Timeline of tuberous sclerosis

The history of tuberous sclerosis (TSC) research spans less than 200 years. TSC is a rare, multi-system genetic disease that can cause benign tumours to grow on the brain or other vital organs such as the kidneys, heart, eyes, lungs, and skin. A combination of symptoms may include seizures, developmental delay, behavioural problems and skin abnormalities, as well as lung and kidney disease. TSC is caused by mutations on either of two genes, TSC1 and TSC2, which encode for the proteins hamartin and tuberin respectively. These proteins act as tumour growth suppressors and regulate cell proliferation and differentiation.[1] Originally regarded as a rare pathological curiosity, it is now an important focus of research into tumour formation and suppression.
The history of TSC research is commonly divided into four periods.[2] In the late 19th century, notable physicians working in European teaching hospitals first described the cortical and dermatological manifestations; these early researchers have been awarded with eponyms such as "Bourneville's disease"[3] and "Pringle's adenoma sebaceum".[4] At the start of the 20th century, these symptoms were recognised as belonging to a single medical condition. Further organ involvement was discovered, along with a realisation that the condition was highly variable in its severity. The late 20th century saw great improvements in cranial imaging techniques and the discovery of the two genes. Finally, the start of the 21st century saw the beginning of a molecular understanding of the illness, along with possible non-surgical therapeutic treatments.
19th century
- 1835
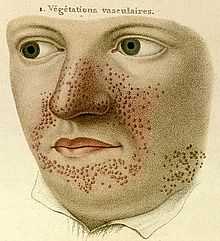
- French dermatologist Pierre François Olive Rayer published an atlas of skin diseases. It contains 22 large coloured plates with 400 figures presented in a systematic order. On page 20, fig. 1 is a drawing that is regarded as the earliest description of tuberous sclerosis.[5] Entitled "végétations vasculaires", Rayer noted these were "small vascular, of papulous appearance, widespread growths distributed on the nose and around the mouth".[6] No mention was made of any medical condition associated with the skin disorder.
- 1850
- English dermatologists Thomas Addison and William Gull described, in Guy's Hospital Reports, the case of a four-year-old girl with a "peculiar eruption extending across the nose and slightly affecting both cheeks", which they called "vitiligoidea tuberosa".[7]
- 1862
- German physician Friedrich Daniel von Recklinghausen, who was working as an assistant to Rudolf Virchow in the Institute for Pathological Anatomy in Berlin,[8] presented a case to the city's Obstetrical Society.[9] The heart of an infant who "died after taking a few breaths" had several tumours. He called these tumours "myomata", one of which was the "size of a pigeon's egg".[7] He also noted the brain had "a great number of scleroses".[5] These were almost certainly the cardiac rhabdomyomas and cortical tubers of tuberous sclerosis. He failed to recognise a distinct disease, regarding it as a pathological-anatomical curiosity.[10] Von Recklinghausen's name would instead become associated with neurofibromatosis after a classic paper in 1881.[8]
- 1864
- German pathologist Rudolf Virchow published a three-volume work on tumours that described a child with cerebral tuberous sclerosis and rhabdomyoma of the heart. His description contained the first hint that this may be an inherited disease: the child's sister had died of a cerebral tumour.[11]
- 1880
- French neurologist Désiré-Magloire Bourneville had a chance encounter with the disease that would bear his name. He was working as an unofficial assistant to Jean Martin Charcot at La Salpêtrière.[10] While substituting for his teacher, Louis J.F. Delasiauve,[12] he attended to Marie, a 15-year-old girl with psychomotor retardation, epilepsy and a "confluent vascular-papulous eruption of the nose, the cheeks and forehead". She had a history of seizures since infancy and was taken to the children's hospital aged three and declared a hopeless case. She had learning difficulties and could neither walk nor talk. While under Bourneville's care, Marie had an ever increasing number of seizures, which came in clusters. She was treated with quinquina, bromide of camphor, amyl nitrite, and the application of leeches behind the ears. On 7 May 1879 Marie died in her hospital bed. The post-mortem examination disclosed hard, dense tubers in the cerebral convolutions, which Bourneville named Sclérose tubéreuse des circonvolutions cérébrales. He concluded they were the source (focus) of her seizures. In addition, whitish hard masses, one "the size of a walnut", were found in both kidneys.[13]
- 1881
- German physician Hartdegen described the case of a two-day-old baby who died in status epilepticus. Post-mortem examination revealed small tumours in the lateral ventricles of the brain and areas of cortical sclerosis, which he called "glioma gangliocellulare cerebri congenitum".[14][15]

- 1881
- Bourneville and Édouard Brissaud examined a four-year-old boy at La Bicêtre. As before, this patient had cortical tubers, epilepsy and learning difficulties. In addition he had a heart murmur and, on post-mortem examination, had tiny hard tumours in the ventricle walls in the brain (subependymal nodules) and small tumours in the kidneys (angiomyolipomas).[16]
- 1885
- French physicians Félix Balzer and Pierre Eugène Ménétrier reported a case of "adénomes sébacés de la face et du cuir" (adenoma of the sebaceous glands of the face and scalp).[17] The term has since proved to be incorrect as they are neither adenoma nor derived from sebaceous glands. The papular rash is now known as facial angiofibroma.[18]
- 1885
- French dermatologists François Henri Hallopeau and Émile Leredde published a case of adenoma sebaceum that was of a hard and fibrous nature. They first described the shagreen plaques and later would note an association between the facial rash and epilepsy.[7][19]
- 1890
- Scottish dermatologist John James Pringle, working in London, described a 25-year-old woman with subnormal intelligence, rough lesions on the arms and legs, and a papular facial rash. Pringle brought attention to five previous reports, two of which were unpublished.[20] Pringle's adenoma sebaceum would become a common eponym for the facial rash.
