B12-dependent enzyme families corresponding to the first two reaction types, are known. These are typified by the following two enzymes:
- MUT is an isomerase which uses the AdoB12 form and reaction type 1 to catalyze a carbon skeleton rearrangement (the X group is -COSCoA). MUT's reaction converts MMl-CoA to Su-CoA, an important step in the extraction of energy from proteins and fats (for more see MUT's reaction mechanism). This functionality is lost in vitamin B12 deficiency, and can be measured clinically as an increased methylmalonic acid (MMA) level. Unfortunately, an elevated MMA, though sensitive to B12 deficiency, is probably overly sensitive, and not all who have it actually have B12 deficiency. For example, MMA is elevated in 90–98% of patients with B12 deficiency; however 20–25% of patients over the age of 70 have elevated levels of MMA, yet 25–33% of them do not have B12 deficiency. For this reason, assessment of MMA levels is not routinely recommended in the elderly. There is no "gold standard" test for B12 deficiency because as a B12 deficiency occurs, serum values may be maintained while tissue B12 stores become depleted. Therefore, serum B12 values above the cut-off point of deficiency do not necessarily indicate adequate B12 status[21] The MUT function is necessary for proper myelin synthesis (see mechanism below) and is not affected by folate supplementation.
- MTR, also known as methionine synthase, is a methyltransferase enzyme, which uses the MeB12 and reaction type 2 to transfer a methyl group from 5-methyltetrahydrofolate to homocysteine, thereby generating tetrahydrofolate (THF) and methionine (for more see MTR's reaction mechanism).[81] This functionality is lost in vitamin B12 deficiency, resulting in an increased homocysteine level and the trapping of folate as 5-methyl-tetrahydrofolate, from which THF (the active form of folate) cannot be recovered. THF plays an important role in DNA synthesis so reduced availability of THF results in ineffective production of cells with rapid turnover, in particular red blood cells, and also intestinal wall cells which are responsible for absorption. THF may be regenerated via MTR or may be obtained from fresh folate in the diet. Thus all of the DNA synthetic effects of B12 deficiency, including the megaloblastic anemia of pernicious anemia, resolve if sufficient dietary folate is present.[65] Thus the best-known "function" of B12 (that which is involved with DNA synthesis, cell-division, and anemia) is actually a facultative function which is mediated by B12-conservation of an active form of folate which is needed for efficient DNA production.[82] Other cobalamin-requiring methyltransferase enzymes are also known in bacteria, such as Me-H4-MPT, coenzyme M methyl transferase.
Enzyme function
If folate is present in quantity, then of the two absolutely vitamin B12-dependent enzyme-family reactions in humans, the MUT-family reactions show the most direct and characteristic secondary effects, focusing on the nervous system (see below). This is because the MTR (methyltransferase-type) reactions are involved in regenerating folate, and thus are less evident when folate is in good supply.
Since the late 1990s, folic acid has begun to be added to fortify flour in many countries, so folate deficiency is now more rare. At the same time, since DNA synthetic-sensitive tests for anemia and erythrocyte size are routinely done in even simple medical test clinics (so that these folate-mediated biochemical effects are more often directly detected), the MTR-dependent effects of B12 deficiency are becoming apparent not as anemia due to DNA-synthetic problems (as they were classically), but now mainly as a simple and less obvious elevation of homocysteine in the blood and urine (homocysteinuria). This condition may result in long term damage to arteries and in clotting (stroke and heart attack), but this effect is difficult to separate from other common processes associated with atherosclerosis and aging.
The specific myelin damage resulting from B12 deficiency, even in the presence of adequate folate and methionine, is more specifically and clearly a vitamin deficiency problem. It has been connected to B12 most directly by reactions related to MUT, which is absolutely required to convert methylmalonyl coenzyme A into succinyl coenzyme A. Failure of this second reaction to occur results in elevated levels of MMA, a myelin destabilizer. Excessive MMA will prevent normal fatty acid synthesis, or it will be incorporated into fatty acid itself rather than normal malonic acid. If this abnormal fatty acid subsequently is incorporated into myelin, the resulting myelin will be too fragile, and demyelination will occur. Although the precise mechanism(s) are not known with certainty, the result is subacute combined degeneration of central nervous system and spinal cord.[83] Whatever the cause, it is known that B12 deficiency causes neuropathies, even if folic acid is present in good supply, and therefore anemia is not present.
