Universal health care
>90% health insurance coverage, and
>90% skilled birth attendance.
Universal health care, sometimes referred to as universal health coverage, universal coverage, or universal care, usually refers to a health care system which provides health care and financial protection to all citizens of a particular country. It is organized around providing a specified package of benefits to all members of a society with the end goal of providing financial risk protection, improved access to health services, and improved health outcomes.[2] Universal health care is not a one-size-fits-all concept and does not imply coverage for all people for everything. Universal health care can be determined by three critical dimensions: who is covered, what services are covered, and how much of the cost is covered.[2]
The health policy framework is of central importance. Thus, in the development of universal health systems, it is appropriate to recognize "healthy public policy" (Health in All Policies) as the overarching policy framework, with public health, primary health care and community services as the cross-cutting framework for all health and health-related services operating across the spectrum from primary prevention to long term care and end-stage conditions. Although this perspective is both logical and well grounded in the social ecological model, the reality is different in most settings, and there is room for improvement everywhere.[3]
History
New Zealand created a universal health care system in a series of steps from 1939 to 1941.[4][5] On July 5, 1948, the United Kingdom implemented its universal National Health Service. Universal health care was next introduced in the Nordic countries of Sweden (1955),[6] Iceland (1956),[7] Norway (1956),[8] Denmark (1961),[9] and Finland (1964).[10] Universal health insurance was then implemented in Japan (1961), Saskatchewan (1962) followed by the rest of Canada (1968–1972).[4][11] The Soviet Union extended universal health care to its rural residents in 1969.[4][12] Universal health insurance was implemented twice in Australia (1974 and 1984). Universal national health services were then introduced in the Southern European countries of Italy (1978), Portugal (1979), Greece (1983), and Spain (1986), followed by the Asian countries of South Korea (1989), Taiwan (1995), and Israel (1995). From the 1970s to 1990s, the Western European countries of Austria, Belgium, France, Germany,[13] and Luxembourg expanded their social health insurance systems to provide universal or nearly universal coverage, as did the Netherlands (1986 and 2006) and Switzerland (1996).
Funding models
Universal health care in most countries has been achieved by a mixed model of funding. General taxation revenue is the primary source of funding, but in many countries it is supplemented by specific levies (which may be charged to the individual and/or an employer) or with the option of private payments (either direct or via optional insurance) for services beyond those covered by the public system.
Almost all European systems are financed through a mix of public and private contributions.[14] The majority of universal health care systems are funded primarily by tax revenue (e.g. Portugal[14] Spain, Denmark, and Sweden). Some nations, such as Germany, France[15] and Japan[16] employ a multi-payer system in which health care is funded by private and public contributions. However, much of the non-government funding is by contributions by employers and employees to regulated non-profit sickness funds. These contributions are compulsory and defined according to law.
A distinction is also made between municipal and national healthcare funding. For example, one model is that the bulk of the healthcare is funded by the municipality, speciality healthcare is provided and possibly funded by a larger entity, such as a municipal co-operation board or the state, and the medications are paid by a state agency.
Universal health care systems are modestly redistributive. Progressivity of health care financing has limited implications for overall income inequality.[17]
Compulsory insurance
This is usually enforced via legislation requiring residents to purchase insurance, but sometimes, in effect, the government provides the insurance. Sometimes there may be a choice of multiple public and private funds providing a standard service (as in Germany) or sometimes just a single public fund (as in Canada). The Swiss Healthcare system and US Patient Protection and Affordable Care Act are based on compulsory insurance.[18][19]
In some European countries where there's private insurance and universal health care, such as Germany, Belgium, and the Netherlands, the problem of adverse selection (see Private insurance below) is overcome using a risk compensation pool to equalize, as far as possible, the risks between funds. Thus a fund with a predominantly healthy, younger population has to pay into a compensation pool and a fund with an older and predominantly less healthy population would receive funds from the pool. In this way, sickness funds compete on price, and there is no advantage to eliminate people with higher risks because they are compensated for by means of risk-adjusted capitation payments. Funds are not allowed to pick and choose their policyholders or deny coverage but then mainly compete on price and service. In some countries, the basic coverage level is set by the government and cannot be modified.[20]
Ireland at one time had a "community rating" system through VHI, effectively a single-payer or common risk pool. The government later opened VHI to competition but without a compensation pool. This resulted in foreign insurance companies entering the Irish market and offering cheap health insurance to relatively healthy segments of the market, which then made higher profits at VHI's expense. The government later reintroduced community rating through a pooling arrangement and at least one main major insurance company, BUPA, then withdrew from the Irish market.