Early 20th century

.jpg)
- 1901
- Italian physician GB Pellizzi studied the pathology of the cerebral lesions. He noted their dysplastic nature, the cortical heterotopia and defective myelination. Pellizzi classified the tubers into type 1 (smooth surface) and type 2 (with central depressions).[21][22]
- 1903
- German physician Richard Kothe described periungual fibromas, which were later rediscovered by the Dutch physician Johannes Koenen in 1932 (known as Koenen's tumours).[23]
- 1906
- Australian neurologist Alfred Walter Campbell, working in England, considered the lesions in the brain, skin, heart and kidney to be caused by one disease. He also first described the pathology in the eye. His review of 20 reported cases led him to suggest a diagnostic triad of symptoms that is more commonly attributed to Vogt.[24]
- 1908
- German paediatric neurologist Heinrich Vogt established the diagnostic criteria for TSC, firmly associating the facial rash with the neurological consequences of the cortical tubers.[25][26] Vogt's triad of epilepsy, idiocy, and adenoma sebaceum held for 60 years until research by Manuel Gómez discovered that fewer than a third of patients with TSC had all three symptoms.[5]
- 1910
- J. Kirpicznick was first to recognise that TSC was a genetic condition. He described cases of identical and fraternal twins and also one family with three successive generations affected.[27]
- 1911
- Edward Sherlock, barrister-at-law and lecturer in biology, reported nine cases in his book on the "feeble-minded". He coined the term epiloia, a portmanteau of epilepsy and anoia (mindless).[28] The word is no longer widely used as a synonym for TSC. The geneticist Robert James Gorlin suggested in 1981 that it could be a useful acronym for epilepsy, low intelligence, and adenoma sebaceum.[29]
- 1913
- H. Berg is credited with first stating that TSC was a hereditary disorder, noting its transmission through two or three generations.[30]
- 1914
- P. Schuster described a patient with adenoma sebaceum and epilepsy but of normal intelligence.[7] This reduced phenotypic expression is called a forme fruste.[31]
- 1918
- French physician René Lutembacher published the first report of cystic lung disease in a patient with TSC. The 36-year-old woman died from bilateral pneumothoraces. Lutembacher believed the cysts and nodules to be metastases from a renal fibrosarcoma. This complication, which only affects women, is now known as lymphangioleiomyomatosis (LAM).[32][33]
- 1920
- Dutch ophthalmologist Jan van der Hoeve described the retinal hamartomas (phakoma). He grouped both TSC and neurofibromatosis together as "phakomatoses" (later called neurocutaneous syndromes).[34]
- 1924
- H. Marcus noted that characteristic features of TSC such as intracranial calcifications were visible on x-ray.[35]
Mid-20th century
- 1932
- MacDonald Critchley and Charles J.C. Earl studied 29 patients with TSC who were in mental institutions. They described behaviour—unusual hand movements, bizarre attitudes and repetitive movements (stereotypies)—that today would be recognised as autistic. However it would be 11 years before Leo Kanner suggested the term "autism". They also noticed the associated white spots on the skin (hypomelanic macules).[36]
- 1934
- N.J. Berkwitz and L.G. Rigler showed it was possible to diagnose tuberous sclerosis using pneumoencephalography to highlight non-calcified subependymal nodules. These resembled "the wax drippings of a burning candle" on the lateral ventricles.[37]
- 1942
- Sylvan E. Moolten proposed "the tuberous sclerosis complex", which is now the preferred name. This recognises the multi-organ nature of the disease. Moolten introduced three words to describe its pathology: "the basic lesion is hamartial, becoming in turn tumor-like (hamartoma) or truly neoplastic (hamartoblastoma)."[38]
- 1954
- Norwegian pathologist Reidar Eker bred a line of Wistar rats predisposed to renal adenomas. The Eker rat became an important model of dominantly inherited cancer.[39]
- 1966
- Phanor Perot and Bryce Weir pioneered surgical intervention for epilepsy in TSC. Of the seven patients who underwent cortical tuber resection, two became seizure-free. Prior to this, only four patients had ever been surgically treated for epilepsy in TSC.[40]