Vitamin B12-dependent MTR reactions may also have neurological effects, through an indirect mechanism. Adequate methionine (which, like folate, must otherwise be obtained in the diet, if it is not regenerated from homocysteine by a B12 dependent reaction) is needed to make S-adenosyl-methionine (SAMe), which is in turn necessary for methylation of myelin sheath phospholipids. Although production of SAMe is not B12 dependent, help in recycling for provision of one adequate substrate for it (the essential amino acid methionine) is assisted by B12. In addition, SAMe is involved in the manufacture of certain neurotransmitters, catecholamines and in brain metabolism. These neurotransmitters are important for maintaining mood, possibly explaining why depression is associated with B12 deficiency. Methylation of the myelin sheath phospholipids may also depend on adequate folate, which in turn is dependent on MTR recycling, unless ingested in relatively high amounts.
Absorption and distribution
Methyl-B12 is absorbed by an intestinal mechanism using intrinsic factor and by a diffusion process in which approximately 1% of the oral dose is absorbed.[84] The human physiology of vitamin B12 is complex, and therefore is prone to mishaps leading to vitamin B12 deficiency. Protein-bound vitamin B12 must be released from the proteins by the action of digestive proteases in both the stomach and small intestine.[85] Gastric acid releases the vitamin from food particles; therefore antacid and acid-blocking medications (especially proton-pump inhibitors) may inhibit absorption of B12. In addition some elderly people produce less stomach acid as they age thereby increasing their probability of B12 deficiencies.[86]
B12 taken in a low-solubility, non-chewable supplement pill form may bypass the mouth and stomach and not mix with gastric acids, but these are not necessary for the absorption of free B12 not bound to protein.
R-proteins (such as haptocorrins and cobalaphilin) are B12 binding proteins that are produced in the salivary glands. They must wait until B12 has been freed from proteins in food by pepsin in the stomach. B12 then binds to the R-Proteins to avoid degradation of it in the acidic environment of the stomach.[87]
This pattern of secretion of a binding protein secreted in a previous digestive step is repeated once more before absorption. The next binding protein is intrinsic factor (IF), a protein synthesized by gastric parietal cells that is secreted in response to histamine, gastrin and pentagastrin, as well as the presence of food. In the duodenum, proteases digest R-proteins and release B12, which then binds to IF, to form a complex (IF/B12). B12 must be attached to IF for it to be absorbed, as receptors on the enterocytes in the terminal ileum of the small bowel only recognize the B12-IF complex; in addition, intrinsic factor protects the vitamin from catabolism by intestinal bacteria.
Absorption of food vitamin B12 thus requires an intact and functioning stomach, exocrine pancreas, intrinsic factor, and small bowel. Problems with any one of these organs makes a vitamin B12 deficiency possible. Individuals who lack intrinsic factor have a decreased ability to absorb B12. In pernicious anemia, there is a lack of IF due to autoimmune atrophic gastritis, in which antibodies form against parietal cells. Antibodies may alternately form against and bind to IF, inhibiting it from carrying out its B12 protective function. Due to the complexity of B12 absorption, geriatric patients, many of whom are hypoacidic due to reduced parietal cell function, have an increased risk of B12 deficiency.[88] This results in 80–100% excretion of oral doses in the feces versus 30–60% excretion in feces as seen in individuals with adequate IF.[88]
Once the IF/B12 complex is recognized by specialized ileal receptors, it is transported into the portal circulation. The vitamin is then transferred to transcobalamin II (TC-II/B12), which serves as the plasma transporter. Hereditary defects in production of the transcobalamins and their receptors may produce functional deficiencies in B12 and infantile megaloblastic anemia, and abnormal B12 related biochemistry, even in some cases with normal blood B12 levels.[89] For the vitamin to serve inside cells, the TC-II/B12 complex must bind to a cell receptor, and be endocytosed. The transcobalamin-II is degraded within a lysosome, and free B12 is finally released into the cytoplasm, where it may be transformed into the proper coenzyme, by certain cellular enzymes (see above).
It's important to note that investigations into the intestinal absorption of B12 point out that the upper limit per single dose, under normal conditions, is about 1.5 µg: "Studies in normal persons indicated that about 1.5 µg is assimilated when a single dose varying from 5 to 50 µg is administered by mouth. In a similar study Swendseid et al. stated that the average maximum absorption was 1.6 µg [...]" [90]
The total amount of vitamin B12 stored in body is about 2–5 mg in adults. Around 50% of this is stored in the liver.[21] Approximately 0.1% of this is lost per day by secretions into the gut, as not all these secretions are reabsorbed. Bile is the main form of B12 excretion; however, most of the B12 secreted in the bile is recycled via enterohepatic circulation. Excess B12 beyond the blood's binding capacity is typically excreted in urine.[21] Owing to the extremely efficient enterohepatic circulation of B12, the liver can store several years’ worth of vitamin B12; therefore, nutritional deficiency of this vitamin is rare. How fast B12 levels change depends on the balance between how much B12 is obtained from the diet, how much is secreted and how much is absorbed. B12 deficiency may arise in a year if initial stores are low and genetic factors unfavourable, or may not appear for decades. In infants, B12 deficiency can appear much more quickly.[91]
History
B12 deficiency is the cause of pernicious anemia, an anemic disease that was usually fatal and had unknown etiology when it was first described in medicine. The cure, and B12, were discovered by accident. George Whipple had been doing experiments in which he induced anemia in dogs by bleeding them, and then fed them various foods to observe which diets allowed them fastest recovery from the anemia produced. In the process, he discovered that ingesting large amounts of liver seemed to most rapidly cure the anemia of blood loss. Thus, he hypothesized that liver ingestion might treat pernicious anemia. He tried this and reported some signs of success in 1920.