Among the potential solutions posited by economists are single payer systems as well as other methods of ensuring that health insurance is universal, such as by requiring all citizens to purchase insurance and limiting the ability of insurance companies to deny insurance to individuals or vary price between individuals.[21][22]
Single payer
Single-payer health care is a system in which the government, rather than private insurers, pays for all health care costs.[23] Single-payer systems may contract for healthcare services from private organizations (as is the case in Canada) or may own and employ healthcare resources and personnel (as is the case in the United Kingdom). The term "single-payer" thus describes only the funding mechanism and refers to health care financed by a single public body from a single fund and does not specify the type of delivery, or for whom doctors work. Although the fund holder is usually the state, some forms of single-payer use a mixed public-private system.
Tax-based financing
In tax-based financing, individuals contribute to the provision of health services through various taxes. These are typically pooled across the whole population, unless local governments raise and retain tax revenues. Some countries (notably the United Kingdom, Canada, Ireland, Australia, New Zealand, Italy, Spain, Portugal, Greece and the Nordic countries) choose to fund health care directly from taxation alone. Other countries with insurance-based systems effectively meet the cost of insuring those unable to insure themselves via social security arrangements funded from taxation, either by directly paying their medical bills or by paying for insurance premiums for those affected.
Social health insurance
In social health insurance, contributions from workers, the self-employed, enterprises and government are pooled into a single or multiple funds on a compulsory basis. These funds typically contract with a mix of public and private providers for the provision of a specified benefit package. Preventive and public health care may be provided by these funds or responsibility kept solely by the Ministry of Health. Within social health insurance, a number of functions may be executed by parastatal or non-governmental sickness funds or in a few cases by private health insurance companies.
Private insurance
In private health insurance, premiums are paid directly from employers, associations, individuals and families to insurance companies, which pool risks across their membership base. Private insurance includes policies sold by commercial for profit firms, non-profit companies, and community health insurers. Generally, private insurance is voluntary, in contrast to social insurance programs, which tend to be compulsory.[24]
In some countries with universal coverage, private insurance often excludes many health conditions which are expensive and which the state health care system can provide. For example, in the United Kingdom, one of the largest private health care providers is BUPA, which has a long list of general exclusions even in its highest coverage policy,[25] most of which are routinely provided by the National Health Service. In the United States, dialysis treatment for end stage renal failure is generally paid for by government and not by the insurance industry. Persons with privatized Medicare (Medicare Advantage) are the exception and must get their dialysis paid through their insurance company, but persons with end stage renal failure generally cannot buy Medicare Advantage plans.[26]
The Planning Commission of India has also suggested that the country should embrace insurance to achieve universal health coverage.[27] General tax is currently used to meet the essential health requirements of all people.
Community-based health insurance
A particular form of private health insurance that has often emerged in environments where financial risk protection mechanisms only have a limited impact is community-based health insurance. Contributions are not risk-related, and there is generally a high level of community involvement in the running of such schemes.
Implementation and comparisons

Universal health care systems vary according to the degree of government involvement in providing care and/or health insurance. In some countries, such as the UK, Spain, Italy, Australia and the Nordic countries, the government has a high degree of involvement in the commissioning or delivery of health care services and access is based on residence rights, not on the purchase of insurance. Others have a much more pluralistic delivery system, based on obligatory health with contributory insurance rates related to salaries or income and usually funded by employers and beneficiaries jointly.
Sometimes, the health funds are derived from a mixture of insurance premiums, salary related mandatory contributions by employees and/or employers to regulated sickness funds, and by government taxes. These insurance based systems tend to reimburse private or public medical providers, often at heavily regulated rates, through mutual or publicly owned medical insurers. A few countries, such as the Netherlands and Switzerland, operate via privately owned but heavily regulated private insurers, which are not allowed to make a profit from the mandatory element of insurance but can profit by selling supplemental insurance.