- 1967
- J.C. Lagos and Manuel Rodríguez Gómez reviewed 71 TSC cases and found that 38% of patients have normal intelligence.[14][41]
- 1971
- American geneticist Alfred Knudson developed his "two hit" hypothesis to explain the formation of retinoblastoma in both children and adults. The children had a congenital germline mutation which was combined with an early lifetime somatic mutation to cause a tumour. This model applies to many conditions involving tumour suppressor genes such as TSC.[42] In the 1980s, Knudson's studies on the Eker rat strengthened this hypothesis.[43]
- 1975
- Giuseppe Pampiglione and E. Pugh, in a letter to The Lancet, noted that up to 69% of patients presented with infantile spasms.[44]
- 1975
- Riemann first used ultrasound to examine TSC-affected kidneys in the case of a 35-year-old woman with chronic renal failure.[45]
Late 20th century

- 1976
- Cranial computed tomography (CT, invented 1972) proved to be an excellent tool for diagnosing cerebral neoplasms in children, including those found in tuberous sclerosis.[46]
- 1979
- Manuel Gómez published a monograph: "Tuberous Sclerosis" that remained the standard textbook for three editions over two decades. The book described the full clinical spectrum of TSC for the first time and established a new set of diagnostic criteria to replace the Vogt triad.[14][47]
- 1982
- Kenneth Arndt successfully treated facial angiofibroma with an argon laser.[48]
- 1983
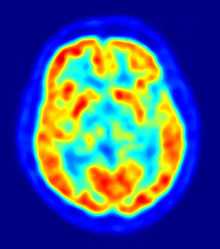
- Positron emission tomography (PET, invented 1981) was compared to electroencephalography (EEG) and CT. It was found to be capable of locating epileptogenic cortical tubers that would otherwise have been missed.[49]
- 1984
- The cluster of infantile spasms in TSC was discovered to be preceded by a focal EEG discharge.[50]
- 1985
- Magnetic resonance imaging (MRI, invented 1980) was first used in TSC to identify affected regions in the brain of a girl with tuberous sclerosis.[51]
- 1987
- MR was judged superior to CT imaging for both sensitivity and specificity. In a study of fifteen patients, it identified subependymal nodules projecting into the lateral ventricles in twelve patients, distortion of the normal cortical architecture in ten patients (corresponding to cortical tubers), dilated ventricles in five patients, and distinguished a known astrocytoma from benign subependymal nodules in one patient.[52]
- 1987
- MR imaging was found to be capable of predicting the clinical severity of the disease (epilepsy and developmental delay). A study of 25 patients found a correlation with the number of cortical tubers identified. In contrast, CT was not a useful predictor, but was superior at identifying calcified lesions.[53]
- 1987
- Linkage analysis on 19 families with TSC located a probable gene on chromosome 9.[54]
- 1988
- Cortical tubers found on MR imaging corresponded exactly to the location of persistent EEG foci, in a study of six children with TSC. In particular, frontal cortical tubers were associated with more intractable seizures.[55]
- 1990
- Vigabatrin was found to be a highly effective antiepileptic treatment for infantile spasms, particularly in children with TSC.[56] Following the discovery in 1997 of severe persistent visual field constriction as a possible side-effect, vigabatrin monotherapy is now largely restricted to this patient group.[57]
- 1992
- Linkage analysis located a second gene to chromosome 16p13.3, close to the polycystic kidney disease type 1 (PKD1) gene.[58]
- 1993
- The European Chromosome 16 Tuberous Sclerosis Consortium announced the cloning of TSC2; its product is called tuberin.[59]
- 1994
- The Eker rat was discovered to be an animal model for tuberous sclerosis; it has a mutation in the rat-equivalent of the TSC2 gene.[60]
- 1995
- MRI with fluid attenuated inversion recovery (FLAIR) sequences was reported to be significantly better than standard T2-weighted images at highlighting small tubers, especially subcortical ones.[61][62]
- 1997
- The TSC1 Consortium announced the cloning of TSC1; its product is called hamartin.[63]
- 1997