After a series of careful clinical studies, George Richards Minot and William Murphy set out to partly isolate the substance in liver which cured anemia in dogs, and found that it was iron. They also found that an entirely different liver substance cured pernicious anemia in humans, that had no effect on dogs under the conditions used. The specific factor treatment for pernicious anemia, found in liver juice, had been found by this coincidence. Minot and Murphy reported these experiments in 1926. This was the first real progress with this disease. Despite this discovery, for several years patients were still required to eat large amounts of raw liver or to drink considerable amounts of liver juice.
In 1928, the chemist Edwin Cohn prepared a liver extract that was 50 to 100 times more potent than the natural liver products. The extract was the first workable treatment for the disease. For their initial work in pointing the way to a working treatment, Whipple, Minot, and Murphy shared the 1934 Nobel Prize in Physiology or Medicine.
These events in turn eventually led to discovery of the soluble vitamin, called vitamin B12, from bacterial broths. In 1947, while working for the Poultry Science Department at the University of Maryland, Mary Shaw Shorb (in a collaborative project with Folkers and Merck) was provided with a $400 grant to develop the so-called "LLD assay" for B12. LLD stood for Lactobacilis lactis Dorner, a strain of bacterium which required "LLD factor" for growth, which was eventually identified as B12. Shorb and colleagues used the LLD assay to rapidly extract the anti-pernicious anemia factor from liver extracts, and pure B12 was isolated in this way by 1948, with the contributions of chemists Shorb,[92] Karl A. Folkers of the United States and Alexander R. Todd of Great Britain. For this discovery, in 1949 Mary Shorb and Karl Folkers received the Mead Johnson Award from the American Society of Nutritional Sciences.[92]
The chemical structure of the molecule was determined by Dorothy Crowfoot Hodgkin and her team in 1956, based on crystallographic data.[93] Eventually, methods of producing the vitamin in large quantities from bacteria cultures were developed in the 1950s, and these led to the modern form of treatment for the disease.
See also
- Cobamamide
- Cyanocobalamin includes discussion of chemistry of preparation of reduced-cobalt B12 analogs
- Hydroxocobalamin
- Methylcobalamin
References
- ↑ Yamada, Kazuhiro (2013). "Chapter 9. Cobalt: Its Role in Health and Disease". In Astrid Sigel, Helmut Sigel and Roland K. O. Sigel. Interrelations between Essential Metal Ions and Human Diseases. Metal Ions in Life Sciences 13. Springer. pp. 295–320. doi:10.1007/978-94-007-7500-8_9.
- ↑ 2.0 2.1 2.2 2.3 "Dietary Supplement Fact Sheet: Vitamin B12". Office of Dietary Supplements, National Institutes of Health. Retrieved 28 September 2011.
- ↑ Albert, M. J.; Mathan, V. I.; Baker, S. J. (1980). "Vitamin B12 synthesis by human small intestinal bacteria". Nature 283 (5749): 781–782. doi:10.1038/283781a0. PMID 7354869.
- ↑ Chanarin, I.; Muir, M. (1982). "Demonstration of vitamin B12 analogues in human sera not detected by microbiological assay". British journal of haematology 51 (1): 171–173. doi:10.1111/j.1365-2141.1982.tb07301.x. PMID 7041953.
- ↑ Kelly, R. J.; Gruner, T. M.; Furlong, J. M.; Sykes, A. R. (2006). "Analysis of corrinoids in ovine tissues". Biomedical Chromatography 20 (8): 806–814. doi:10.1002/bmc.604. PMID 16345011.
- ↑ 6.0 6.1 Yamada, K.; Shimodaira, M.; Chida, S.; Yamada, N.; Matsushima, N.; Fukuda, M.; Yamada, S. (2008). "Degradation of Vitamin B12 in Dietary Supplements". International Journal for Vitamin and Nutrition Research 78 (45): 195–203. doi:10.1024/0300-9831.78.45.195. PMID 19326342.