Universal health care is a broad concept that has been implemented in several ways. The common denominator for all such programs is some form of government action aimed at extending access to health care as widely as possible and setting minimum standards. Most implement universal health care through legislation, regulation and taxation. Legislation and regulation direct what care must be provided, to whom, and on what basis. Usually, some costs are borne by the patient at the time of consumption, but the bulk of costs come from a combination of compulsory insurance and tax revenues. Some programs are paid for entirely out of tax revenues. In others, tax revenues are used either to fund insurance for the very poor or for those needing long-term chronic care.
The United Kingdom National Audit Office in 2003 published an international comparison of ten different health care systems in ten developed countries, nine universal systems against one non-universal system (the United States), and their relative costs and key health outcomes.[28] A wider international comparison of 16 countries, each with universal health care, was published by the World Health Organization in 2004.[29] In some cases, government involvement also includes directly managing the health care system, but many countries use mixed public-private systems to deliver universal health care.
See also
- Health care reform debate in the United States
- Health insurance cooperative
- Health system
- List of countries by health insurance coverage
- National health insurance
- Primary health care
- Public health
- Publicly funded health care
- Right to health
- Single-payer health care
- Socialized medicine
- Two-tier health care
Notes and references
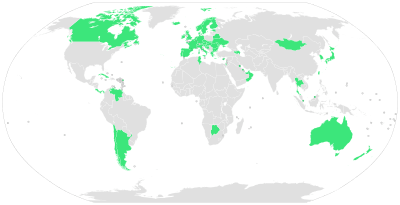
- ↑ Stuckler, David; Feigl, Andrea B.; Basu, Sanjay; McKee, Martin (November 2010). "The political economy of universal health coverage. Background paper for the First Global Symposium on Health Systems Research, 16–19 November 2010, Montreaux, Switzerland" (PDF). Pacific Health Summit. Seattle: National Bureau of Asian Research. p. 16.
Figure 2. Global Prevalence of Universal Health Care in 2009; 58 countries: Andorra, Antigua, Argentina, Armenia, Australia, Austria, Azerbaijan, Bahrain, Belarus, Belgium, Bosnia and Herzegovina, Botswana, Brunei Darussalam, Bulgaria, Canada, Chile, Costa Rica, Croatia, Cuba, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Israel, Italy, Japan, Kuwait, Luxembourg, Moldova, Mongolia, Netherlands, New Zealand, Norway, Oman, Panama, Portugal, Romania, Singapore, Slovakia, Slovenia, South Korea, Spain, Sweden, Switzerland, Taiwan, Thailand, Tunisia, UAE, Ukraine, United Kingdom, Venezuela.
- ↑ 2.0 2.1 World Health Organization (November 22, 2010). "The world health report: health systems financing: the path to universal coverage". Geneva: World Health Organization. ISBN 978-92-4-156402-1. Retrieved April 11, 2012.
- ↑ White F. Primary health care and public health: foundations of universal health systems. Med Princ Pract 2015;24:103-116. doi:10.1159/000370197
- ↑ 4.0 4.1 4.2 Abel-Smith, Brian (1987). "Social welfare; Social security; Benefits in kind; National health schemes". The new Encyclopaedia Britannica (15th ed.). Chicago: Encyclopaedia Britannica. ISBN 0-85229-443-3. Retrieved September 30, 2013.
- ↑ Richards, Raymond (1993). "Two Social Security Acts". Closing the door to destitution: the shaping of the Social Security Acts of the United States and New Zealand. University Park: Pennsylvania State University Press. p. 14. ISBN 0-271-01061-6. Retrieved March 11, 2013.
Mein Smith, Philippa (2012). "Making New Zealand 1930–1949". A concise history of New Zealand (2nd ed.). Cambridge: Cambridge University Press. pp. 164–165. ISBN 978-1-107-40217-1. Retrieved March 11, 2013. - ↑ Serner, Uncas (1980). "Swedish health legislation: milestones in reorganisation since 1945". In Heidenheimer, Arnold J.; Elvander, Nils; Hultén, Charly. The shaping of the Swedish health system. New York: St. Martin's Press. p. 103. ISBN 0-312-71627-3.