- The PKD1 gene, which leads to autosomal dominant polycystic kidney disease (ADPKD), and the TSC2 gene were discovered to be adjacent on chromosome 16p13.3. A team based at the Institute of Medical Genetics in Wales studied 27 unrelated patients with TSC and renal cystic disease. They concluded that serious renal disease in those with TSC is usually due to contiguous gene deletions of TSC2 and PKD1. They also noted that the disease was different (earlier and more severe) than ADPKD and that patients with TSC1 did not suffer significant cystic disease.[64]
- 1997
- Patrick Bolton and Paul Griffiths examined 18 patients with TSC, half of whom had some form of autism. They found a strong association between tubers in the temporal lobes and the patients with autism.[65]
- 1998
- The Tuberous Sclerosis Consensus Conference issued revised diagnosic criteria, which is the current standard.[66]
- 1998
- An Italian team used magnetoencephalography (MEG) to study three patients with TSC and partial epilepsy. Combined with MRI, they were able to study the association between tuberous areas of the brain, neuronal malfunctioning and epileptogenic areas.[67] Later studies would confirm that MEG is superior to EEG in identifying the eliptogenic tuber, which may be a candidate for surgical resection.[68]
21st century
- 2001
- A multi-centre cohort of 224 patients were examined for mutations and disease severity. Those with TSC1 were less severely affected than those with TSC2. They had fewer seizures and less mental impairment. Some symptoms of TSC were rare or absent in those with TSC1. A conclusion is that "both germline and somatic mutations appear to be less common in TSC1 than in TSC2".[69]
- 2002
- Several research groups investigated how the TSC1 and TSC2 gene products (tuberin and hamartin) work together to inhibit mammalian target of rapamycin (mTOR)-mediated downstream signalling. This important pathway regulates cell proliferation and tumour suppression.[70]
- 2002
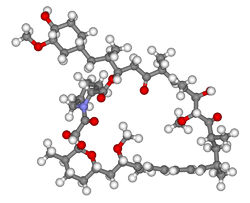
- Treatment with rapamycin (sirolimus) was found to shrink tumours in the Eker rat (TSC2)[71] and mouse (TSC1)[72] models of tuberous sclerosis.
- 2006
- Small trials showed promising results in the use of rapamycin to shrink angiomyolipoma[73] and astrocytomas.[74] Several larger multicentre clinical trials began: lymphangioleiomyomatosis (LAM)[75] and kidney angiomyolipoma (AML)[76] were treated with rapamycin; giant cell astrocytomas were treated with the rapamycin derivative everolimus.[77]
Notes
- ↑ "Tuberous Sclerosis Fact Sheet". NINDS. 11 April 2006. Retrieved 9 January 2007.
- ↑ Rott (2005), page 2 - Introduction.
- ↑ Enersen, Ole Daniel. "Désiré-Magloire Bourneville". Who Named It?. Retrieved 30 April 2007.
- ↑ Enersen, Ole Daniel. "John James Pringle". Who Named It?. Retrieved 30 April 2007.
- ↑ 5.0 5.1 5.2 Curatolo (2003), chapter: "Historical Background".
- ↑ Rayer, Pierre François (1835). Traité des maladies de la peau / atlas (in French). Paris: J.B. Baillière. p. 20. Retrieved 9 December 2006.
- ↑ 7.0 7.1 7.2 7.3 Jay V (2004). "Historical contributions to pediatric pathology: Tuberous Sclerosis". Pediatric and Developmental Pathology 2 (2): 197–8. doi:10.1007/s100249900110. PMID 9949228.
- ↑ 8.0 8.1 Enersen, Ole Daniel. "Friedrich Daniel von Recklinghausen". Who Named It?. Retrieved 10 December 2006.
- ↑ von Recklinghausen, F (1862). "Ein Herz von einem Neugeborene welches mehrere theils nach aussen, theils nach den Höhlen prominirende Tumoren (Myomen) trug". Monatschr Geburtsheilkd (in German) 20: 1–2.(As cited in Curatolo (2003))
- ↑ 10.0 10.1 Jansen F, van Nieuwenhuizen O, van Huffelen A (2004). "Tuberous sclerosis complex and its founders". Journal of Neurology, Neurosurgery and Psychiatry 75 (5): 770. doi:10.1136/jnnp.2003.027524. PMC 1763558. PMID 15090576.
- ↑ Virchow R (1863–7). Die Krankhaften Geschwülste. Vol II. Berlin: August Hirschwald. p. 148. Check date values in:
|date=(help)(As cited in Acierno (1994)) - ↑ Wilkins, Robert H (ed); Brody, Irwin A (ed) (1997). "XXXI Tuberous Sclerosis". Neurological Classics. American Association of Neurological Surgeons. pp. 149–52. ISBN 1-879284-49-9.(contains an abridged translation of Bourneville's 1880 paper)
- ↑ Bourneville D (1880). "Sclérose tubéreuse des circonvolutions cérébrales: Idiotie et épilepsie hemiplégique". Archives de neurologie, Paris (in French) 1: 81–9l. Retrieved 22 August 2009.