- ↑ 7.0 7.1 Herbert, V.; Drivas, G.; Foscaldi, R.; Manusselis, C.; Colman, N.; Kanazawa, S.; Das, K.; Gelernt, M.; Herzlich, B.; Jennings, J. (1982). "Multivitamin/Mineral Food Supplements Containing Vitamin B12May Also Contain Analogues of Vitamin B12". New England Journal of Medicine 307 (4): 255–256. doi:10.1056/NEJM198207223070424. PMID 7088084.
- ↑ 8.0 8.1 Watanabe, F.; Katsura, H.; Takenaka, S.; Fujita, T.; Abe, K.; Tamura, Y.; Nakatsuka, T.; Nakano, Y. (1999). "Pseudovitamin B(12) is the predominant cobamide of an algal health food, spirulina tablets". Journal of agricultural and food chemistry 47 (11): 4736–4741. doi:10.1021/jf990541b. PMID 10552882.
- ↑ 9.0 9.1 9.2 Yamada, K.; Yamada, Y.; Fukuda, M.; Yamada, S. (1999). "Bioavailability of dried asakusanori (porphyra tenera) as a source of Cobalamin (Vitamin B12)". International journal for vitamin and nutrition research. Internationale Zeitschrift fur Vitamin- und Ernahrungsforschung. Journal international de vitaminologie et de nutrition 69 (6): 412–418. doi:10.1024/0300-9831.69.6.412. PMID 10642899.
- ↑ 10.0 10.1 "Vitamin B12". The American Society of Health-System Pharmacists. Retrieved 3 April 2011.
- ↑ Hall AH, Rumack BH (1987). "Hydroxycobalamin/sodium thiosulfate as a cyanide antidote". The Journal of Emergency Medicine 5 (2): 115–21. doi:10.1016/0736-4679(87)90074-6. PMID 3295013.
- ↑ Dart RC (2006). "Hydroxocobalamin for acute cyanide poisoning: new data from preclinical and clinical studies; new results from the prehospital emergency setting". Clinical Toxicology 44 (Suppl 1): 1–3. doi:10.1080/15563650600811607. PMID 16990188.
- ↑ Vogiatzoglou A, Refsum H, Johnston C et al. (2008). "Vitamin B12 status and rate of brain volume loss in community-dwelling elderly". Neurology 71 (11): 826–32. doi:10.1212/01.wnl.0000325581.26991.f2. PMID 18779510.
- ↑ O'Conner, Richard D. M.D. (1990). "FDA investigational New Drug IND No. 30,488". (link needed)
- ↑ "Dietary Supplement Fact Sheet: Vitamin B12 — Health Professional Fact Sheet". Office of Dietary Supplements. National Institutes of Health. 2011-06-24. Retrieved 2012-11-02.
- ↑ "Vitamins and minerals – B vitamins and folic acid". NHS. National Health Service. 2012-11-26. Retrieved 2013-07-10.
- ↑ "Vitamin B12 recommendation change". American Journal of Nutrition Facts. NutritionFacts.org. 2010. Retrieved 2014-09-19.
- ↑ "Guidance for Industry: A Food Labeling Guide (14. Appendix F: Calculate the Percent Daily Value for the Appropriate Nutrients)". U.S. Food and Drug Administration. Retrieved 30 October 2014.
- ↑ Institute Of Medicine (Us) Standing Committee On The Scientific Evaluation Of Dietary Reference Intakes And Its Panel On Folate, Other B Vitamins (1998). "Dietary Reference Intakes: Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline". Food and Nutrition Board, Institute of Medicine (Washington, DC: National Academy Press). ISBN 0-309-06554-2.
- ↑ Institute of Medicine (1998). "Vitamin B12". Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC: The National Academies Press. pp. 340–342. ISBN 0-309-06554-2. Retrieved 2012-02-07.
- ↑ 21.0 21.1 21.2 21.3 Vitamin B12, usda.gov
- ↑ Walsh, Stephen. "What every vegan should know about vitamin B12". Vegan Society. Archived from the original on 2007-07-17. Retrieved 2007-12-03.
- ↑ 23.0 23.1 Mangels, Reed. "Vitamin B12 in the Vegan Diet". Vegetarian Resource Group. Retrieved 2008-01-17.
- ↑ 24.0 24.1 "Don't Vegetarians Have Trouble Getting Enough Vitamin B12?". Physicians Committee for Responsible Medicine. Retrieved 2008-01-17.
- ↑ 25.0 25.1 Kittaka-Katsura, H.; Fujita, T.; Watanabe, F.; Nakano, Y. (2002). "Purification and characterization of a corrinoid compound from Chlorella tablets as an algal health food". Journal of agricultural and food chemistry 50 (17): 4994–4997. doi:10.1021/jf020345w. PMID 12166996.