Universal and comprehensive health insurance was debated at intervals all through the Second World War, and in 1946 such a bill was voted in Parliament. For financial and other reasons, its promulgation was delayed until 1955, at which time coverage was extended to include drugs and sickness compensation, as well.
- ↑ Kuhnle, Stein; Hort, Sven E.O. (September 1, 2004). "The developmental welfare state in Scandinavia: lessons to the developing world". Geneva: United Nations Research Institute for Social Development. p. 7. Retrieved March 11, 2013.
- ↑ Evang, Karl (1970). Health services in Norway. English version by Dorothy Burton Skårdal (3rd ed.). Oslo: Norwegian Joint Committee on International Social Policy. p. 23. OCLC 141033.
Since 2 July 1956 the entire population of Norway has been included under the obligatory health national insurance program.
- ↑ Gannik, Dorte; Holst, Erik; Wagner, Mardsen (1976). "Primary health care". The national health system in Denmark. Bethesda: National Institutes of Health. pp. 43–44. Retrieved March 11, 2013.
- ↑ Alestalo, Matti; Uusitalo, Hannu (1987). "Finland". In Flora, Peter. Growth to limits: the Western European welfare states since World War II, Vol. 4 Appendix (synopses, bibliographies, tables). Berlin: Walter de Gruyter. pp. 137–140. ISBN 3-11-011133-0. Retrieved March 11, 2013.
- ↑ Taylor, Malcolm G. (1990). "Saskatchewan medical care insurance". Insuring national health care: the Canadian experience. Chapel Hill: University of North Carolina Press. pp. 96–130. ISBN 0-8078-1934-4.
Maioni, Antonia (1998). "The 1960s: the political battle". Parting at the crossroads: the emergence of health insurance in the United States and Canada. Princeton: Princeton University Press. pp. 121–122. ISBN 0-691-05796-6. Retrieved September 30, 2013. - ↑ Kaser, Michael (1976). "The USSR". Health care in the Soviet Union and Eastern Europe. Boulder, Colo.: Westview Press. pp. 38–39, 43. ISBN 0-89158-604-0.
Roemer, Milton Irwin (1993). "Social security for medical care". National health systems of the world: Volume II: The issues. Oxford: Oxford University Press. p. 94. ISBN 0-19-507845-4. Retrieved September 30, 2013.
Denisova, Liubov N. (2010). "Protection of childhood and motherhood in the countryside". In Mukhina, Irina. Rural women in the Soviet Union and post-Soviet Russia. New York: Routledge. p. 167. ISBN 0-203-84684-2. Retrieved September 30, 2013. - ↑ Bärnighausen, Till; Sauerborn, Rainer (May 2002). "One hundred and eighteen years of the German health insurance system: are there any lessons for middle- and low-income countries?". Social Science & Medicine 54 (10): 1559–1587. doi:10.1016/S0277-9536(01)00137-X. PMID 12061488.
Busse, Reinhard; Riesberg, Annette (2004). "Germany" (PDF). Health Care Systems in Transition (Copenhagen: WHO Regional Office for Europe, European Observatory on Health Systems) 6 (9). ISSN 1020-9077. Retrieved October 8, 2013.
Carrin, Guy; James, Chris (January 2005). "Social health insurance: key factors affecting the transition towards universal coverage" (PDF). International Social Security Review 58 (1): 45–64. doi:10.1111/j.1468-246X.2005.00209.x. Retrieved October 8, 2013.
Hassenteufel, Patrick; Palier, Bruno (December 2007). "Towards neo-Bismarckian health care states? Comparing health insurance reforms in Bismarckian welfare systems" (PDF). Social Policy & Administration 41 (6): 574–596. doi:10.1111/j.1467-9515.2007.00573.x. Retrieved October 8, 2013.
Green, David; Irvine, Benedict; Clarke, Emily; Bidgood, Elliot (January 23, 2013). "Healthcare systems: Germany" (PDF). London: Civitas. Retrieved October 8, 2013. - ↑ 14.0 14.1 Bentes, Margarida; Dias, Carlos Matias; Sakellarides, Sakellarides; Bankauskaite, Vaida (2004). "Health care systems in transition: Portugal" (PDF). Copenhagen: WHO Regional Office for Europe on behalf of the European Observatory on Health Systems and Policies. Retrieved August 30, 2006.