- ↑ 14.0 14.1 14.2 Sancak, Özgür (2005). Tuberous Sclerosis Complex: Mutations, Functions and Phenotypes. Stichting Tubereuze Sclerose Nederland. pp. 11–2. ISBN 90-902019-3-9.
- ↑ Hartdegen A (February 1881). "Ein Fall von multipler Verhärtung des Grosshirns nebst histologisch eigenartigen harten Geschwülsten der Seitenventrikel ("Glioma gangliocellulare") bei einem Neugeborenen". European Archives of Psychiatry and Clinical Neuroscience 11 (1): 117–31. doi:10.1007/BF02054825.
- ↑ Bourneville D, Brissaud É (1881). "Encéphalite ou sclérose tubéreuse des circonvolutions cérébrales". Archives de neurologie, Paris 1: 390–412.(As cited in Curatolo (2003))
- ↑ Balzer F, Ménétrier P (1885). "Étude sur un cas d'adénomes sébacés de la face et du cuir". Archives de Physiologie normale et pathologique (série III) 6: 564–76.(As cited in Curatolo (2003))
- ↑ Sanchez N, Wick M, Perry H (1981). "Adenoma sebaceum of Pringle: a clinicopathologic review, with a discussion of related pathologic entities". Journal of Cutaneous Pathology 8 (6): 395–403. doi:10.1111/j.1600-0560.1981.tb01028.x. PMID 6278000.
- ↑ Hallopeau F; Leredde É (1885). "Sur un cas d'adenomes sébacés à forme sclereuse". Ann Dermatol Syph 6: 473–9.(As cited in Curatolo (2003))
- ↑ Pringle, JJ (1890). "A case of congenital adenoma sebaceum". British Journal of Dermatology, Oxford 2: 1–14. Retrieved 22 August 2009.
- ↑ Pellizzi GB (1901). "Contributo allo studio dell'idiozia: rivisita sperimentale di freniatria e medicina legale delle alienazioni mentali". Riv Sper Freniat 27: 265–9.(As cited in Curatolo (2003))
- ↑ Braffman BH, Bilaniuk LT, Naidich TP, Altman NR, Post MJ, Quencer RM, Zimmerman RA, Brody BA (April 1, 1992). "MR imaging of tuberous sclerosis: pathogenesis of this phakomatosis, use of gadopentetate dimeglumine, and literature review". Radiology 183 (1): 227–38. doi:10.1148/radiology.183.1.1549677. PMID 1549677.
- ↑ Kothe R (1903). "Zur Lehre der Talgdrüsengeschwülste". Archives of Dermatology and Syphilis (in German) 68: 273–8.(As cited in Rott (2005))
- ↑ Campbell, AW (1906). "Cerebral sclerosis". Brain 28 (3–4): 382–96. doi:10.1093/brain/28.3-4.367.
- ↑ Enersen, Ole Daniel. "Heinrich Vogt". Who Named It?. Retrieved 11 December 2006.
- ↑ Vogt H (1908). "Zur Diagnostik der tuberösen Sklerose". Zeitschrift für die Erforschung und Behandlung des jugendlichen Schwachsinns auf wissenschaftlicher Grundlage, Jena 2: 1–16.(As cited in Curatolo (2003) and fully cited by Who Named It?)
- ↑ Kirpicznik J (1910). "Ein Fall von Tuberoser Sklerose und gleichzeitigen multiplen Nierengeschwùlsten". Virchow's Archiv für pathologische Anatomie und Physiologie und für klinische Medicin (in German) 202 (3): 258. doi:10.1007/BF01993975.(As cited in Curatolo (2003))
- ↑ Sherlock, Edward Birchall (1911). The Feeble-minded, A Guide to Study and Practice. Macmillan & Co.(As cited in Jay (2004))
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) Tuberous Sclerosis -191100
- ↑ Berg H (1913). "Vererbung der tuberösen Sklerose durch zwei bzw. drei Generationen". Z ges Neurol Psychiatr (in German) 19: 528–39. doi:10.1007/BF02909909.(As cited in Curatolo (2003))
- ↑ Schuster P (1914). "Beiträge zur Klinik der tuberösen Sklerose des Gehirns". Dtsch Z Nervenheilk (in German) 50: 96–133.(As cited in Curatolo (2003))
- ↑ Lutembacher R (1918). "Dysembryomes métatypique des reins. Carcinose submiliaire aigue du poumon avec emphysème généralisé et double pneumothorax". Annals of Medicine (in French) 5: 435–50.(As cited in Curatolo (2003))
- ↑ Abbott GF, Rosado-de-Christenson ML, Frazier AA, Franks TJ, Pugatch RD, Galvin JR. (2005). "From the archives of the AFIP: lymphangioleiomyomatosis: radiologic-pathologic correlation". Radiographics 25 (3): 803–28. doi:10.1148/rg.253055006. PMID 15888627.