- ↑ 26.0 26.1 Watanabe, F.; Takenaka, S.; Kittaka-Katsura, H.; Ebara, S.; Miyamoto, E. (2002). "Characterization and bioavailability of vitamin B12-compounds from edible algae". Journal of nutritional science and vitaminology 48 (5): 325–331. doi:10.3177/jnsv.48.325. PMID 12656203.
- ↑ 27.0 27.1 Watanabe, F.; Takenaka, S.; Katsura, H.; Miyamoto, E.; Abe, K.; Tamura, Y.; Nakatsuka, T.; Nakano, Y. (2000). "Characterization of a vitamin B12 compound in the edible purple laver, Porphyra yezoensis". Bioscience, biotechnology, and biochemistry 64 (12): 2712–2715. doi:10.1271/bbb.64.2712. PMID 11210144.
- ↑ 28.0 28.1 Takenaka, S.; Sugiyama, S.; Ebara, S.; Miyamoto, E.; Abe, K.; Tamura, Y.; Watanabe, F.; Tsuyama, S.; Nakano, Y. (2001). "Feeding dried purple laver (nori) to vitamin B12-deficient rats significantly improves vitamin B12 status". The British journal of nutrition 85 (6): 699–703. doi:10.1079/BJN2001352. PMID 11430774.
- ↑ Sethi NK, Robilotti E, Sadan Y (2005). "Neurological Manifestations Of Vitamin B-12 Deficiency". The Internet Journal of Nutrition and Wellness 2 (1). doi:10.5580/5a9.
- ↑ Masalha R, Chudakov B, Muhamad M, Rudoy I, Volkov I, Wirguin I (2001). "Cobalamin-responsive psychosis as the sole manifestation of vitamin B12 deficiency". Israeli Medical Association Journal 3: 701–703. PMID 11574992.
- ↑ Killen, J. P.; Brenninger, V. L. (2013). "Vitamin B12 deficiency". N. Engl. J. Med 368: 2040–1. doi:10.1056/nejmc1304350.
- ↑ Biemans, E.; Hart, H.E.; Rutten, G.E.; Renteria, V.G.C.; Kooijman-Buiting, A.M.; Beulens, J.W. (2014). "Cobalamin status has a relationship with depression, cognition and neuropathy in patients with Type 2 diabetes mellitus using metformin". Acta diabetologica: 1–11.
- ↑ Bottiglieri, T.; Laundy, M.; Crellin, R.; Toone, B.K.; Carney, M.W.; Reynolds, E.H. (2000). "Homocysteine, folate, methylation, and monoamine metabolism in depression". Journal of Neurology, Neurosurgery & Psychiatry 69 (2): 228–232. doi:10.1136/jnnp.69.2.228.
- ↑ Doscherholmen, A.; McMahon, J.; Ripley, D. (1975). "Vitamin B12 absorption from eggs". Proceedings of the Society for Experimental Biology and Medicine. Society for Experimental Biology and Medicine 149 (4): 987–990. doi:10.3181/00379727-149-38940. PMID 1172618.
- ↑ Kwak, C. S.; Lee, M. S.; Lee, H. J.; Whang, J. Y.; Park, S. C. (2010). "Dietary source of vitamin B12intake and vitamin B12status in female elderly Koreans aged 85 and older living in rural area". Nutrition Research and Practice 4 (3): 229–234. doi:10.4162/nrp.2010.4.3.229. PMC 2895704. PMID 20607069.
- ↑ Kwak, C. S.; Lee, M. S.; Oh, S. I.; Park, S. C. (2010). "Discovery of Novel Sources of Vitamin B12 in Traditional Korean Foods from Nutritional Surveys of Centenarians". Current Gerontology and Geriatrics Research 2010: 1. doi:10.1155/2010/374897. PMC 3062981. PMID 21436999.
- ↑ Kittaka-Katsura, H.; Ebara, S.; Watanabe, F.; Nakano, Y. (2004). "Characterization of Corrinoid Compounds from a Japanese Black Tea (Batabata-cha) Fermented by Bacteria". Journal of Agricultural and Food Chemistry 52 (4): 909–911. doi:10.1021/jf030585r. PMID 14969549.
- ↑ Nakano, S.; Takekoshi, H.; Nakano, M. (2009). "Chlorella pyrenoidosa Supplementation Reduces the Risk of Anemia, Proteinuria and Edema in Pregnant Women". Plant Foods for Human Nutrition 65 (1): 25–30. doi:10.1007/s11130-009-0145-9. PMID 20013055.
- ↑ Croft, M. T.; Lawrence, A. D.; Raux-Deery, E.; Warren, M. J.; Smith, A. G. (2005). "Algae acquire vitamin B12 through a symbiotic relationship with bacteria". Nature 438 (7064): 90–93. doi:10.1038/nature04056. PMID 16267554.
