Tumors of the hematopoietic and lymphoid tissues
| Tumors of the hematopoietic and lymphoid tissues | |
|---|---|
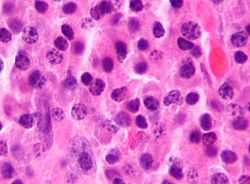 Micrograph of a plasmacytoma, a hematological malignancy | |
| Classification and external resources | |
| ICD-10 | C81-C96 |
| ICD-9 | 200-209 |
| ICD-O | 9590-9999 |
| MeSH | D019337 |
Tumors of the hematopoietic and lymphoid tissues or haematopoietic and lymphoid malignancies are tumors that affect the blood, bone marrow, lymph, and lymphatic system.[1][2] As those elements are all intimately connected through both the circulatory system and the immune system, a disease affecting one will often affect the others as well, making myeloproliferation and lymphoproliferation (and thus the leukemias and the lymphomas) closely related and often overlapping problems.
While uncommon in solid tumors, chromosomal translocations are a common cause of these diseases. This commonly leads to a different approach in diagnosis and treatment of haematological malignancies.
Haematological malignancies are malignant neoplasms ("cancer"), and they are generally treated by specialists in hematology and/or oncology. In some centers "Haematology/oncology" is a single subspecialty of internal medicine while in others they are considered separate divisions (there are also surgical and radiation oncologists). Not all haematological disorders are malignant ("cancerous"); these other blood conditions may also be managed by a hematologist.
Hematological malignancies may derive from either of the two major blood cell lineages: myeloid and lymphoid cell lines. The myeloid cell line normally produces granulocytes, erythrocytes, thrombocytes, macrophages and mast cells; the lymphoid cell line produces B, T, NK and plasma cells. Lymphomas, lymphocytic leukemias, and myeloma are from the lymphoid line, while acute and chronic myelogenous leukemia, myelodysplastic syndromes and myeloproliferative diseases are myeloid in origin.
A subgroup of them are more severe and are known as haematological malignancies (American spelling hematological malignancies) or blood cancer. They may also be referred to as liquid tumors.[3][4]
Diagnosis
For the analysis of a suspected hematological malignancy, a complete blood count and blood film are essential, as malignant cells can show in characteristic ways on light microscopy. When there is lymphadenopathy, a biopsy from a lymph node is generally undertaken surgically. In general, a bone marrow biopsy is part of the "work up" for the analysis of these diseases. All specimens are examined microscopically to determine the nature of the malignancy. A number of these diseases can now be classified by cytogenetics (AML, CML) or immunophenotyping (lymphoma, myeloma, CLL) of the malignant cells.
Classification
Historically, hematological malignancies have been most commonly divided by whether the malignancy is mainly located in the blood (leukemia) or in lymph nodes (lymphomas).
However, the influential WHO Classification (published in 2001) placed a greater emphasis on cell lineage.
Relative proportions of hematological malignancies in the United States[5]
| Type of hematological malignancy | Percentage | Total |
|---|---|---|
| Leukemias | — | 30.4% |
| Acute lymphoblastic leukemia (ALL) | 4.0% | |
| Acute myelogenous leukemia (AML) | 8.7% | |
| Chronic lymphocytic leukemia (CLL) sorted under lymphomas according to current WHO classification; called small lymphocytic lymphoma (SLL) when leukemic cells are absent. |
10.2% | |
| Chronic myelogenous leukemia (CML) | ||
| Acute monocytic leukemia (AMoL) | 0.7% | |
| Other leukemias | 3.1% | |
| Lymphomas | — | 55.6% |
| Hodgkin's lymphomas (all four subtypes) | 7.0% | |
| Non-Hodgkin's lymphomas (all subtypes) | 48.6% | |
| Myelomas | 14.0% | |
| Total | 100% |
Treatment
Treatment can occasionally consist of "watchful waiting" (e.g. in CLL) or symptomatic treatment (e.g. blood transfusions in MDS). The more aggressive forms of disease require treatment with chemotherapy, radiotherapy, immunotherapy and—in some cases—a bone marrow transplant. The use of rituximab has been established for the treatment of B-cell–derived hematologic malignancies, including follicular lymphoma (FL) and diffuse large B-cell lymphoma (DLBCL) [6]
Follow-up
If treatment has been successful ("complete" or "partial remission"), a person is generally followed up at regular intervals to detect recurrence and monitor for "secondary malignancy" (an uncommon side-effect of some chemotherapy and radiotherapy regimens—the appearance of another form of cancer). In the follow-up, which should be done at pre-determined regular intervals, general anamnesis is combined with complete blood count and determination of lactate dehydrogenase or thymidine kinase in serum.
Epidemiology
Taken together, haematological malignancies account for 9.5% of new cancer diagnoses in the United States[7] and 30,000 patients in the UK are diagnosed each year.[8] Within this category, lymphomas are more common than leukemias.
See also
References
- ↑ Vardiman, JW; Thiele, J; Arber, DA; Brunning, RD; Borowitz, MJ; Porwit, A; Harris, NL; Le Beau, MM; Hellström-Lindberg, E; Tefferi, A; Bloomfield, CD (30 July 2009). "The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes.". Blood 114 (5): 937–51. doi:10.1182/blood-2009-03-209262. PMID 19357394.
- ↑ World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 5.13. ISBN 9283204298.
- ↑ Juo, Pei-Show (2001). Concise Dictionary of Biomedicine and Molecular Biology. (2nd ed. ed.). Hoboken: CRC Press. p. 653. ISBN 9781420041309.
- ↑ Cancer Rehabilitation Medicine Quick Reference (RMQR). New York: Demos Medical Publishing. 2013. p. 26. ISBN 9781617050008.
- ↑ Horner MJ, Ries LAG, Krapcho M, Neyman N, et al. (eds). "SEER Cancer Statistics Review, 1975–2006". Surveillance Epidemiology and End Results (SEER). Bethesda, MD: National Cancer Institute. Retrieved 3 November 2009.
Table 1.4: Age-Adjusted SEER Incidence and U.S. Death Rates and 5-Year Relative Survival Rates By Primary Cancer Site, Sex and Time Period
- ↑ "The Clinical and Economic Value of Rituximab for the Treatment of Hematologic Malignancies". Contemporary Oncology. Retrieved 14 September 2011.
- ↑ "Facts & Statistics". The Leukemia and Lymphoma Society. Retrieved 3 November 2009.
- ↑ "Facts about blood cancers". Leukaemia & Lymphoma Research. Retrieved 24 September 2013.
| ||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||