- ↑ Van der Hoeve J (1920). "Eye symptoms in tuberous sclerosis of the brain". Trans Ophthalmol Soc UK 40: 329–34.(As cited in Curatolo (2003))
- ↑ Marcus H (1924). Svenska Làk Sallsk Forth.(As cited by Dickerson WW (1945). "Characteristic roentgenographic changes associated with tuberous sclerosis". Archives of Neurology and Psychiatry 53: 199–204. doi:10.1001/archneurpsyc.1945.02300030036005., as cited in Curatolo (2003) and Gómez (1995))
- ↑ Critchley M, Earl CJC (1932). "Tuberose sclerosis and allied conditions". Brain 55 (3): 311–46. doi:10.1093/brain/55.3.311.
- ↑ Berkwitz NJ, Rigler LG (1934). "Tuberous sclerosis diagnosed with cerebral pneumography". Archives of Neurology and Psychiatry 35: 833–8.(As cited in Gómez (1995))
- ↑ Moolten SE (1942). "Hamartial nature of tuberous sclerosis complex and its bearings on the tumor problem: report of a case with tumor anomaly of the kidney and adenoma sebaceum". Arch Intern Med 69: 589–623. doi:10.1001/archinte.1942.00200160040005.
- ↑ Eker R (1954). "Familial renal adenomas in Wistar rats; a preliminary report". Acta Pathologica et Microbiologica Scandinavica 34 (6): 554–62. doi:10.1111/j.1699-0463.1954.tb00301.x. PMID 13206757.(As cited in Yeung (1994))
- ↑ Perot P, Weir B, Rasmussen T (1966). "Tuberous sclerosis. Surgical therapy for seizures". Archives of Neurology 15 (5): 498–506. doi:10.1001/archneur.1966.00470170052005. PMID 5955139.(As cited in Bebin EM, Kelly PJ, Gómez MR (1993). "Surgical treatment for epilepsy in cerebral tuberous sclerosis". Epilepsia 34 (4): 651–7. doi:10.1111/j.1528-1157.1993.tb00442.x. PMID 8330575.)
- ↑ Lagos JC, Gómez MR (1967). "Tuberous sclerosis: reappraisal of a clinical entity". Mayo Clinic Proceedings 42 (1): 26–49. PMID 5297238.(As cited in Curatolo (2003))
- ↑ Knudson AG (April 1971). "Mutation and Cancer: Statistical Study of Retinoblastoma". Proc. Natl. Acad. Sci. U.S.A. 68 (4): 820–3. doi:10.1073/pnas.68.4.820. PMC 389051. PMID 5279523.(As cited in Rott (2005))
- ↑ Yeung R (2004). "Lessons from the Eker rat model: from cage to bedside". Current Molecular Medicine 4 (8): 799–806. doi:10.2174/1566524043359791. PMID 15579026.
- ↑ Pampiglione G, Pugh E (1975). "Letter: Infantile spasms and subsequent appearance of tuberous sclerosis syndrome". Lancet 2 (7943): 1046. doi:10.1016/S0140-6736(75)90343-8. PMID 53537.
- ↑ Riemann JF, Mörl M, Rott HD (1975). "Chronische Niereninsuffizienz bei Morbus Bourneville-Pringle (Chronic renal failure in bourneville-pringle's disease)". Medizinische Klinik (in German) 70 (26): 1128–32. PMID 1223616.(As cited in Rott (2005))
- ↑ Berger PE, Kirks DR, Gilday DL, Fitz CR, Harwood-Nash DC (1976). "Computed tomography in infants and children: intracranial neoplasms". American Journal of Roentgenology 127 (1): 129–37. doi:10.2214/ajr.127.1.129. PMID 180824.