- ↑ Physicians for a National Health Program (2004). "International health systems". Chicago: Physicians for a National Health Program. Retrieved November 7, 2006.
- ↑ Chua, Kao-Ping (February 10, 2006). "Single payer 101" (PDF). Sterling, Virginia: American Medical Student Association. Archived from the original (PDF) on October 24, 2006. Retrieved November 7, 2006.
- ↑ Glied, Sherry A. (March 2008). "Health care financing, efficiency, and equity. Working Paper 13881" (PDF). Cambridge, Massachusetts: National Bureau of Economic Research. Retrieved March 25, 2008.
- ↑ Tomasky, Michael (March 21, 2010). "Healthcare vote: Barack Obama passes US health reform by narrow margin". Michael Tomasky's blog (London: The Guardian). Retrieved March 23, 2010.
- ↑ Roy, Avik. Forbes http://www.forbes.com/sites/aroy/2012/12/26/switzerland-a-case-study-in-consumer-driven-health-care/. Missing or empty
|title=(help) - ↑ Varkevisser, Marco; van der Geest, Stéphanie (2002). "Competition among social health insurers: a case study for the Netherlands, Belgium and Germany" (PDF). Research in Healthcare Financial Management 7 (1): 65–84. Retrieved November 28, 2007.
- ↑ Rothschild, Michael; Stiglitz, Joseph (November 1976). "Equilibrium in competitive insurance markets: an essay on the economics of imperfect information" (PDF). Quarterly Journal of Economics 90 (4): 629–649. doi:10.2307/1885326. JSTOR 1885326. Retrieved March 20, 2007.
- ↑ Belli, Paolo (March 2001). "How adverse election affects the health insurance market. Policy Research Working Paper 2574" (PDF). Washington, D.C.: World Bank. Retrieved March 20, 2007.
- ↑ single-payer, Merriam Webster Dictionary
- ↑ World Health Organization (2008). "Health financing mechanisms: private health insurance". Geneva: World Health Organization. Archived from the original on October 9, 2010. Retrieved April 11, 2012.
- ↑ Bupa (2010). "Individuals: Health and life cover: Health care select 1: Key features of this health insurance plan: What's covered? What's not covered?". London: Bupa. Archived from the original on April 9, 2010. Retrieved April 11, 2010.
- ↑ Centers for Medicare & Medicaid Services (2010). "Medicare coverage of kidney dialysis & kidney transplant services" (PDF). Baltimore: Centers for Medicare & Medicaid Services. Retrieved April 11, 2010.
- ↑ Varshney, Vibha; Gupta, Alok; Pallavi, Aparna (September 30, 2012). "Universal health scare". Down To Earth. New Delhi: Society for Environmental Communications. Retrieved September 25, 2012.
- ↑ National Audit Office (February 1, 2003). "International health comparisons: a compendium of published information on healthcare systems, the provision of health care and health achievement in 10 countries". London: National Audit Office. Retrieved November 7, 2007.
- ↑ Grosse-Tebbe, Susanne; Figueras, Josep (2004). "Snapshots of health systems: the state of affairs in 16 countries in summer 2004" (PDF). Copenhagen: World Health Organization on behalf of the European Observatory on Health Systems and Policies. Archived from the original (PDF) on September 26, 2007. Retrieved November 7, 2007.
External links
- Achieving Universal Health Care (July 2011). MEDICC Review: International Journal of Cuban Health and Medicine 13 (3). Theme issue: authors from 19 countries on dimensions of the challenges of providing universal access to health care.
- Catalyzing Change: The System Reform Costs of Universal Health Coverage (November 15, 2010). New York: The Rockefeller Foundation. Report on the feasibility of establishing the systems and institutions needed to pursue UHC.
- Physicians for a National Health Program Chicago: PNHP. A group of physicians and health professionals who support single-payer reform.
- UHC Forward Washington, D.C.: Results for Development Institute. Portal on universal health coverage.