- ↑ Kazamia, E.; Czesnick, H. R.; Nguyen, T. T. V.; Croft, M. T.; Sherwood, E.; Sasso, S.; Hodson, S. J.; Warren, M. J.; Smith, A. G. (2012). "Mutualistic interactions between vitamin B12-dependent algae and heterotrophic bacteria exhibit regulation". Environmental Microbiology 14 (6): 1466–1476. doi:10.1111/j.1462-2920.2012.02733.x. PMID 22463064.
- ↑ Moore, S. J.; Lawrence, A. D.; Biedendieck, R; Deery, E; Frank, S; Howard, M. J.; Rigby, S. E.; Warren, M. J. (2013). "Elucidation of the anaerobic pathway for the corrin component of cobalamin (vitamin B12)". Proceedings of the National Academy of Sciences 110 (37): 14906–11. doi:10.1073/pnas.1308098110. PMC 3773766. PMID 23922391.
- ↑ Walsh, Stephen, RD. "Vegan Society B12factsheet". Vegan Society. Retrieved 2008-01-17.
- ↑ Herbert, Victor (1988). "Vitamin B-12: Plant sources, requirements, and assay" (PDF). The American journal of clinical nutrition 48 (3 Suppl): 852–8. PMID 3046314.
- ↑ Daisley, K. W. (1969). "Monthly survey of vitamin B12 concentration in some waters of the English Lake District" (PDF). Limnol. Oceanogr. 14 (2): 224–228. doi:10.4319/lo.1969.14.2.0224.
- ↑ Wakayama EJ, Dillwith JW, Howard RW, Blomquist GJ; Dillwith; Howard; Blomquist (1984). "Vitamin B12 levels in selected insects". Insect Biochemistry 14 (2): 175–179. doi:10.1016/0020-1790(84)90027-1.
- ↑ Albert MJ, Mathan VI, Baker SJ; Mathan; Baker (1980). "Vitamin B12 synthesis by human small intestinal bacteria". INature 283 (5749): 781–782. doi:10.1038/283781a0. PMID 7354869.
- ↑ Sharabi, A; Cohen, E; Sulkes, J; Garty, M (2003). "Replacement therapy for vitamin B12 deficiency: comparison between the sublingual and oral route". British Journal of Clinical Pharmacology 56 (6): 635–8. doi:10.1046/j.1365-2125.2003.01907.x. PMC 1884303. PMID 14616423.
- ↑ Bolaman Z, Kadikoylu G, Yukselen V, Yavasoglu I, Barutca S, Senturk T; Kadikoylu; Yukselen; Yavasoglu; Barutca; Senturk (2003). "Oral versus intramuscular cobalamin treatment in megaloblastic anemia: a single-center, prospective, randomized, open-label study". Clin Ther 25 (12): 3124–34. doi:10.1016/S0149-2918(03)90096-8. PMID 14749150.
- ↑ Lane LA, Rojas-Fernandez C; Rojas-Fernandez (2002). "Treatment of vitamin b(12)-deficiency anemia: oral versus parenteral therapy". Ann Pharmacother 36 (7–8): 1268–72. doi:10.1345/aph.1A122. PMID 12086562.
- ↑ Butler, C. C. (2006). "Oral vitamin B12 versus intramuscular vitamin B12 for vitamin B12 deficiency: A systematic review of randomized controlled trials". Family Practice 23 (3): 279. doi:10.1093/fampra/cml008.
- ↑ Andersson HC, Shapira E; Shapira (1998). "Biochemical and clinical response to hydroxocobalamin versus cyanocobalamin treatment in patients with methylmalonic acidemia and homocystinuria (cblC)". J. Pediatr. 132 (1): 121–4. doi:10.1016/S0022-3476(98)70496-2. PMID 9470012.
- ↑ Roze E, Gervais D, Demeret S et al. (2003). "Neuropsychiatric disturbances in presumed late-onset cobalamin C disease". Arch. Neurol. 60 (10): 1457–62. doi:10.1001/archneur.60.10.1457. PMID 14568819.
- ↑ Thauvin-Robinet C, Roze E, Couvreur G et al. (2008). "The adolescent and adult form of cobalamin C disease: clinical and molecular spectrum". J. Neurol. Neurosurg. Psychiatr. 79 (6): 725–8. doi:10.1136/jnnp.2007.133025. PMID 18245139.
- ↑ Heil SG, Hogeveen M, Kluijtmans LA et al. (2007). "Marfanoid features in a child with combined methylmalonic aciduria and homocystinuria (CblC type)". J. Inherit. Metab. Dis. 30 (5): 811. doi:10.1007/s10545-007-0546-6. PMID 17768669.