- ↑ Gómez, Manuel R (1979). Tuberous Sclerosis (1st ed.). New York: Raven Press. ISBN 0-89004-313-2.(As cited in Özgür (2005))
- ↑ Arndt KA (1982). "Adenoma sebaceum: successful treatment with the argon laser". Plastic Reconstructive Surgery 70 (1): 91–3. doi:10.1097/00006534-198207000-00021. PMID 7089113.(As cited in Rott (2005))
- ↑ Szelies B, Herholz K, Heiss W et al. (1983). "Hypometabolic cortical lesions in tuberous sclerosis with epilepsy: demonstration by positron emission tomography". Journal of Computer Assisted Tomography 7 (6): 946–53. doi:10.1097/00004728-198312000-00002. PMID 6415136. (As cited in Rott (2005))
- ↑ Dulac O, Lemaitre A, Plouin P (1984). "The Bourneville syndrome: clinical and EEG features of epilepsy in the first year of life". Boll Lega Ital Epil. 45/46: 39–42.(As cited in Curatolo (2003))
- ↑ Kandt RS, Gebarski SS, Goetting MG (1985). "Tuberous sclerosis with cardiogenic cerebral embolism: magnetic resonance imaging". Neurology 35 (8): 1223–5. doi:10.1212/wnl.35.8.1223. PMID 4022361.(As cited in Rott (2005))
- ↑ McMurdo SK Jr, Moore SG et al. (1987). "MR imaging of intracranial tuberous sclerosis". AJR Am J Roentgenol 148 (4): 791–6. doi:10.2214/ajr.148.4.791. PMID 3493666.
- ↑ Roach ES, Williams DP, Laster DW (1987). "Magnetic resonance imaging in tuberous sclerosis". Arch Neurol 44 (3): 301–3. doi:10.1001/archneur.1987.00520150047020. PMID 3827681.(As cited in Curatolo (2003))
- ↑ Fryer AE, Chalmers A, Connor JM et al. (1987). "Evidence that the gene for tuberous sclerosis is on chromosome 9". Lancet 1 (8534): 659–61. doi:10.1016/S0140-6736(87)90416-8. PMID 2882085.
- ↑ Curatolo P, Cusmai R (1988). "Imagerie par résonance magnétique nucléaire dans la maladie de Bourneville: relation avec les données électroencéphalographiques (Magnetic resonance imaging in the Bourneville syndrome: relations with EEG)". Neurophysiologie clinique (in French) 18 (5): 459–67. doi:10.1016/s0987-7053(88)80056-x. PMID 3185465.(As cited in Curatolo (2003))
- ↑ Chiron C, Dulac O, Luna D et al. (1990). "Vigabatrin in infantile spasms". Lancet 335 (8685): 363–4. doi:10.1016/0140-6736(90)90660-W. PMID 1967808.
- ↑ Vigabatrin Paediatric Advisory Group (May 2000). "Guideline for prescribing vigabatrin in children has been revised". BMJ 320 (7246): 1404–5. doi:10.1136/bmj.320.7246.1404. PMC 1118061. PMID 10858057.
- ↑ Kandt RS, Haines JL, Smith M et al. (1992). "Linkage of an important gene locus for tuberous sclerosis to a chromosome 16 marker for polycystic kidney disease". Nature Genetics 2 (1): 37–41. doi:10.1038/ng0992-37. PMID 1303246.
- ↑ European Chromosome 16 Tuberous Sclerosis Consortium (1993). "Identification and characterization of the tuberous sclerosis gene on chromosome 16". Cell 75 (7): 1305–15. doi:10.1016/0092-8674(93)90618-Z. PMID 8269512.(As cited in Rott (2005))
- ↑ Yeung R, Xiao G, Jin F, et all (November 1994). "Predisposition to renal carcinoma in the Eker rat is determined by germ-line mutation of the tuberous sclerosis 2 (TSC2) gene". Proc Natl Acad Sci USA 91 (24): 11413–6. doi:10.1073/pnas.91.24.11413. PMC 45241. PMID 7972075.
- ↑ Maeda M, Tartaro A, Matsuda T, Ishii Y (1995). "Cortical and subcortical tubers in tuberous sclerosis and FLAIR sequence". Journal of Computer Assisted Tomography 19 (4): 660–1. doi:10.1097/00004728-199507000-00033. PMID 7622707.
- ↑ Takanashi J, Sugita K, Fujii K, Niimi H (October 1, 1995). "MR evaluation of tuberous sclerosis: increased sensitivity with fluid-attenuated inversion recovery and relation to severity of seizures and mental retardation". AJNR American Journal of Neuroradiology 16 (9): 1923–8. PMID 8693996.
- ↑ van Slegtenhorst M, de Hoogt R, Hermans C et al. (1997). "Identification of the tuberous sclerosis gene TSC1 on chromosome 9q34". Science 277 (5327): 805–8. doi:10.1126/science.277.5327.805. PMID 9242607.
- ↑ Sampson JR, Maheshwar MM, Aspinwall R et al. (October 1997). "Renal cystic disease in tuberous sclerosis: role of the polycystic kidney disease 1 gene". American Journal of Human Genetics 61 (4): 843–51. doi:10.1086/514888. PMC 1716004. PMID 9382094.