- ↑ Tsai, A. C. H.; Morel, C. F.; Scharer, G.; Yang, M.; Lerner-Ellis, J. P.; Rosenblatt, D. S.; Thomas, J. A. (2007). "Late-onset combined homocystinuria and methylmalonic aciduria (cblC) and neuropsychiatric disturbance". American Journal of Medical Genetics Part A 143A (20): 2430. doi:10.1002/ajmg.a.31932.
- ↑ "5’-deoxyadenosylcobalamin and methylcobalamin as sources for Vitamin B12 added as a nutritional substance in food supplements[1] - Scientific opinion of the Scientific Panel on Food Additives and Nutrient Sources added to food". EFSA Journal 815: 1–21. 2008. doi:10.2903/j.efsa.2008.815. "the metabolic fate and biological distribution of methylcobalamin and 5’-deoxyadenosylcobalamin are expected to be similar to that of other sources of vitamin B12 in the diet."
- ↑ "5’-deoxyadenosylcobalamin and methylcobalamin as sources for Vitamin B12 added as a nutritional substance in food supplements[1] - Scientific opinion of the Scientific Panel on Food Additives and Nutrient Sources added to food". EFSA Journal 815: 1–21. 2008. doi:10.2903/j.efsa.2008.815.
- ↑ Pott JW, Wong KH (2006). "Leber's hereditary optic neuropathy and vitamin B12 deficiency". Graefe's Archive for Clinical and Experimental Ophthalmology 244 (10): 1357–9. doi:10.1007/s00417-006-0269-7. PMID 16523300.
- ↑ De Jager, J.; Kooy, A.; Lehert, P.; Wulffelé, M. G.; Van Der Kolk, J.; Bets, D.; Verburg, J.; Donker, A. J. M.; Stehouwer, C. D. A. (2010). "Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency: Randomised placebo controlled trial". BMJ 340: c2181. doi:10.1136/bmj.c2181. PMC 2874129. PMID 20488910.
- ↑ Andrès E, Noel E, Goichot B (2002). "Metformin-associated vitamin B12 deficiency". Arch Intern Med 162 (19): 2251–2. doi:10.1001/archinte.162.19.2251-a. PMID 12390080.
- ↑ Gilligan M (2002). "Metformin and vitamin B12 deficiency". Arch Intern Med 162 (4): 484–5. doi:10.1001/archinte.162.4.484. PMID 11863489.
- ↑ Bauman, WA; Shaw, S; Jayatilleke, E; Spungen, AM; Herbert, V (2000). "Increased intake of calcium reverses vitamin B12 malabsorption induced by metformin". Diabetes Care 23 (9): 1227–31. doi:10.2337/diacare.23.9.1227. PMID 10977010.
- ↑ Copp, Samantha (2007-12-01). "What effect does metformin have on vitamin B12 levels?". UK Medicines Information, NHS.
- ↑ Conrad, Marcel (2006-10-04). "Pernicious Anemia". Retrieved 2008-06-02.
- ↑ 65.0 65.1 "Argument for providing B12 with food fortification of folate, since otherwise folate will correct hematological symptoms while leaving neurological symptoms to progress". Victorherbert.com. Retrieved 2013-04-20.
- ↑ Palva, I. P.; Salokannel, S. J.; Timonen, T; Palva, H. L. (1972). "Drug-induced malabsorption of vitamin B 12 . IV. Malabsorption and deficiency of B 12 during treatment with slow-release potassium chloride". Acta medica Scandinavica 191 (4): 355–7. PMID 5032681.
- ↑ Jaouen, G., ed. (2006). Bioorganometallics: Biomolecules, Labeling, Medicine. Weinheim: Wiley-VCH. ISBN 3-527-30990-X.
- ↑ Loeffler, G. (2005). Basiswissen Biochemie. Heidelberg: Springer. p. 606. ISBN 3-540-23885-9.
- ↑ Bertrand EM; Saito MA; Young JJ; Neilan BA (2011). "Vitamin B12 biosynthesis gene diversity in the Ross Sea: the identification of a new group of putative polar B12 biosynthes". Environmental Microbiology 13 (5): 1285–98. doi:10.1111/j.1462-2920.2011.02428.x. PMID 21410623.
- ↑ Khan, Adil Ghani; Eswaran, S. V. (2003). "Woodward's synthesis of vitamin B12". Resonance 8 (6): 8. doi:10.1007/BF02837864.
- ↑ Eschenmoser A, Wintner CE (June 1977). "Natural product synthesis and vitamin B12". Science 196 (4297): 1410–20. doi:10.1126/science.867037. PMID 867037.
- ↑ Riether, Doris; Mulzer, Johann (2003). "Total Synthesis of Cobyric Acid: Historical Development and Recent Synthetic Innovations". European Journal of Organic Chemistry 2003: 30. doi:10.1002/1099-0690(200301)2003:1<30::AID-EJOC30>3.0.CO;2-I.
- ↑ Martens JH, Barg H, Warren MJ, Jahn D (2002). "Microbial production of vitamin B12". Applied Microbiology and Biotechnology 58 (3): 275–85. doi:10.1007/s00253-001-0902-7. PMID 11935176.
- ↑ Linnell JC, Matthews DM (1984). "Cobalamin metabolism and its clinical aspects". Clinical Science 66 (2): 113–21. PMID 6420106.
- ↑ Vitamin B12. Code of Federal Regulations. U.S. Government Printing Office. Title 21, Volume 3. Revised. April 1, 2001. CITE: 21CFR184.1945 p. 552
- ↑ De Baets S, Vandedrinck S, Vandamme EJ (2000). "Vitamins and Related Biofactors, Microbial Production". In Lederberg J. Encyclopedia of Microbiology 4 (2nd ed.). New York: Academic Press. pp. 837–853. ISBN 0-12-226800-8.
- ↑ Riaz, Muhammad; Iqbal, Fouzia; Akram, Muhammad (2007). "Microbial production of vitamin B12 by methanol utilizing strain of Pseudomonas specie". Pak J. Biochem. Mol. Biol. 1 40: 5–10.
- ↑ Yemei, Zhang (January 26, 2009) New round of price slashing in vitamin B12 sector. (Fine and Specialty). China Chemical Reporter.
- ↑ Voet, Judith G.; Voet, Donald (1995). Biochemistry. New York: J. Wiley & Sons. p. 675. ISBN 0-471-58651-X. OCLC 31819701.
- ↑ Banerjee, R; Ragsdale, SW (2003). "The many faces of vitamin B12: catalysis by cobalamin-dependent enzymes". Annual review of biochemistry 72: 209–47. doi:10.1146/annurev.biochem.72.121801.161828. PMID 14527323.
- ↑ Banerjee RV, Matthews RG (1990). "Cobalamin-dependent methionine synthase". The FASEB Journal 4 (5): 1450–9. PMID 2407589.
- ↑ Wickramasinghe SN (1995). "Morphology, biology and biochemistry of cobalamin- and folate-deficient bone marrow cells". Baillière's Clinical Haematology 8 (3): 441–59. doi:10.1016/S0950-3536(05)80215-X. PMID 8534956.
- ↑ Naidich MJ, Ho SU (2005). "Case 87: Subacute combined degeneration". Radiology 237 (1): 101–5. doi:10.1148/radiol.2371031757. PMID 16183926.
- ↑ CerefolinNAC® Caplets. intetlab.com
- ↑ Marks, Allan D. (2009) Basic Medical Biochemistry: A Clinical Approach, 3rd ed., Lippincott Williams & Wilkins, p. 757, ISBN 078177022X.
- ↑ Beck, Melinda (January 18, 2011). "Sluggish? Confused? Vitamin B12 May Be Low". The Wall Street Journal.
- ↑ Allen, RH; Seetharam, B; Podell, E; Alpers, DH (1978). "Effect of Proteolytic Enzymes on the Binding of Cobalamin to R Protein and Intrinsic Factor". The Journal of Clinical Investigation 61 (1): 47–54. doi:10.1172/JCI108924. PMC 372512. PMID 22556.
- ↑ 88.0 88.1 Combs, Gerald F. (2008). The vitamins: fundamental aspects in nutrition and health (3rd ed.). Amsterdam: Elsevier Academic Press. ISBN 0-12-183492-1. OCLC 150255807.
- ↑ Conrad, Marcel E (August 26, 2009) Pernicious Anemia. emedicine.medscape.com
- ↑ Abels, J.; Vegter, J. J. M.; Woldring, M. G.; Jans, J. H.; Nieweg, H. O. (2009). "The Physiologic Mechanism of Vitamin B12 Absorption". Acta Medica Scandinavica 165 (2): 105. doi:10.1111/j.0954-6820.1959.tb14477.x.
- ↑ "B12: An essential part of a healthy plant-based diet". International Vegetarian Union.
- ↑ 92.0 92.1 "Dr. Mary Shaw Shorb – Annual Lecture". Department of Animal & Avian Sciences, University of Maryland. May 10, 2012.
- ↑ Kirkland, Kyle (2010). Biological Sciences: Notable Research and Discoveries. Facts on File, Inc. p. 87. ISBN 0816074399.
External links
- Vitamin B12 Fact Sheet from the U.S. National Institutes of Health
- Jane Higdon, "Vitamin B12", Micronutrient Information Center, Linus Pauling Institute, Oregon State University
- Vitamin B12 deficiency article in American Family Physician journal
- Vitamin B12 and Folate at Lab Tests Online
- Cyanocobalamin at the US National Library of Medicine Medical Subject Headings (MeSH)
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||