- ↑ Bolton PF, Griffiths PD (1997). "Association of tuberous sclerosis of temporal lobes with autism and atypical autism". Lancet 349 (9049): 392–5. doi:10.1016/S0140-6736(97)80012-8. PMID 9033466.
- ↑ Roach ES, Gómez MR, Northrup H (1998). "Tuberous sclerosis complex consensus conference: revised clinical diagnostic criteria". Journal of Child Neurology 13 (12): 624–8. doi:10.1177/088307389801301206. PMID 9881533.
- ↑ Peresson M, Lopez L, Narici L, Curatolo P (1998). "Magnetic source imaging and reactivity to rhythmical stimulation in tuberous sclerosis". Brain Dev 20 (7): 512–8. doi:10.1016/S0387-7604(98)00034-5. PMID 9840671.
- ↑ Jansen F, Huiskamp G, van Huffelen A, Bourez-Swart M, Boere E, Gebbink T, Vincken K, van Nieuwenhuizen O (2006). "Identification of the epileptogenic tuber in patients with tuberous sclerosis: a comparison of high-resolution EEG and MEG". Epilepsia 47 (1): 108–14. doi:10.1111/j.1528-1167.2006.00373.x. PMID 16417538.
- ↑ Dabora SL, Jozwiak S, Franz DN et al. (January 2001). "Mutational Analysis in a Cohort of 224 Tuberous Sclerosis Patients Indicates Increased Severity of TSC2, Compared with TSC1, Disease in Multiple Organs". The American Journal of Human Genetics 68 (1): 64–80. doi:10.1086/316951. PMC 1234935. PMID 11112665.
- ↑ Tee A, Fingar D, Manning B, Kwiatkowski D, Cantley L, Blenis J (15 October 2005). "Tuberous sclerosis complex-1 and -2 gene products function together to inhibit mammalian target of rapamycin (mTOR)-mediated downstream signaling". Proc Natl Acad Sci USA 99 (21): 13571–6. doi:10.1073/pnas.202476899. PMC 129715. PMID 12271141.
- ↑ Kenerson H, Aicher L, True L, Yeung R (October 15, 2002). "Activated mammalian target of rapamycin pathway in the pathogenesis of tuberous sclerosis complex renal tumors". Cancer Res 62 (20): 5645–50. PMID 12384518.
- ↑ Kwiatkowski D, Zhang H, Bandura J et al. (2002). "A mouse model of TSC1 reveals sex-dependent lethality from liver hemangiomas, and up-regulation of p70S6 kinase activity in Tsc1 null cells". Hum Mol Genet 11 (5): 525–34. doi:10.1093/hmg/11.5.525. PMID 11875047.
- ↑ Wienecke R, Fackler I, Linsenmaier U, Mayer K, Licht T, Kretzler M (September 2006). "Antitumoral activity of rapamycin in renal angiomyolipoma associated with tuberous sclerosis complex". American Journal of Kidney Diseases 48 (3): e27–9. doi:10.1053/j.ajkd.2006.05.018. PMID 16931204.
- ↑ Franz DN, Leonard J, Tudor C et al. (2006). "Rapamycin causes regression of astrocytomas in tuberous sclerosis complex". Annals of Neurology 59 (3): 490–8. doi:10.1002/ana.20784. PMID 16453317.
- ↑ "Multicenter International Lymphangioleiomyomatosis Efficacy of Sirolimus Trial (The MILES Trial)". ClinicalTrials.gov (NIH). 6 January 2007. Retrieved 10 January 2007.
- ↑ "Sirolimus in Treating Patients With Angiomyolipoma of the Kidney". ClinicalTrials.gov (NIH). 21 November 2006. Retrieved 10 January 2007.
- ↑ "Everolimus (RAD001) Therapy of Giant Cell Astrocytoma in Patients With Tuberous Sclerosis Complex". ClinicalTrials.gov (NIH). 13 December 2006. Retrieved 10 January 2007.
References
- Acierno, Louis J (1994). The History of Cardiology. Taylor & Francis. p. 427. ISBN 1-85070-339-6.
- Curatolo, Paolo (Editor) (2003). Tuberous Sclerosis Complex : From Basic Science to Clinical Phenotypes. MacKeith Press. ISBN 1-898683-39-5.
- Gómez MR (1995). "History of the tuberous sclerosis complex". Brain & Development 17 (suppl): 55–7. doi:10.1016/0387-7604(94)00130-8. PMID 8882573.
- Rott HD, Mayer K, Walther B, Wienecke R (2005). "Zur Geschichte der Tuberösen Sklerose (The History of Tuberous Sclerosis)" (PDF) (in German). Tuberöse Sklerose Deutschland e.V. Retrieved 8 January 2007.